预约演示
更新于:2026-08-03
LR1
更新于:2026-08-03
概要
基本信息
非在研机构- |
权益机构- |
最高研发阶段临床前 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |

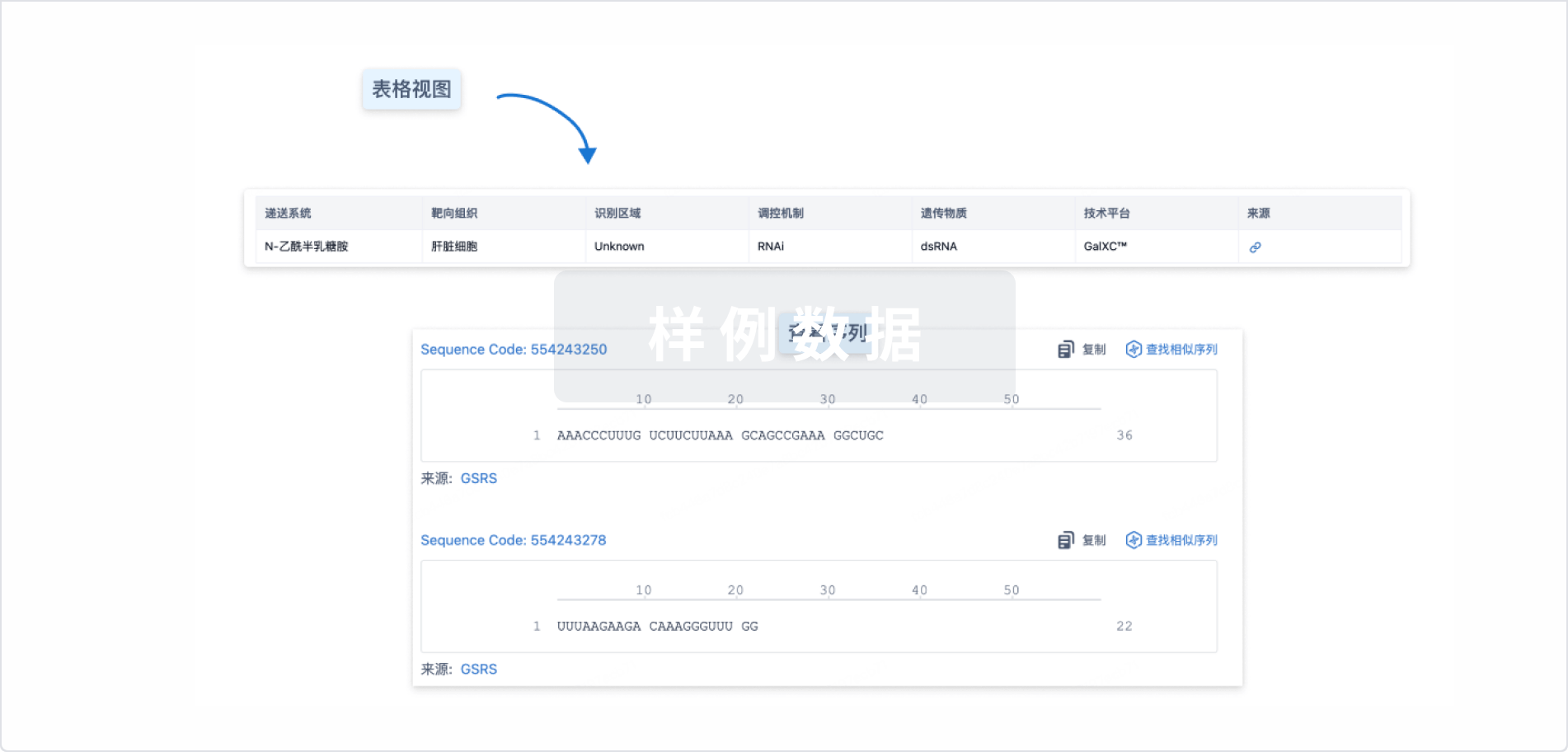
结构/序列
使用我们的RNA技术数据为新药研发加速。
登录
或
关联
100 项与 LR1 相关的临床结果
登录后查看更多信息
100 项与 LR1 相关的转化医学
登录后查看更多信息
100 项与 LR1 相关的专利(医药)
登录后查看更多信息
19
项与 LR1 相关的文献(医药)2021-01-01·Meat science1区 · 农林科学
Effect of long-term dietary probiotic Lactobacillus reuteri 1 or antibiotics on meat quality, muscular amino acids and fatty acids in pigs
1区 · 农林科学
Article
作者: Cui, Yiyan ; Lu, Huijie ; Ma, Xianyong ; Tian, Zhimei ; Wang, Gang
This study investigated effects of 175-d dietary treatment with Lactobacillus reuteri 1 (LR1) or antibiotics (olaquindox and aureomycin) on the longissimus thoracis (LT) of pigs. Results showed that antibiotics decreased pork quality by increasing drip loss, shear force, and altering myofiber characteristics including diameter, cross-sectional area and myosin heavy chain isoforms compared to LR1. Pigs fed antibiotics had lower muscle contents of free glutamic acid, inosinic acid, and higher glutamine compared to pigs fed the controls and LR1 diets (P ≤ .05). Furthermore, antibiotics decreased free isoleucine, leucine, methionine in LT compared to the control (P ≤ .05). Compared to antibiotics, LR1 likely improved protein synthesis by modulating expression of amino acid transport and ribosomal protein S6 kinase 1 (S6K1) genes, and altered fatty acid profile by regulating metabolic pathways. Overall, LR1 improved pork quality compared to antibiotics by decreasing drip loss and shear force, increasing inosinic acid and glutamic acid that may improve flavor, and altering muscle fiber characteristics.
2019-12-01·Microbial pathogenesis3区 · 医学
Probiotic potential of Lactobacillus on the intestinal microflora against Escherichia coli induced mice model through high-throughput sequencing
3区 · 医学
Article
作者: Aoyun Li ; Jiakui Li ; Mudassar Iqbal ; Zhixing Li ; Suolang Sizhu ; Yaping Wang ; Khalid Mehmood ; Yi Lian ; Can Muyou ; Lihong Zhang ; Muhammad Waqas
The aim of this study was to evaluate the antibacterial potential of Lactobacillus screened from Tibetan yaks on clinical symptoms and intestinal microflora in enteroinvasive Escherichia coli (EIEC) induced mice model. In vitro study, Lactobacillus reuteri (LR1) exhibited stronger resistance to acid and bile and inhibited the growth of EIEC than Lactobacillus mucosae (LM1). The mice were randomly divided into four groups i.e. the LR1 group (LR1 1 × 109 CFU/day), LM1 group (LM1 1 × 109 CFU/day), blank control group and control group. Mice in control, LR1, and LM1 groups were challenged with EIEC on day 23. The body weight in the control and LM1 groups were significantly decreased after the infection with EIEC (P < 0.05), whereas the body weight of mice in the LR1 group did not change significantly (P > 0.05). The lowest diarrhea rate was recorded in the LR1 group after infection with EIEC. The results showed that the number of pathogens in the control group was higher than that in the experimental groups. The sequence analysis and OTU classification showed that the duodenum, ileum, and cecum of mice in the LR1 group had the highest number of OTUs compared with other groups. Whereas, the diversity analysis showed that in duodenum, ileum and cecum of mice in the LR1 group had the highest abundance and diversity. The composition of intestinal microbes indicated the presence of high proportions of Firmicutes, Proteobacteria and Bacteroidetes. Heat map analysis indicated high abundance of Bdello vibrio in the duodenum of mice in the LR1 group, while many pathogens were found in the different part of intestines in the control group, such as Streptococcus, Clostridium and Pseudomonas. In conclusion, pre-supplementation of LR1 alleviate the clinical symptoms caused by E. coli, and promote a healthy gut flora.
2019-12-01·Saudi journal of biological sciences3区 · 生物学
Analysis of the protective mechanism of liraglutide on retinopathy based on diabetic mouse model
3区 · 生物学
ArticleOA
作者: Liu, Yahong ; Sun, Ting ; Gao, Lijuan ; Wu, Lingling ; Chen, Fengju ; Cao, Yaohui
In order to study the protection mechanism of liraglutide on the infectious lesion of the retina of type I diabetes, in this experiment, a mouse model of type I diabetes was established by induction with streptozotocin (STZ) and feeding with high-fat and high-sugar diet. After observing the living conditions of the modeled mice and detecting their fasting blood glucose (FBG), it was found that the modeled mice exhibited clinically similar symptoms in patients with type I diabetes, and their FBG was larger than 16.7 mmol/L, indicating that the experimental mouse model was obtained. The mice were divided into groups. The control group was divided into negative control group (A), light positive control group (B), diabetic control group (C), and diabetes care group (D) according to different treatment methods, and the experimental group was divided into treatment group 1 (LR1), treatment group 2 (LR2) and treatment group 3 (LR3) according to different injection doses. The eyes of mice in each group were extracted and retinal tissue sections were made, and the sections were stained with HE. The retinal morphology was observed and it was found that compared with group A, the outer nucleus layer was significantly thinner in group B and C, and the group D was the thinnest. After treatment with liraglutide, the outer nuclear layer of LR1 group and LR2 group LR3 group recovered significantly, indicating that liraglutide had protective effect on type I diabetes and light-induced damage of mouse retinal photoreceptor cells. Immunohistochemistry was used to detect p-Erk1/2 and ASK1 protein contents in retina. It was found that compared with the negative control group and the light control group, p-Erk1/2 protein contents in LR1, LR2 and LR3 groups were significantly increased, showing statistical significance. Compared with the negative control group and the light control group, ASK1 protein content in LR1, LR2 and LR3 groups significantly decreased. This suggested that the protective mechanism of liraglutide on retinopathy was related to up-regulation of antioxidant protein p-Erk1/2 and down-regulation of apoptosis-related protein ASK1, that is to say, the action site of liraglutide may be related to this. Through real-time quantitative detection of the Trx gene expression level in diabetic and photodamaged mice, it was found that compared with the diabetic light group, the Trx expression level in mice treated with liraglutide showed a significant up-regulated trend, suggesting that the protective mechanism of liraglutide on retinopathy was related to the up-regulated expression of antioxidant protein Trx. Therefore, liraglutide has a certain protective effect on diabetic retinal injury, and its mechanism is related to the up-regulation of p-Erk1/2 and Trx antioxidant protein, and the down-regulation of apoptosis-related protein ASK1.
1
项与 LR1 相关的新闻(医药)2023-11-06
SINGAPORE, CAMBRIDGE, Mass. and SHANGHAI, Nov. 6, 2023 /PRNewswire/ -- Lerna Biopharma Pte. Ltd (Lerna Bio) proudly announces the unveiling of its pioneering liver regeneration drug candidate, LR1, at The Liver Meeting in Boston organized by American Association for the Study of Liver Diseases (AASLD) from November 10th to 14th. During this esteemed event, Lerna Bio will present two highly anticipated presentations: "Promoting Liver Regeneration and Protection with LR1: A Novel siRNA Drug" by Dr. Tan Si Hui, Vice President of Biology at Lerna Bio, on November 11th, and an oral report on the Quartz platform, a groundbreaking in vivo target discovery platform for liver diseases, by Dr. Torsten Wuestefeld, Co-founder and Advisor of Lerna Bio, on November 13th.
By targeting liver regeneration, LR1 provides a novel mechanism and innovative solution for patients at risk of liver failure. This first-in-class siRNA drug has demonstrated its potential to sustain and improve liver functions, addressing a critical gap in liver care. The preclinical data, to be presented by Dr. Tan Si Hui, highlights LR1's ability to promote liver regeneration and protect the liver from further deterioration.
Every year, over 2 million lives succumb to liver failure due to liver cirrhosis resulting from chronic liver diseases, making it a leading cause of mortality worldwide. The existing treatment for liver failure patients - liver transplantation - has severe limitations, leaving patients and physicians in search of effective solutions. LR1, a siRNA drug that promotes liver regeneration, holds the promise to transform the landscape of liver disease treatment. With over 100 million cirrhosis patients globally and a rapidly growing population driven by increasing patients with nonalcoholic steatohepatitis (NASH), the need for a breakthrough is more urgent than ever.
Commenting on the potential of LR1, Ms. Kathy He, CEO of Lerna Bio, enthused, "Leveraging liver's innate regenerative capacity to combat liver diseases has been a longstanding aspiration for liver researchers. The unmet needs in this disease area are monumental. By harnessing the power of siRNA and our novel liver regeneration target, LR1 is poised to revolutionize treatment of chronic liver diseases, potentially eliminating the need for transplantation."
Lerna Bio invites attendees of The Liver Meeting to join Dr. Tan Si Hui's presentation on LR1's role in promoting liver regeneration and protection, along with an overview of preclinical data showcasing its therapeutic potential. Additionally, Dr. Torsten Wuestefeld, will present an oral report on November 13th on the Quartz platform – the discovery engine that engendered Lerna Bio's lead target and continues to generate a robust pipeline of new generation targets.
About Lerna Biopharma Pte. Ltd. (Lerna Bio)
Lerna Bio is a global biotech focused on developing first-in-class therapeutics for liver diseases. Leveraging Quartz target discovery platform developed by Torsten Wuestefeld, Lerna Bio combines its in-depth understanding of new biological targets and deep industry experience in nucleic acid medicinal chemistry to develop novel siRNA drugs for diseases with high unmet needs.
Please visit the company website or contact Ms. Melodee Wu [email protected] for more information.
SOURCE Lerna Biopharma Pte. Ltd (Lerna Bio)
100 项与 LR1 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 肝纤维化 | 临床前 | 新加坡 | 2021-11-12 | |
| 肝硬化 | 临床前 | 新加坡 | 2021-11-12 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
| 研究 | 分期 | 人群特征 | 评价人数 | 分组 | 结果 | 评价 | 发布日期 |
|---|
No Data | |||||||
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

芽仔
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用