预约演示
更新于:2026-05-30
Semaglutide (China Resources Double-Crane)
司美格鲁肽(华润双鹤)
更新于:2026-05-30
概要
基本信息
原研机构 |
非在研机构- |
权益机构- |
最高研发阶段申请上市 |
首次获批日期- |
最高研发阶段(中国)申请上市 |
特殊审评- |
登录后查看时间轴
结构/序列
Sequence Code 50953
当前序列信息引自: *****
关联
2
项与 司美格鲁肽(华润双鹤) 相关的临床试验CTR20242569
司美格鲁肽注射液在中国2型糖尿病患者中的有效性和安全性Ⅲ期临床试验
CTR20241524
司美格鲁肽注射液人体药代动力学比对研究
100 项与 司美格鲁肽(华润双鹤) 相关的临床结果
登录后查看更多信息
100 项与 司美格鲁肽(华润双鹤) 相关的转化医学
登录后查看更多信息
100 项与 司美格鲁肽(华润双鹤) 相关的专利(医药)
登录后查看更多信息
617
项与 司美格鲁肽(华润双鹤) 相关的文献(医药)2026-12-01MOLECULAR BIOLOGY REPORTS
Targeting UBE2B-mediated U2AF1 degradation to alleviate endothelial dysfunction in renal ischemia-reperfusion injury: therapeutic potential of semaglutide
Article
作者: Wang, Qian ; Zhang, Lihui ; Wang, Jing ; Ren, Suxia ; Wang, Ting ; Zhu, Qiuxiao ; Jiao, Lijing
BACKGROUND:
Renal ischemia-reperfusion injury (RIRI) is a major cause of acute kidney injury, with endothelial dysfunction playing a central role in its pathophysiology. However, the molecular mechanisms underlying endothelial damage during RIRI remain incompletely understood.
METHODS AND RESULTS:
We investigated the role of ubiquitin-conjugating enzyme E2 B (UBE2B) in endothelial cell regulation during RIRI. Our data indicate that upregulation of UBE2B promotes endothelial apoptosis and inhibits proliferation by targeting U2 small nuclear RNA auxiliary factor 1 (U2AF1) for ubiquitination and degradation, thereby modulating the p53/p21 signaling pathway. Furthermore, treatment with semaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist, alleviated endothelial injury in our models, which was associated with reduced UBE2B expression, oxidative stress, and apoptosis.
CONCLUSIONS:
These findings suggest a previously unrecognized role of UBE2B in mediating endothelial dysfunction during RIRI and indicate that targeting this pathway may hold therapeutic potential. Moreover, semaglutide showed protective effects against endothelial damage under our experimental conditions, pointing to a possible strategy for RIRI management that warrants further validation in long-term and clinical studies.
2026-07-01SURVEY OF OPHTHALMOLOGY
Too much of a good thing
Article
作者: Abdelsalam, Dina ; Bhatti, M Tariq ; Varghese, Danny ; Lee, Andrew G ; Ibrahim, Safa
A 38-year-old man with poorly controlled type 2 diabetes mellitus and arterial hypertension on semaglutide presented with acute, painless, vision loss in the left eye. Ophthalmic examination revealed optic disc edema (ODE) in the left eye and optic disc pallor (ODP) in the right eye, accompanied by severe nonproliferative diabetic retinopathy and cystoid macular edema in both eyes. The combination of ODE in one eye and ODP in the fellow eye raised concern for the Foster Kennedy syndrome secondary to an intracranial mass; however, neuroimaging and systemic evaluation were unremarkable. Ultimately, it was decided the ODP was due to a prior unrecognized non-arteritic anterior ischemic optic neuropathy (NAION) event, and the ODE was the result of an acute NAION in the symptomatic fellow eye (i.e. pseudo-Foster Kennedy syndrome).
2026-07-01ANALYTICAL BIOCHEMISTRY
Development of an electrochemiluminescence immunoassay for quantitative determination of semaglutide in human serum
Article
作者: Zou, Linglong ; Zhang, Junyan ; Zhang, Hefeng ; Luo, Yifan ; Chen, Wenlong
Semaglutide, a long-acting glucagon-like peptide-1 receptor agonist (GLP-1RA), is widely used in the treatment of patients with type 2 diabetes mellitus and obesity. A sensitive and reliable quantification method is essential for bioanalysis of semaglutide in clinical studies. To develop a sensitive and specific immunoassay, we have prepared a pair of highly specific anti-semaglutide monoclonal antibodies and subsequently employed them as critical reagents in the development of an electrochemiluminescence immunoassay (ECLIA) for the quantification of semaglutide levels in human serum. The assay validation data presented here demonstrate that the performance of the ECLIA method meets prespecified criteria for all validation parameters within the quantitative range of 0.5 ng/mL to 200.0 ng/mL. The intra- and inter-assay precision (%CV) are both ≤14.4%, and accuracy (%RE) ranges from -12.5% to 15.3%. No interference is found with recombinant human GLP-1 as the endogenous counterpart, confirming the assay specificity. Additional assay performance parameters, including selectivity, dilutional linearity, hook effect, and sample stability, all meet the acceptance criteria preset in accordance with international guidelines for bioanalytical method validation. The method is suitable for bioanalysis of semaglutide in human serum.
100 项与 司美格鲁肽(华润双鹤) 相关的药物交易
登录后查看更多信息
外链
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| - | - | - |
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 2型糖尿病 | 临床3期 | 中国 | 2024-08-02 | |
| 肥胖 | 临床申请批准 | 中国 | 2024-11-20 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
登录后查看更多信息
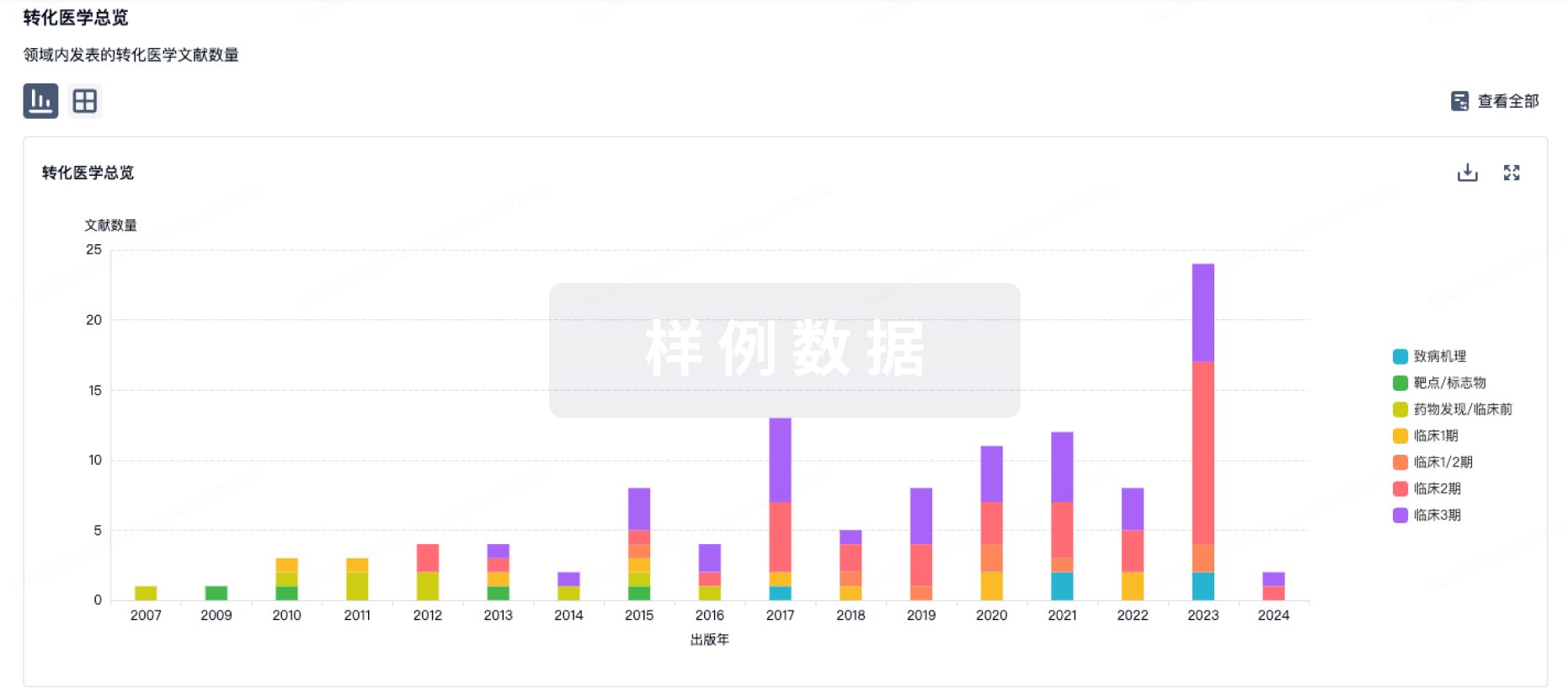
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
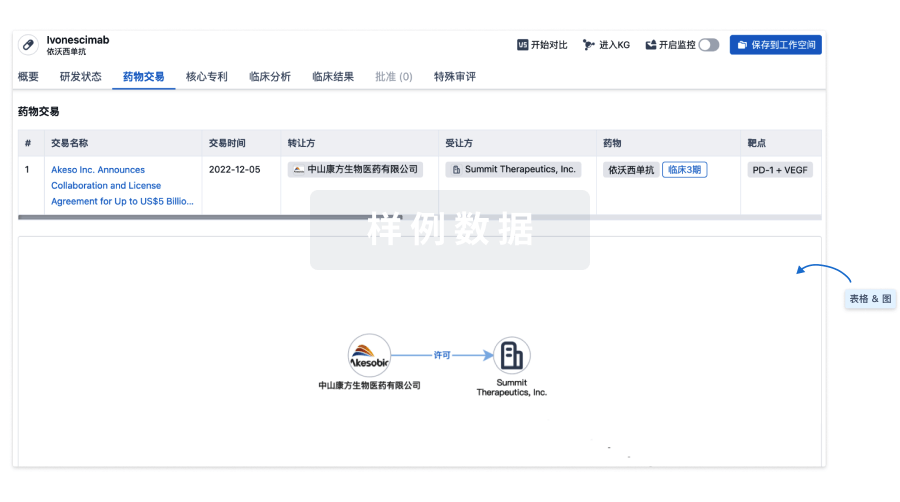
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
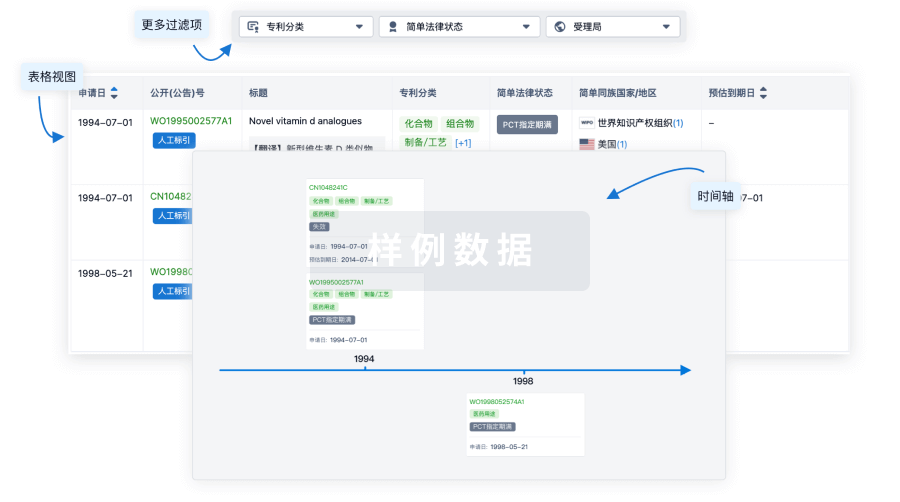
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

生物类似药
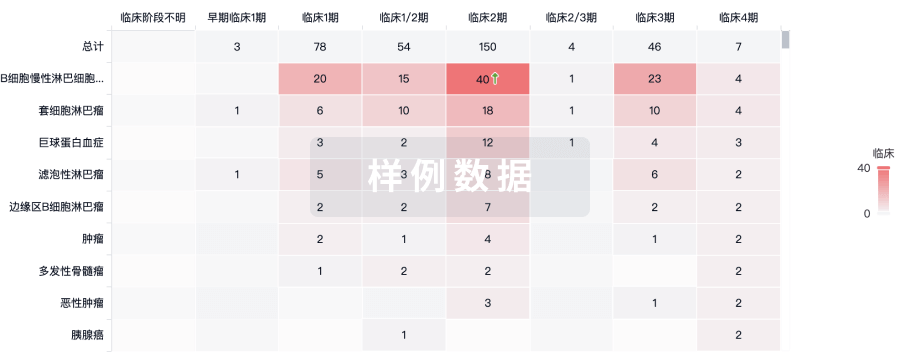
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用