预约演示
更新于:2025-05-07
C1-INH(MiNA Therapeutics)
更新于:2025-05-07
概要
基本信息
非在研机构- |
权益机构- |
最高研发阶段临床前 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |
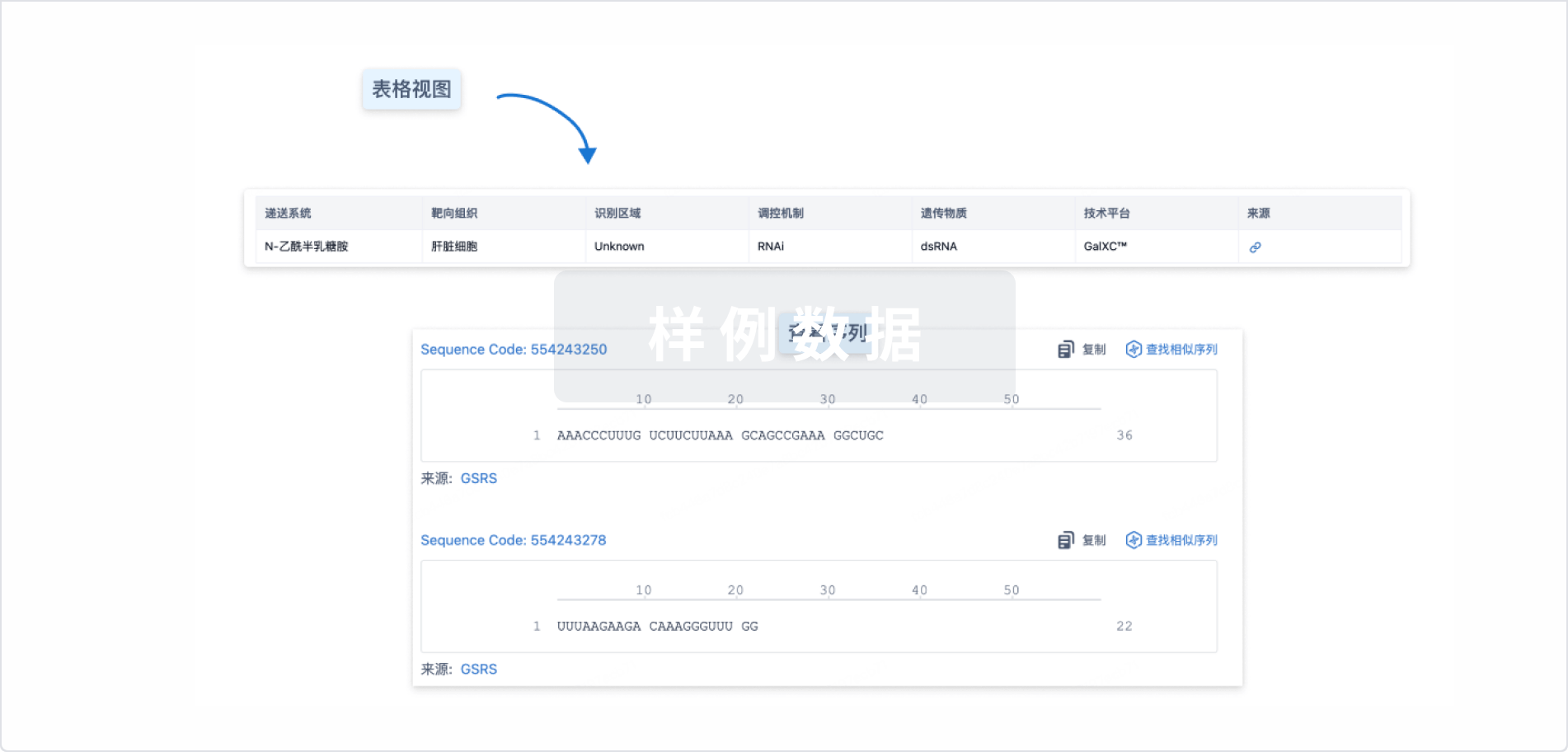
结构/序列
使用我们的RNA技术数据为新药研发加速。
登录
或
关联
100 项与 C1-INH(MiNA Therapeutics) 相关的临床结果
登录后查看更多信息
100 项与 C1-INH(MiNA Therapeutics) 相关的转化医学
登录后查看更多信息
100 项与 C1-INH(MiNA Therapeutics) 相关的专利(医药)
登录后查看更多信息
74
项与 C1-INH(MiNA Therapeutics) 相关的文献(医药)2023-10-15·International journal of cardiology
Mannose binding lectin-associated serine protease-1 is a novel contributor to myocardial ischemia/reperfusion injury.
Article
作者: Sang, Haiqiang ; Xu, Jing ; Sun, Jihong ; Guo, Shengcun ; Li, Yunpeng ; Hu, Fudong ; Yang, Linjie ; Cheng, Dong ; Zhang, Shengye
2023-07-01·Xenotransplantation
Antibody‐mediated rejection in xenotransplantation: Can it be prevented or reversed?
Review
作者: Ikechukwu, Ileka ; Pierson, Richard N. ; Hara, Hidetaka ; Zaletel, Tjasa ; Habibabady, Zahra ; Elias, Gabriela F. ; Cooper, David K. C. ; McGrath, Gannon ; Rosales, Ivy ; Maenaka, Akihiro ; Kinoshita, Kohei
2023-02-01·The American Journal of Emergency Medicine
Efficacy of human C1 esterase inhibitor concentrate for treatment of ACE-inhibitor induced angioedema
Article
作者: Trainotti, Susanne ; Volkenstein, Stefan ; Stelter, Klaus ; Hahn, Janina ; Bas, Murat ; Kojda, Georg ; Greve, Jens ; Hoffmann, Thomas K ; Gröger, Moritz ; Kehl, Victoria ; Wirth, Magdalena ; Wirth, Markus ; Strassen, Ulrich
1
项与 C1-INH(MiNA Therapeutics) 相关的新闻(医药)2021-07-01
Highlights the broader potential of Orchard’s ex vivo HSC gene therapy platform approach in new and larger indications
Reinforces Pharming’s commitment to the HAE community and utilizes its relevant clinical expertise and global commercialization infrastructure
Companies to host joint investor call at 8:00 a.m. EDT / 2:00 p.m. CEST
BOSTON, LONDON and LEIDEN, The Netherlands, July 01, 2021 (GLOBE NEWSWIRE) -- Orchard Therapeutics (Nasdaq: ORTX), a global gene therapy leader, and Pharming Group N.V. (Euronext Amsterdam: PHARM/Nasdaq: PHAR), a global, commercial stage biopharmaceutical company, today announced a strategic collaboration to research, develop, manufacture and commercialize OTL-105, a newly disclosed investigational ex vivo autologous hematopoietic stem cell (HSC) gene therapy for the treatment of hereditary angioedema (HAE), a life-threatening rare disorder that causes recurring swelling attacks in the face, throat, extremities and abdomen.
OTL-105 is an investigational HSC gene therapy designed to increase C1 esterase inhibitor (C1-INH) in HAE patient serum to prevent hereditary angioedema attacks. OTL-105 inserts one or more functional copies of the SERPING1 gene into patients own HSCs ex vivo which are then transplanted back into the patient for potential durable C1-INH production. In preclinical studies, to date, OTL-105 demonstrated high levels of SERPING1 gene expression via lentiviral-mediated transduction in multiple cell lines and primary human CD34+ HSCs. Furthermore, the program achieved production of functional C1-INH protein, as measured by a clinically validated assay.
Under the terms of the collaboration, Pharming has been granted worldwide rights to OTL-105 and will be responsible for clinical development, regulatory filings, and commercialization of the investigational gene therapy, including associated costs. Orchard will lead the completion of IND-enabling activities and oversee manufacturing of OTL-105 during pre-clinical and clinical development, which will be funded by Pharming. In addition, both companies will explore the application of non-toxic conditioning regimen for use with OTL-105 administration.
Orchard will receive an upfront payment of $17.5 million comprising $10 million in cash and a $7.5 million equity investment from Pharming at a premium to Orchard's recent share price. Orchard is also eligible to receive up to $189.5 million in development, regulatory and sales milestones as well as mid-single to low double-digit royalty payments on future worldwide sales.
“Given the combination of our expertise in HSC gene therapy with Pharming’s long-standing legacy and experience, we have the potential to reinvent the treatment paradigm for HAE by providing people living with this life-threatening disorder a sustained therapy with a single administration,” said Bobby Gaspar, M.D., Ph.D., chief executive officer of Orchard Therapeutics. “This collaboration demonstrates the promise of the HSC gene therapy platform and how it can be applied to new therapeutic areas with larger patient populations. We believe the HSC gene therapy pipeline we are building could continue to be a source of future partnerships in areas where the biology supports our approach.”
“Pharming has been committed to the HAE community for more than two decades,” said Sijmen de Vries M.D., MBA, chief executive officer of Pharming. “We have partnered with Orchard Therapeutics, a leader in the development of autologous HSC gene therapy, to develop a potentially curative treatment for HAE. Based on Pharming’s experience in HAE, we believe that HSC gene therapy has the potential for the highest probability of success. This confidence is based on the durability of effect and safety observed in approved treatments from Orchard’s HSC gene therapy portfolio and positive clinical data in several other programs. This a significant first step in developing a potentially transformative one-time treatment for HAE.”
“Great progress has been made in HAE treatment over the last 15 years. However, HAE remains a severe, debilitating disease with an ongoing burden of angioedema attacks or chronic medication use,” said Dr. Marc Riedl, professor of medicine and clinical director of the U.S. Hereditary Angioedema Association Center at the University of California, San Diego. “This promising work toward treatment with the potential for durable long-term clinical benefit is encouraging and signifies an ongoing commitment to the HAE community. I look forward to these efforts to identify and carefully advance a potential cure for HAE.”
The HAE market is expected to generate ~$2 billion in sales in 2021, currently growing at 8% per annum. This represents a significant commercial opportunity for Pharming Group and Orchard Therapeutics.
Webcast Link:
Participant Dial-in Details:
United Kingdom
0800 640 6441
United Kingdom (Local)
020 3936 2999
United States (Local)
1 646 664 1960
Netherlands
085 888 7233
All other locations
+44 20 3936 2999
Access code: 470719
About HAE
Hereditary angioedema (HAE) is a rare genetic disorder. The condition is caused by a deficiency of the C1 esterase inhibitor protein, which is normally present in blood and helps control inflammation (swelling) and parts of the immune system. Deficient C1 inhibitor does not adequately perform its regulatory function and, as a result, a biochemical imbalance can occur and produce unwanted peptides that induce the capillaries to release fluids into surrounding tissue, thereby causing swelling or edema.
HAE is characterized by spontaneous and recurrent episodes of swelling (edema attacks) of the skin in different parts of the body, as well as in the airways and internal organs. Edema of the skin usually affects the extremities, the face, and the genitals. Patients suffering from this kind of edema often withdraw from their social lives because of the disfiguration, discomfort and pain these symptoms may cause. Almost all HAE patients suffer from bouts of severe abdominal pain, nausea, vomiting and diarrhea caused by swelling of the intestinal wall.
Edema of the throat, nose or tongue is particularly dangerous and potentially life-threatening as it can lead to obstruction of the airway passages. Although there is currently no known cure for HAE, it is possible to treat the symptoms associated with angioedema attacks. HAE affects about 1 in 10,000 to 1 in 50,000 people worldwide. Experts believe a lot of patients are still seeking the right diagnosis: although HAE is (in principle) easy to diagnose, it is frequently identified very late or not discovered at all. The reason HAE is often misdiagnosed is because the symptoms are similar to those of many other common conditions such as allergies or appendicitis. By the time it is diagnosed correctly, the patient has often been through a long ordeal.
About Pharming Group N.V.
Pharming Group N.V. is a global, commercial stage biopharmaceutical company developing innovative protein replacement therapies and precision medicines for the treatment of rare diseases and unmet medical needs.
The flagship of our portfolio is our recombinant human C1 esterase inhibitor (rhC1INH) franchise. C1INH is a naturally occurring protein that down regulates the complement and contact cascades in order to control inflammation in affected tissues.
Our lead product, RUCONEST®, is the first and only plasma-free rhC1INH protein replacement therapy. It is approved for the treatment of acute hereditary angioedema (HAE) attacks. We are commercializing RUCONEST® in the United States, the European Union and the United Kingdom through our own sales and marketing organization, and the rest of the world through our distribution network.
In addition, we are investigating the clinical efficacy of rhC1INH in the treatment of further indications, including pre-eclampsia, acute kidney injury, and severe pneumonia as a result of COVID-19 infections.
Furthermore, we are leveraging our transgenic manufacturing technology to develop next-generation protein replacement therapies, most notably for Pompe disease, which is currently in preclinical development.
About Orchard Therapeutics
Orchard Therapeutics is a global gene therapy leader dedicated to transforming the lives of people affected by severe diseases through the development of innovative, potentially curative gene therapies. Our ex vivo autologous gene therapy approach harnesses the power of genetically modified blood stem cells and seeks to correct the underlying cause of disease in a single administration. In 2018, Orchard acquired GSK’s rare disease gene therapy portfolio, which originated from a pioneering collaboration between GSK and the San Raffaele Telethon Institute for Gene Therapy in Milan, Italy. Orchard now has one of the deepest and most advanced gene therapy product candidate pipelines in the industry spanning multiple therapeutic areas where the disease burden on children, families and caregivers is immense and current treatment options are limited or do not exist.
Orchard has its global headquarters in London and U.S. headquarters in Boston. For more information, please visit , and follow us on Twitter and LinkedIn.
Availability of Other Information About Orchard Therapeutics
Investors and others should note that Orchard communicates with its investors and the public using the company website ( ), the investor relations website (ir.orchard-tx.com), and on social media (Twitter and LinkedIn), including but not limited to investor presentations and investor fact sheets, U.S. Securities and Exchange Commission filings, press releases, public conference calls and webcasts. The information that Orchard posts on these channels and websites could be deemed to be material information. As a result, Orchard encourages investors, the media, and others interested in Orchard to review the information that is posted on these channels, including the investor relations website, on a regular basis. This list of channels may be updated from time to time on Orchard’s investor relations website and may include additional social media channels. The contents of Orchard’s website or these channels, or any other website that may be accessed from its website or these channels, shall not be deemed incorporated by reference in any filing under the Securities Act of 1933.
Orchard Therapeutics Forward-looking Statements
This press release contains certain forward-looking statements about Orchard’s strategy, future plans and prospects, which are made pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. Forward-looking statements include express or implied statements relating to, among other things, Orchard’s business strategy and goals, the therapeutic potential of Orchard’s product candidates, including the product candidate or candidates referred to in this release, and the possibility of future milestone or royalty payments. These statements are neither promises nor guarantees and are subject to a variety of risks and uncertainties, many of which are beyond Orchard’s control, which could cause actual results to differ materially from those contemplated in these forward-looking statements. In particular, these risks and uncertainties include, without limitation: the risk that prior results, such as signals of safety, activity or durability of effect, observed from preclinical studies or clinical trials will not be replicated or will not continue in ongoing or future studies or trials involving Orchard’s product candidates, will be insufficient to support regulatory submissions or marketing approval in the US or EU, as applicable, or that long-term adverse safety findings may be discovered; the risk that any one or more of Orchard’s product candidates, including the product candidates referred to in this release, will not be approved, successfully developed or commercialized; the risk of cessation or delay of any of Orchard’s ongoing or planned clinical trials; the risk that Orchard may not successfully recruit or enroll a sufficient number of patients for its clinical trials; the delay of any of Orchard’s regulatory submissions; the failure to obtain marketing approval from the applicable regulatory authorities for any of Orchard’s product candidates or the receipt of restricted marketing approvals; the inability or risk of delays in Orchard’s ability to commercialize its product candidates, if approved, or Libmeldy in the EU; the risk that the market opportunity for Libmeldy, or any of Orchard’s product candidates, may be lower than estimated; the risk that certain milestones may never be achieved or royalty payments may never be earned and paid; and the severity of the impact of the COVID-19 pandemic on Orchard’s business, including on clinical development, its supply chain and commercial programs. Given these uncertainties, the reader is advised not to place any undue reliance on such forward-looking statements.
Other risks and uncertainties faced by Orchard include those identified under the heading "Risk Factors" in Orchard’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2021, as filed with the U.S. Securities and Exchange Commission (SEC), as well as subsequent filings and reports filed with the SEC. The forward-looking statements contained in this press release reflect Orchard’s views as of the date hereof, and Orchard does not assume and specifically disclaims any obligation to publicly update or revise any forward-looking statements, whether as a result of new information, future events or otherwise, except as may be required by law.
Pharming Group N.V. Forward-looking Statements
This press release contains forward-looking statements, including with respect to timing and progress of Pharming’s preclinical studies and clinical trials of its product candidates, Pharming’s clinical and commercial prospects, Pharming’s ability to overcome the challenges posed by the COVID-19 pandemic to the conduct of its business, and Pharming’s expectations regarding its projected working capital requirements and cash resources, which statements are subject to a number of risks, uncertainties and assumptions, including, but not limited to the scope, progress and expansion of Pharming’s clinical trials and ramifications for the cost thereof; and clinical, scientific, regulatory and technical developments. In light of these risks and uncertainties, and other risks and uncertainties that are described in Pharming’s 2020 Annual Report and the Annual Report on Form 20-F for the year ended December 31, 2020 filed with the U.S. Securities and Exchange Commission, the events and circumstances discussed in such forward-looking statements may not occur, and Pharming’s actual results could differ materially and adversely from those anticipated or implied thereby. Any forward-looking statements speak only as of the date of this press release and are based on information available to Pharming as of the date of this release.
Inside Information
This press release relates to the disclosure of information that qualifies, or may have qualified, as inside information within the meaning of Article 7(1) of the EU Market Abuse Regulation.
Orchard Therapeutics Contacts
Investors
Renee Leck
Director, Investor Relations
+1 862-242-0764
Renee.Leck@orchard-tx.com
Media
Benjamin Navon
Director, Corporate Communications
+1 857-248-9454
Benjamin.Navon@orchard-tx.com
Pharming Group N.V. Contacts
Company
Pharming Group, Leiden, The Netherlands
Sijmen de Vries,
CEO
+31 71 524 7400
Investors
Susanne Embleton
Investor Relations Manager
+31 71 524 7400
investor@pharming.com
Media
FTI Consulting, London, UK
Victoria Foster Mitchell/Alex Shaw
+44 203 727 1000
LifeSpring Life Sciences Communication, Amsterdam, The Netherlands
Leon Melens
+31 6 53 81 64 27
pharming@lifespring.nl
合作基因疗法
100 项与 C1-INH(MiNA Therapeutics) 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 自身免疫性疾病 | 临床前 | 英国 | 2024-06-27 | |
| 遗传性血管性水肿 | 临床前 | 英国 | 2024-06-27 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
| 研究 | 分期 | 人群特征 | 评价人数 | 分组 | 结果 | 评价 | 发布日期 |
|---|
No Data | |||||||
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

芽仔
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用