预约演示
更新于:2026-05-19
Genetron Health (Beijing) Co., Ltd.
更新于:2026-05-19
概览
关联
NCT05023746
Clinical Evaluation of Genetron Lung Cancer Panel in Non-small Cell Lung Cancer Patients
100 项与 北京泛生子基因科技有限公司 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-06-01Translational Cancer Research
Development and clinical applications of liquid biopsy assays in cancer screening
Review
作者: Song, Lele ; Han, Ying ; Gong, Yuan ; Zhang, Peiying
Liquid biopsy has become a research focus and a hotspot of product development in cancer screening. With the rapid development of molecular biology technology, many new markers have been identified and developed in cancer screening tests in recent years. This article reviews the development of novel liquid biopsy-based markers in cancer screening, including methylation, hydroxymethylation, mutation, copy number variation, and microRNA (miRNA), with specific focuses on clinical trials and studies from approved cancer screening assays or tests under development in China. Studies on screening of lung cancer, hepatocellular carcinoma (HCC), colorectal cancer, gastric cancer, esophageal cancer, and multiple cancers (pan-cancer screening) are reviewed and summarized. Liquid biopsy techniques detecting novel markers show great potential in the early screening of cancers, but still face challenges in sensitivity, specificity, productization, standardization, and cost-effectiveness. The emerging pan-cancer screening represents a direction of high-throughput and multiple cancer simultaneous screening, while it still needs optimization in detection performance and organ-specific recognition. Multi-omics integration analysis, artificial intelligence (AI)-assisted diagnosis, and large-scale prospective clinical studies will become important development steps in this field. Through a systematic review of the relevant literature, this paper describes in detail the development of new liquid biopsy technology, new progress in the field of cancer early screening, clinical application status, and future research direction. The review provides some useful insights into the future selection of early screening technology, the formulation of clinical research or trial protocols, and the balance between performance and cost.
2023-01-01Clinical lung cancer
A Novel PRKAR1A::MET Fusion Dramatic Response to Crizotinib in a Patient with Unresectable Lung Cancer
作者: Zhang, Yanxiang ; Yang, Yang ; Zhao, Dandan ; Ma, Tonghui ; Li, Xiaoli
This report demonstrated a significant clin. benefit from first-line treatment of crizotinib in a patient with unresectable lung cancer with novel PRKAR1A::MET gene fusion.After disease progress resulted from discontinued therapy, the patient still achieved clin. benefit from second-line monotherapy of crizotinib.This finding provided insight to perform the clin. trials to assess the efficacy and rationale of first-line or second line treatment to patients with unresectable lung cancer carrying MET fusion.
2022-01-17Briefings in bioinformatics
Calling small variants using universality with Bayes-factor-adjusted odds ratios
Article
作者: Wang, Sizhen ; Zhao, Xiaofei ; Hu, Allison C ; Wang, Xiaoyue
Abstract:
The application of next-generation sequencing in research and particularly in clinical routine requires highly accurate variant calling. Here we describe UVC, a method for calling small variants of germline or somatic origin. By unifying opposite assumptions with sublation, we discovered the following two empirical laws to improve variant calling: allele fraction at high sequencing depth is inversely proportional to the cubic root of variant-calling error rate, and odds ratios adjusted with Bayes factors can model various sequencing biases. UVC outperformed other variant callers on the GIAB germline truth sets, 192 scenarios of in silico mixtures simulating 192 combinations of tumor/normal sequencing depths and tumor/normal purities, the GIAB somatic truth sets derived from physical mixture, and the SEQC2 somatic reference sets derived from the breast-cancer cell-line HCC1395. UVC achieved 100% concordance with the manual review conducted by multiple independent researchers on a Qiagen 71-gene-panel dataset derived from 16 patients with colon adenoma. UVC outperformed other unique molecular identifier (UMI)-aware variant callers on the datasets used for publishing these variant callers. Performance was measured with sensitivity-specificity trade off for called variants. The improved variant calls generated by UVC from previously published UMI-based sequencing data provided additional insight about DNA damage repair. UVC is open-sourced under the BSD 3-Clause license at https://github.com/genetronhealth/uvc and quay.io/genetronhealth/gcc-6-3-0-uvc-0-6-0-441a694
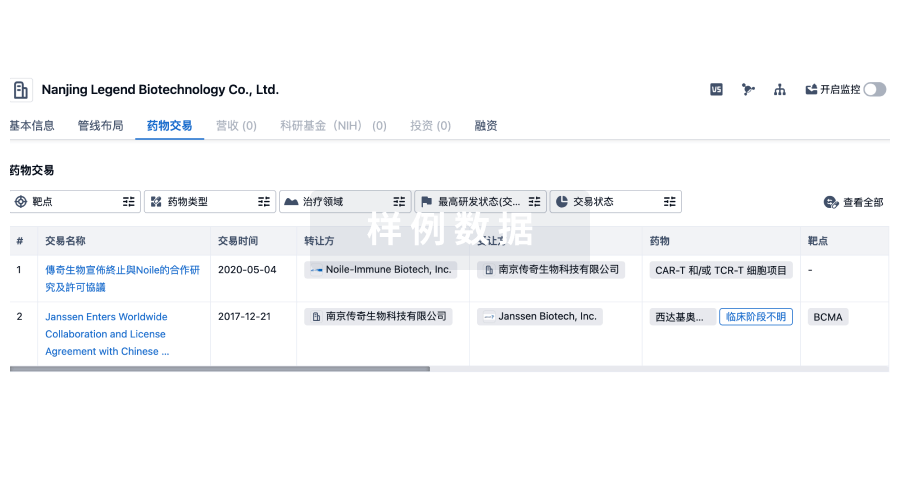
100 项与 北京泛生子基因科技有限公司 相关的药物交易
登录后查看更多信息
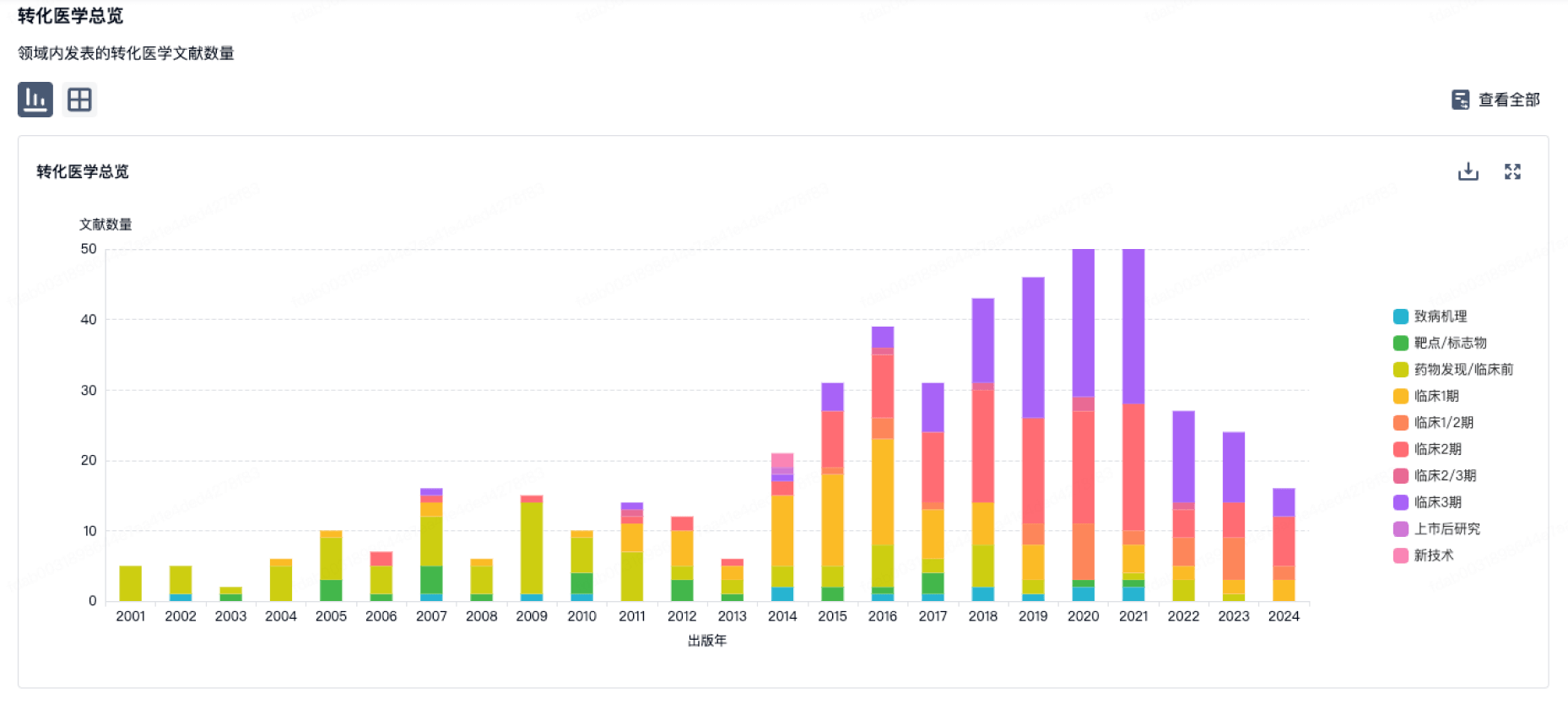
100 项与 北京泛生子基因科技有限公司 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月01日管线快照
无数据报导
登录后保持更新
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
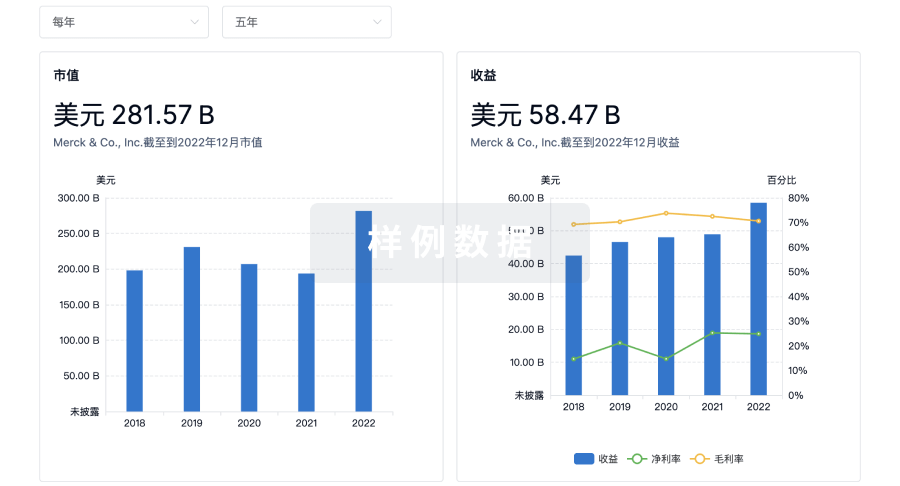
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用