预约演示
更新于:2025-05-07
ImClone Systems Corp.
注销
| 私营公司|New Jersey, United States注销
| 私营公司|New Jersey, United States更新于:2025-05-07
概览
关联
100 项与 ImClone Systems Corp. 相关的临床结果
登录后查看更多信息
0 项与 ImClone Systems Corp. 相关的专利(医药)
登录后查看更多信息
3
项与 ImClone Systems Corp. 相关的文献(医药)2014-05-20·Journal of Clinical Oncology
Final results of a phase 2 study of ramucirumab (RAM) plus eribulin (E) versus E in advanced metastatic breast cancer (MBC).
作者: Bromund, Jane L. ; Osborne, Cynthia R. C. ; Paul, Devchand ; Yardley, Denise A. ; Ibrahim, Ayman B. ; Soliman, Hatem Hussein ; Xu, Yihuan ; Richards, Paul D. ; Ademuyiwa, Foluso Olabisi ; Reeves, James Andrew ; Dees, Elizabeth Claire ; Guthrie, Troy H.
2013-01-01·mAbs2区 · 医学
Conformational characterization of the charge variants of a human IgG1 monoclonal antibody using H/D exchange mass spectrometry
2区 · 医学
Article
作者: Carlson, Ping ; Zhou, Qinwei ; Parekh, Babita ; Hsieh, Ming-Ching ; Matathia, Alice ; Tang, Liangjie ; Sundaram, Shanmuuga ; Zhang, Jingming
2012-09-20·Journal of Clinical Oncology
Interim safety results of eribulin (E) combined with ramucirumab (RAM) in patients (pts) with advanced metastatic breast cancer (MBC).
作者: Favret, Anne ; Daniel, Brooke R. ; Hsu, Yanzhi ; Bromund, Jane ; Richards, Paul D. ; Danso, Michael A. ; Ibrahim, Ayman B. ; Osborne, Cynthia R. C. ; Yardley, Denise Aysel
4
项与 ImClone Systems Corp. 相关的新闻(医药)2014-09-25
September 25, 2014
By
Jessica Wilson
, BioSpace.com Breaking News Staff
Kadmon Corporation, LLC, the New York, NY-based biopharmaceutical company, announced yesterday that Samuel Waksal has stepped down as Chief Executive Officer and will be replaced by Harlan Waksal, his brother, who has served on the board since April 2014. Samuel Waksal will remain with Kadmon as Chief of Innovation, Science and Strategy.
The Waksal brothers have had a long career in the biotech space, which included founding ImClone Systems Incorporated, now a wholly-owned subsidiary of Eli Lilly and Company. The career has been marked with scandal, however, for Samuel Waksal, who was convicted on charges of insider trading, and served a five-year sentence. (To put this in context, he was involved in the same scandal that put Martha Stewart in federal prison.) As part of his 2003 settlement with the U.S. Securities Exchange Commission, Samuel Waksal agreed to a lifetime ban on helming a publicly traded company.
The change in leadership at Kadmon Corporation could be a step to prepare the company for an IPO, which could not take place with Samuel Waksal as CEO. In the press release announcing the leadership change, Kadmon stated, “While the company is continuing to explore its strategic and financial opportunities, including an initial public offering, no specific timelines have been set.”
Despite the coy statement, Samuel Waksal has not been shy about stating his determination for a Kadmon IPO. In fact, yesterday, he said in an interview with CNBC that the company plans to form S-1 with the SEC by the end of 2014, which is a preparatory step in an IPO.
In addition, as early as September 2013, he told Bloomberg, “We haven’t seen a biotech market like this since 2000. You get these windows, you get companies funded, you get shareholders that are interested in an approach, a strategy, a technology, a management team, and often, you really get big winners.”
In the press release, Harlan Waksal expressed his enthusiasm for, “building on the foundation of forward-thinking science, clinical research, and product pipeline, including our current clinical candidates, envisioned and put together by Sam and our management team.”
Kadmon currently offers treatments for liver diseases, with a pipeline that includes novel medicines in the areas of oncology, immunology and infectious, neurodegenerative and ophthalmic diseases. The company’s research targets the metabolomics and signaling pathways associated with disease.
var switchTo5x=true;
stLight.options({publisher: "0341611e-38a4-415d-9e18-75e093ff27e0", doNotHash: false, doNotCopy: false, hashAddressBar: false});
高管变更
2008-06-02
CHICAGO — Two biotechnology giants did battle here at the nation’s largest cancer conference over the weekend. And both remained standing.
2005-05-16
ORLANDO, Fla., May 16 /PRNewswire-FirstCall/ -- ImClone Systems Incorporated and Bristol-Myers Squibb Company today announced the results of several clinical studies of ERBITUX(R) (Cetuximab), an IgG1 monoclonal antibody, presented at the American Society of Clinical Oncology (ASCO) 41st Annual Meeting.
Data were presented from clinical studies exploring treatment of various stages of colorectal, head and neck, and ovarian cancers using ERBITUX either as a single agent or in combination with cytotoxic agents, including chemotherapy and radiation therapy. The studies included:
* Abstract 3508: Findings were presented of a randomized Phase II trial
conducted by the National Cancer Institute to evaluate the efficacy and
safety of the use of ERBITUX and AVASTIN(TM) (bevacizumab) with or
without irinotecan in 81 patients with irinotecan-refractory metastatic
colorectal cancer. Of 41 patients who received
ERBITUX/bevacizumab/irinotecan, 37 percent had a partial response (95%
CI: 22-53), and the median time to progression was 7.9 months. Of 40
patients who received ERBITUX/bevacizumab alone, 20 percent of patients
had a partial response (95% CI: 9-36), and the median time to
progression was 5.6 months. The most commonly reported adverse events
in the ERBITUX/bevacizumab/irinotecan arm were skin rash (grade 2, 60%;
grade 3, 17%), diarrhea (grade 2, 29%; grade 3/4, 24%), fatigue (grade
2, 32%; grade 3, 10%) and neutropenia (grade 3/4, 22%). The most
commonly reported adverse event in the ERBITUX/bevacizumab arm was skin
rash (grade 2, 65%; grade 3, 20%).
* Abstract 3535: An international Phase II study (EMR-018) evaluated the
safety and efficacy of ERBITUX in combination with FOLFOX-4
(oxaliplatin/5-fluorouracil/folinic acid) as first-line treatment in
patients with non-resectable, EGFR-expressing metastatic colorectal
cancer. In a preliminary efficacy analysis of 42 patients, 10 percent
had a complete response (95% CI: 3-23), 71 percent had a partial
response (95% CI: 55-84), and 17 percent had stable disease (95% CI:
7-31). Median progression-free survival was 12.3 months. Nine
patients subsequently underwent surgery of their metastases. The major
grade 3/4 toxicities in 43 patients evaluable for safety were acne-like
rash (30%), neurotoxicity (30%), diarrhea (26%), neutropenia (21%) and
stomatitis/mucositis (16%).
* Abstract 5533: A retrospective subgroup analysis evaluated 171 patients
with hypopharyngeal and laryngeal carcinoma who were enrolled in an
international Phase III randomized trial (IMC-9815) of 424 patients
with locoregionally advanced squamous-cell carcinoma of the head and
neck. The randomized study evaluated the addition of ERBITUX to high-
dose radiation versus radiation alone, to evaluate the primary endpoint
of locoregional control and secondary endpoint of overall survival. The
subgroup analysis was undertaken to assess the rates of organ
preservation in patients who had hypopharyngeal and laryngeal
carcinoma. Of the 93 patients receiving ERBITUX plus radiation, larynx
preservation rates were 90 percent at two years and 87 percent at three
years. Of the 78 patients receiving radiation therapy alone, larynx
preservation rates were 80 percent at two years and 77 percent at three
years (hazard ratio 0.51; 95% CI: 0.21-1.24). Because the study was
not powered to assess organ preservation, these results were not
statistically significant.
* Abstract 5047: A Phase II study (CA225009) examining the addition of
ERBITUX to standard chemotherapy with paclitaxel and carboplatin as
first-line treatment of EGFR-expressing advanced ovarian, primary
peritoneal and fallopian tube cancer. The primary endpoint is
progression-free survival. Preliminary data were reported for the
first 27 patients to complete six cycles of initial treatment. Of the
12 patients with stage III cancer whose tumor was completely removed by
surgery, 91.7 percent (95% CI: 61.52-99.79) achieved a clinical
complete response. Of the nine patients with stage III disease whose
tumors could not be completely removed, 44.4 percent (95% CI: 13.70-
78.80) achieved a clinical complete response. Of the six patients with
stage IV disease, four were evaluable for efficacy. Of these four,
50.0 percent (95% CI: 6.76-93.24) achieved a clinical complete
response. Commonly occurring grade 3 adverse events in all 27 patients
receiving initial therapy were febrile neutropenia (18.5%),
hypokalaemia (14.8%) and dyspnea (11.1%). Three hypersensitivity
reactions were reported (grade 3, 7.4%; grade 4, 3.7%). Eighteen
patients experienced a rash (grade 1, 48.1%; grade 2, 18.5%).
"Clinical trial results observed in combinations of ERBITUX with widely used cancer treatments improve our understanding of where to focus our future study of this antibody," said Eric Rowinsky, M.D., Chief Medical Officer of ImClone Systems. "Our long-term commitment to developing ERBITUX in multiple indications will include pivotal or exploratory studies of ERBITUX with other targeted therapies in colorectal, lung, pancreatic and ovarian cancers in addition to our ongoing Phase III studies with chemotherapy."
"Bristol-Myers Squibb and ImClone Systems are dedicated to the ongoing investigation of ERBITUX and to providing more treatment options for cancer patients in the future," said Martin Birkhofer, M.D., Vice President, Oncology Global Medical Affairs, Bristol-Myers Squibb.
About ERBITUX(R) (Cetuximab)
On February 12, 2004, the FDA approved ERBITUX for use in the United States in combination with irinotecan in the treatment of patients with EGFR- expressing, metastatic colorectal cancer who are refractory to irinotecan- based chemotherapy and for use as a single agent in the treatment of patients with EGFR-expressing, metastatic colorectal cancer who are intolerant to irinotecan-based chemotherapy. The effectiveness of ERBITUX is based on objective response rates. Currently, no data are available that demonstrate an improvement in disease-related symptoms or increased survival with ERBITUX.
Important Safety Information
Severe infusion reactions, rarely fatal and characterized by rapid onset of airway obstruction (bronchospasm, stridor, hoarseness), urticaria, and hypotension, have occurred in approximately 3% (20/774) of patients with the administration of ERBITUX. Most reactions (90%) are associated with the first infusion of ERBITUX despite the use of prophylactic antihistamines. Caution must be exercised with every ERBITUX infusion as there were patients who experienced their first severe infusion reaction during later infusions. Severe infusion reactions require immediate and permanent discontinuation of ERBITUX therapy.
Severe cases of interstitial lung disease (ILD), which was fatal in one case, occurred in less than 0.5% of 774 patients receiving ERBITUX.
Dermatologic toxicities, including acneform rash (11% of 774 patients, grade 3/4), skin drying and fissuring, inflammatory or infectious sequelae (e.g. blepharitis, cheilitis, cellulitis, cyst) and paronychial inflammation (0.4% of 774 patients, grade 3) were reported. Sun exposure may exacerbate any skin reactions.
Hypomagnesemia has been reported with ERBITUX when administered as a single agent and in combination with multiple different chemotherapeutic regimens. The incidence of hypomagnesemia (both overall and severe [NCI CTC grades 3 & 4]) is increased in patients receiving chemotherapy and ERBITUX as compared to those receiving chemotherapy alone based on controlled clinical trials. Patients receiving ERBITUX therapy should be monitored for hypomagnesemia. Magnesium repletion may be necessary based on clinical judgment.
Other serious adverse events associated with ERBITUX in clinical trials (n=774) were fever (5%), sepsis (3%), kidney failure (2%), pulmonary embolus (1%), dehydration (5% in patients receiving ERBITUX plus irinotecan, 2% receiving ERBITUX as a single agent) and diarrhea (6% in patients receiving ERBITUX plus irinotecan, 0.2% with ERBITUX as a single agent).
Additional common adverse events seen in patients receiving ERBITUX plus irinotecan (n=354) or ERBITUX as a single agent (n=420) were acneform rash (88%/90%), asthenia/malaise (73%/48%), diarrhea (72%/25%), nausea (55%/29%), abdominal pain (45%/26%), vomiting (41%/25%), fever (34%/27%), constipation (30%/26%) and headache (14%/26%).
Full prescribing information, including boxed WARNING regarding infusion reactions is available upon request or by visiting .
About ImClone Systems
ImClone Systems Incorporated is committed to advancing oncology care by developing and commercializing a portfolio of targeted biologic treatments designed to address the medical needs of patients with a variety of cancers. The Company's research and development programs include growth factor blockers and angiogenesis inhibitors. ImClone Systems' strategy is to become a fully integrated biopharmaceutical company, taking its development programs from the research stage to the market. ImClone Systems' headquarters and research operations are located in New York City, with additional administration and manufacturing facilities in Branchburg, New Jersey.
Certain matters discussed in this news release may constitute forward- looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 and the Federal securities laws. Although the company believes that the expectations reflected in such forward-looking statements are based upon reasonable assumptions it can give no assurance that its expectations will be achieved. Forward-looking information is subject to certain risks, trends and uncertainties that could cause actual results to differ materially from those projected. Many of these factors are beyond the company's ability to control or predict. Important factors that may cause actual results to differ materially and could impact the company and the statements contained in this news release can be found in the company's filings with the Securities and Exchange Commission including quarterly reports on Form 10-Q, current reports on Form 8-K and annual reports on Form 10-K. For forward-looking statements in this news release, the company claims the protection of the safe harbor for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995. The company assumes no obligation to update or supplement any forward-looking statements whether as a result of new information, future events or otherwise.
About Bristol-Myers Squibb
Bristol-Myers Squibb is a global pharmaceutical and related health care products company whose mission is to extend and enhance human life.
This press release contains "forward-looking statements" as that term is defined in the Private Securities Litigation Reform Act of 1995 regarding product development. Such forward-looking statements are based on current expectations and involve inherent risks and uncertainties, including factors that could delay, divert or change any of them, and could cause actual outcomes and results to differ materially from current expectations. No forward-looking statement can be guaranteed. Forward-looking statements in this press release should be evaluated together with the many uncertainties that affect Bristol-Myers Squibb's business, particularly those identified in the cautionary factors discussion in Bristol-Myers Squibb's Annual Report on Form 10-K for the year ended December 31, 2004 and in our Quarterly Reports on Form 10-Q. Bristol-Myers Squibb undertakes no obligation to publicly update any forward-looking statement, whether as a result of new information, future events or otherwise.
ERBITUX is a registered trademark of ImClone Systems Incorporated.
AVASTIN is a trademark of Genentech, Inc.
Media and Investor Contacts:
Andrea Rabney Kathy Baum
Corporate Communications Business and R&D Communications
ImClone Systems Incorporated Bristol-Myers Squibb
Tel: (646) 638-5058 Tel: (609) 252-4227
Andrea.Rabney@imclone.com Cell: (609) 575-0017
or or
David Pitts John Elicker
Corporate Communications Investor Relations
ImClone Systems Incorporated Bristol-Myers Squibb
Tel: (646) 638-5058 Tel: (212) 546-3775
David.Pitts@imclone.com
or
Stefania Bethlen
Corporate Communications/IR
ImClone Systems Incorporated
Tel: (646) 638-5058
Stefania.Bethlen@imclone.com
Bristol-Myers Squibb; ImClone Systems Incorporated
CONTACT: Corporate Communications: Andrea Rabney,Andrea.Rabney@imclone.com, David Pitts, David.Pitts@imclone.com, +1-646-638-5058, Corporate Communications/IR: Stefania Bethlen, +1-646-638-5058,Stefania.Bethlen@imclone.com, all of ImClone Systems Incorporated; Kathy Baum,+1-609-252-4227, +1-609-575-0017 (cell), John Elicker, Investor Relations,+1-212-546-3775, all of Bristol-Myers Squibb
Web site:
抗体放射疗法ASCO会议
100 项与 ImClone Systems Corp. 相关的药物交易
登录后查看更多信息
100 项与 ImClone Systems Corp. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年07月02日管线快照
无数据报导
登录后保持更新
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
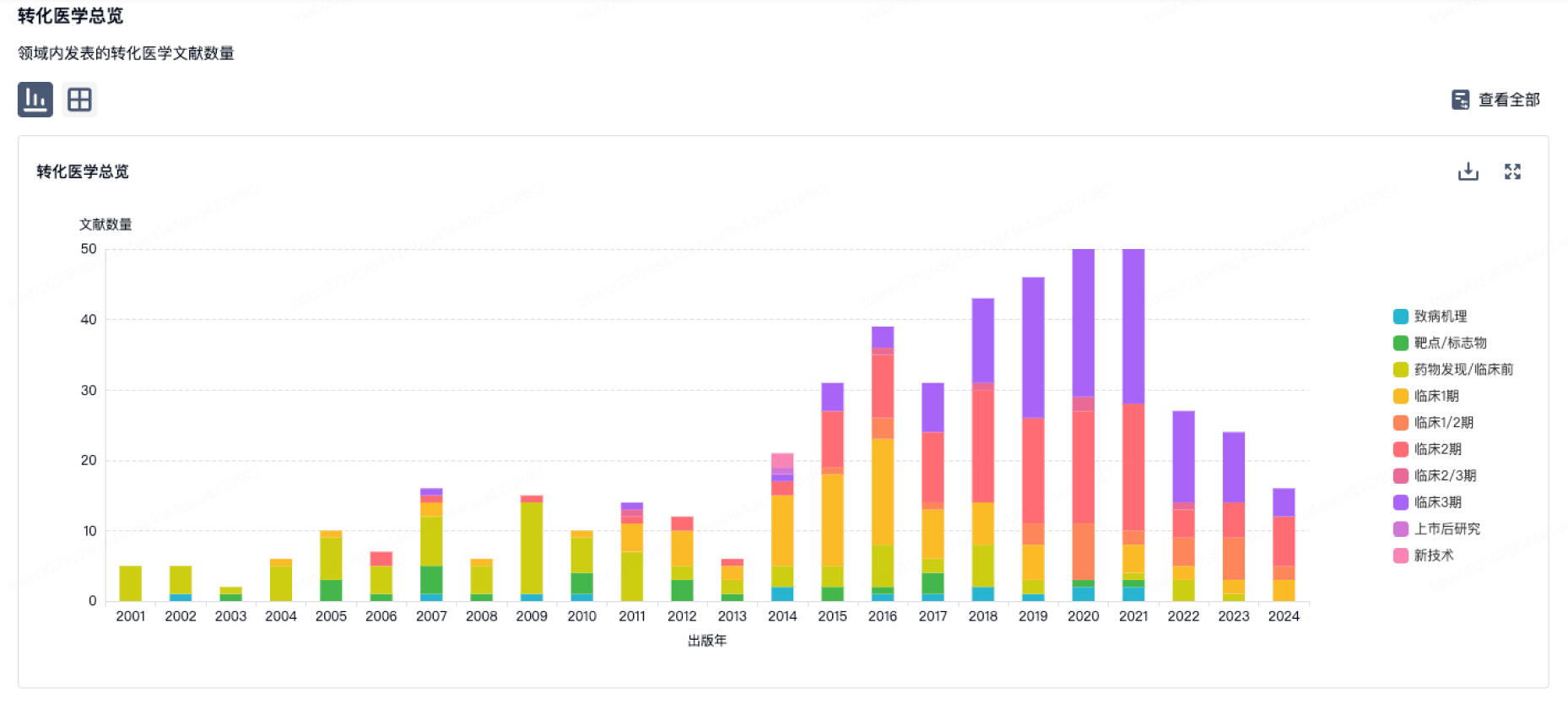
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
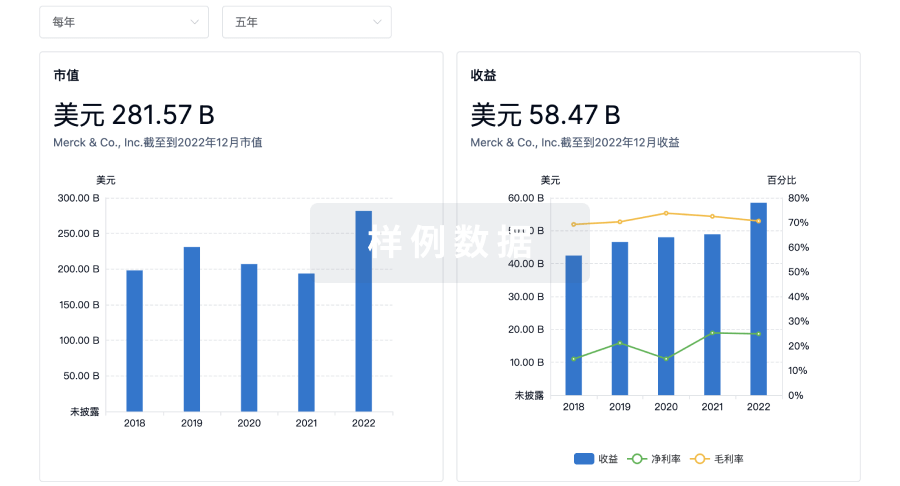
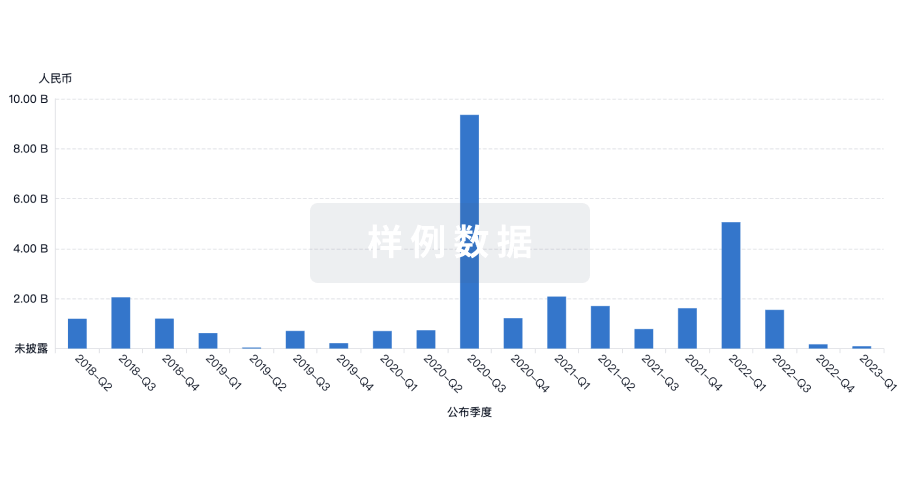
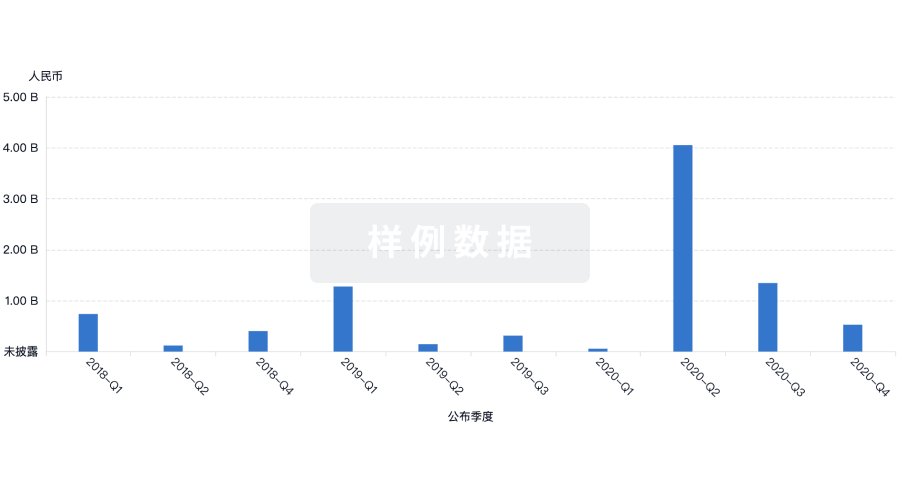
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用