预约演示
更新于:2025-12-05

Pritzker School of Medicine
更新于:2025-12-05
概览
关联
100 项与 Pritzker School of Medicine 相关的临床结果
登录后查看更多信息
0 项与 Pritzker School of Medicine 相关的专利(医药)
登录后查看更多信息
170
项与 Pritzker School of Medicine 相关的文献(医药)2025-12-01·American Journal of Hospice & Palliative Medicine
Differences in Inpatient Palliative Care Consultation During the Terminal Admission for Pediatric Neuro-Oncology Patients
Article
作者: Hoehn, K. Sarah ; Udemgba, Chinwe S. ; Palama, Brett K. ; Darlington, Wendy
Pediatric neuro-oncology patients have one of the highest mortality rates among all children with cancer. Our study examines the potential relationship between palliative care consultation and intensity of in-hospital care and determines if racial and ethnic differences are associated with palliative care consultations during their terminal admission. Retrospective observational study using the Pediatric Health Information System (PHIS) database with data from U.S. children’s hospitals. PHIS was queried for patients under 18 years of age who received a diagnosis of brain tumor and had their terminal admission between January 1, 2017 and December 31, 2021. Of the 567 patients who fit the inclusion criteria, 359 (63%) patients had an inpatient palliative care consultation during their terminal hospital stay. There were no statistically significant differences seen when comparing palliative care consultation rates among racial groups. When comparing the ethnicity variables, patients in the Hispanic group had approximately a 10% higher rate of palliative care consultations than their non-Hispanic counterpart. Patients with palliative care consultations had a lower percentage of PICU admission (64.9 vs 83.2), mechanical ventilation (51.0 vs 76.0), and TPN use (18.1 vs 25.5) despite having similar lengths of stay. Pediatric neuro-oncology patients who received a palliative care consultation during their terminal hospital stay had lower intensity care (lower rates PICU admission, mechanical ventilation use, and TPN use) despite having similar lengths of stay. This may reflect the enhanced decision-making support for the patients and their families so that they may consider all options. Children facing a terminal illness and their families deserve access to optimal supportive services. This study highlights the importance of integrating palliative care in hospital admissions of terminally ill children with neuro-oncological diagnoses.
2025-11-19·JOURNAL OF ORTHOPAEDIC TRAUMA
The Impact of Gunshot Injury on the Development of Heterotopic Ossification after Periarticular Elbow Trauma
Article
作者: Sethi, Sahil ; Strelzow, Jason ; Reddy, Sai Kashyap ; Pathuri, Manish ; Christiano, Anthony
OBJECTIVES::
To evaluate whether ballistic (gunshot) injuries increase the rate of severity of heterotopic ossification (HO) compared to blunt trauma in patients with peri-articular elbow fractures.
METHODS::
Design: Retrospective Cohort
Setting::
Single Level 1 Trauma Center
Patient Selection Criteria::
Study inclusion required; patients of mature skeletal age diagnosed with a peri-articular elbow fracture (OTA/AO 13A-C) with a minimum of 6-weeks radiographic follow-up between 2018-2024.
Outcome Measures and Comparisons::
Data on demographics, injury characteristics, and surgical management were collected for the ballistic trauma cohort and blunt trauma cohort. HO was assessed using the Hastings/Brooker Classification. Secondary outcomes included post-injury stiffness defined as a flexion/extension arc of motion < 100°, revision surgery, and complications. Descriptive statistics were used to compare frequencies of categorical outcome variables between blunt and ballistic cohorts, and multivariable logistic regressions were used to identify risk factors for elbow HO occurrence and severity as well as all secondary outcomes.
RESULTS::
A total of 171 patients met inclusion criteria including 65 GSW-related fractures (38%). GSW patients were younger (29.2 [Range: 18-62] vs. 43.8 years [Range: 18-93]) and more often male (84.6% vs 51.9%). Overall HO occurrence was 61.4%. GSW was not significantly associated with HO (63.1% vs. 60.4%,
p
=0.607). Distal humerus fractures were associated with increased HO risk (OR 2.15) and severity (OR 2.63) compared to proximal radius/ulna injuries. Stiffness occurred in 73.7% of patients and was more common in distal humerus injuries than proximal radius/ulna fractures (OR 2.50;
p
= 0.030). No significant differences were found in stiffness, revision surgery, or complication rates between GSW and non-GSW groups (OR 1.36; 95% CI: 0.537-3.455;
p
=0.51).
CONCLUSIONS::
Ballistic injury did not significantly increase heterotopic ossification risk or stiffness compared to blunt trauma in a civilian population. Consistent with prior literature, fracture location, specifically distal humerus fractures compared to proximal radius/ulna injuries, appears to be an important driver for heterotopic ossification prevalence and severity. Identifying heterotopic ossification risk factors after peri-articular elbow trauma can help clinicians stratify patient risk and guide preventive strategies for managing these complex injuries.
LEVEL OF EVIDENCE::
Level III
2025-11-01·JOURNAL OF ORTHOPAEDIC TRAUMA
Percutaneous Anterior Pelvic Ring Fixation in Addition to Percutaneous Posterior Pelvic Ring Fixation Decreases Postoperative Pain and Narcotic Usage in Hospital for Lateral Compression Types 1 and Lateral Compression Type 2 Injuries
Article
作者: Lee, Jackson ; Lee, Adam ; Marecek, Geoffrey ; Wier, Julian ; Patterson, Joseph T. ; Kumaran, Pranit ; Gary, Joshua L.
Objectives::
To compare postoperative pain and opioid requirements between lateral compression types 1 (LC1) and lateral compression type 2 (LC2) injuries treated with anterior and posterior fixation (PF) [anterior fixation (AF) + PF] versus PF only.
Methods::
.
Design::
Retrospective review of propensity matched cohorts for sex, age, LC1 versus LC2, sacral fracture type, and preoperative Visual Analogue Scale (VAS) pain scores were created in a 1:1 ratio.
Setting::
Level 1 trauma center and academic tertiary care hospital.
Patient Selection Criteria::
Adult patients with LC1 or LC2 (OTA/AO 61B2.1, 61B2.2) injuries treated surgically with PF or AF + PF between March 2019 through January 2024.
Outcome Measures and Comparisons::
VAS and morphine milligram equivalents (MMEs) were measured at 24 and 48 hours postoperatively, and 24 hours before discharge between the groups. Secondary outcomes included postoperative days to mobilization (DTM) and length of stay.
Results:Intotal,:
56 patients (28 AF + PF, mean age 49.4 ± 16.9, 57.1% female, 28 PF, mean age 49.8 ± 16.9, 53.6% female) were included. There were no differences between the groups for demographic data (all P > 0.78). Patients with AF + PF had lower VAS scores than patients with PF 24 hours postoperatively [difference in mean (DIM): 2.18 cm (95% confidence interval (95% CI): 0.9068–3.4532], P = 0.001), 48 hours postoperatively [DIM: 3.43 cm (95% CI: 2.11 to 4.75), P < 0.001] and 24 hours before discharge [DIM: 2.68 (95% CI: 1.31 to 4.04), P < 0.001]. Patients with AF + PF required lower MMEs 24 hours before discharge [DIM: 6.989 (95% CI: 0.873 to 13.105), P = 0.026]. Patients with AF + PF also had shorter DTM [DIM: 3.21 (95% CI: 0.03 to 6.40), P = 0.048]. There were no differences in MMEs 24 hours postoperatively [DIM: 3.64 (95% CI: −4.15 to 11.44), P = 0.35], 48 hours postoperatively [DIM: 4.78 (95% CI: −3.12 to 12.67), P = 0.23], or length of stay [DIM: 1.96 (95% CI: −2.03 to 5.95), P = 0.33].
Conclusions::
Anterior and posterior fixation was associated with significantly decreased inpatient postoperative pain, predischarge narcotics use, and DTM compared with PF alone. The combination of percutaneous AF and PF for LC1 and LC2 pelvic ring injuries should be considered when the goals are maximizing pain control.
LEVEL OF EVIDENCE::
Therapeutic Level III. See Instructions for Authors for a complete description of levels of evidence.
27
项与 Pritzker School of Medicine 相关的新闻(医药)2025-12-04
编者按:2025年,药明康德迎来创立25周年的重要里程碑。值此契机,我们向所有与我们共同书写产业变革篇章的科学家、医药人和投资者致以衷心感谢与诚挚敬意,也特别推出“致敬时代”系列,回顾全球同仁如何借助科学与合作的力量,不断拓展治疗边界、改善患者命运。
四分之一个世纪的坚守,只为加速每一款新药的诞生。下一个25年,我们将继续心怀感恩与敬畏,依托独特的CRDMO模式,与全球伙伴携手同行,共赴健康未来。
1853年,伦敦医院,一名53岁的男子在与病魔抗争了3年后去世,外科医生John Adams为了搞清楚病因,做了尸检,发现凶手隐藏在患者的前列腺中。Adams在病理报告里写道,患者的前列腺发生了硬化,他进一步评论,这是一种很罕见的疾病。
这是医学史上第一例通过病理检验确诊的前列腺癌。但Adams恐怕不会想到150多年后,自己发现的这种疾病将会成为男性中最常见的癌症之一。2020年,前列腺癌在112个国家中位列男性癌症发病率首位,每年新增病例约140万,占男性癌症的15%,造成约40万人死亡。
前列腺癌发病率确实出现了大幅增加,而且这种上升趋势很可能还会继续,研究预计到2040年,全球每年新增前列腺癌将达290万。
为什么前列腺癌越来越多?背后有多个因素。首先是诊断手段的进步。直到20世纪初,前列腺癌才与其他类型的尿路梗阻区分开来,而如今,通过前列腺特异性抗原(PSA)筛查,临床上可以发现非常早期的前列腺癌。
其次是老龄化趋势。前列腺癌的发病率与年龄密切相关,而且这种随年龄增长的增速几乎超过所有癌症。
其三则与生活方式有关。流行病学研究显示亚洲男性的前列腺癌发病率低于西方,但移居欧美的亚裔男性风险显著上升,提示饮食或环境因素可能影响前列腺癌的发病率。
不过,值得欣慰的是,过去几十年里,前列腺癌的诊疗突飞猛进。对很多患者来说,前列腺癌的确诊报告早已不再是一份宣告生命即将结束的“判决书”。
图片来源:123RF
作为全球医药及生命科学行业值得信赖的合作伙伴和重要贡献者,药明康德在过去25年发展历程中,很荣幸见证了多款前列腺癌创新疗法从实验室到临床的突破历程,更通过提供一体化、端到端的新药研发和生产服务,助力全球合作伙伴加速多款前列腺癌创新疗法的研发进程、造福病患。今天这篇文章将回望前列腺癌创新疗法的发展历程,向那些拯救无数患者的英雄们致敬。
诺奖级发现打破治疗僵局
医学界很早就对前列腺癌发起了挑战,1904年,泌尿科先驱,后来创办了《泌尿外科杂志》(The Journal of Urology)的Hugh Hampton Young博士做了全球首例前列腺根治性切除术。1909年,Young博士报告了19例手术预后,15位患者症状几乎完全缓解,有1位患者术后存活超过5年,可能已被治愈。前列腺根治性切除至今仍是早期前列腺癌的关键治疗手段。
同一时期,居里夫妇发现了镭、钋这两个放射性元素后掀起的放疗研究热进入前列腺癌治疗。法国泌尿科医生Henri Minet尝试用含镭的导管经尿道或耻骨上导管治疗前列腺癌,近距离放疗成了最早用于前列腺治疗的放疗手段。
然而,这些早期突破后,前列腺癌的治疗很快陷入僵局。受限于早期放疗技术缺陷,操作过程对患者来说极痛,难以在前列腺癌中推广。而手术对于已经出现癌细胞转移的晚期前列腺癌患者也意义有限。
20世纪中期,泌尿科医生面对的典型前列腺癌患者会是一位70岁刚出头的老人,癌细胞已经转移到骨骼或软组织。这在当时几乎等于被判了死刑,患者通常在1-2年里就会被癌症夺去生命。
但前列腺癌治疗的革命性突破即将在一所建立不久的医学院里诞生。1927年,刚做完普外科住院医师培训,年仅26岁加拿大裔美国医生Charles Brenton Huggins被招募到刚成立的芝加哥大学医学院,作为整个医学院最初的8名员工之一,Huggins博士被分配到了泌尿科,被迫迅速自学专科知识。
整个30年代,他不断深入研究包括前列腺在内的男性泌尿系统器官。厚积薄发,1940-41年,Huggins博士与他的两名学生连续发表了3篇论文,阐述通过睾丸切除术或雌激素治疗来抑制雄激素活性,可以让许多转移性前列腺癌患者的肿瘤缩小。那些接受治疗的患者短短几天内疼痛就得到了显著缓解,最初接受治疗的21人中,有4人存活超过12年!
Huggins博士的发现开启了前列腺癌治疗的全新时代:去势治疗。由于超过80%的前列腺癌对雄激素存在依赖,去势治疗可以缓解绝大部分患者的病痛。Huggins也因此获得1966年诺贝尔生理学或医学奖。值得一提的是,他提出的口服雌激素药物去势疗法还是第一个有效的全身性癌症治疗方法,是晚期肿瘤治疗的划时代突破。而对于广大前列腺患者,时至今日,Huggins博士开启的去势疗法仍然是最普遍有效的治疗方法。
▲Charles Brenton Huggins博士(图片来源:Nobel Foundation archive)
从LHRH激动剂到拮抗剂
尽管口服雌激素与睾丸切除术开启了前列腺癌治疗的全新时代,但很快这些去势手段的局限性就显现了出来,首先是口服雌激素降低血清睾酮水平会导致显著的心血管毒性,增加血栓风险。其次,通过去势或雌激素治疗来消除雄激素,也不足以治愈晚期前列腺癌。
显然,需要寻找更好的去势治疗手段,而这需要另一个诺奖级别的突破。
1971年,美国科学家Andrew Schally用了16万头猪的下丘脑,分离出800微克的一种名为促黄体生成素释放激素(LHRH)的下丘脑激素。这种激素能刺激脑垂体释放黄体生成素(LH),后者又能与睾丸上的受体结合,激活雄激素睾酮合成。
有趣的是,Schally博士发现尽管LHRH激动剂会导致血清睾酮短暂升高,但长期使用会产生抑制作用,下调垂体LHRH受体,降低血清睾酮,与去势手术相当。于是,他尝试将LHRH激动剂用于前列腺癌患者治疗,发现可以显著缓解癌症相关的骨痛。
▲Andrew Schally博士(图片来源:Nobel Foundation archive)
1977年,Schally博士获得了诺贝尔生理学或医学奖。1985年,FDA批准了第一个用于治疗晚期前列腺癌的LHRH激动剂Lupron(leuprolide,亮丙瑞林),之后,Zoladex(goserelin,戈舍瑞林)、Trelstar(triptorelin acetate,醋酸曲普瑞林)相继上市。70-80%的前列腺癌患者使用这些LHRH激动剂后,肿瘤能被有效抑制,同时,这些药物没有口服激素带来的心血管、血栓风险,至今仍是优先使用的去势治疗手段。
可是,LHRH激动剂也有缺点,如同Schally博士当初观察到的,这类药物刚开始使用时会先增加体内睾酮合成,导致有些前列腺癌患者将经历癌症恶化。于是,业界开始寻找LHRH拮抗剂。
2008年,Firmagon(degarelix,地加瑞克),这种皮下注射的LHRH拮抗剂获批上市,让患者能更快降低血清睾酮,避免了去势治疗初始阶段因睾酮短暂升高而出现癌症恶化的风险。2020年,全球首个口服LHRH拮抗剂Orgovyx(relugolix,瑞卢戈利)获批,又为患者提供了一种更便捷的治疗选择。
突破重重困难的抗雄激素
就在Schally研究LHRH的同一时期,60年代末,科学家发现了雄激素受体,这无疑带来了新的潜在去势疗法研发方向。无论是LHRH激动剂还是拮抗剂,都存在影响性功能、导致潮热等副作用,靶向雄激素受体的抗雄激素(雄激素受体拮抗剂)或许能避免这些副作用。很快科学家们找到了一个甾体类抗雄激素,cyproterone(环丙孕酮)。
科学家们对这第一个抗雄激素充满期望,但挫折很快到来:环丙孕酮能透过血脑屏障,它不仅和前列腺癌细胞上的雄激素受体结合,还与下丘脑和垂体上的雄激素受体结合,阻断雄激素合成的负反馈。这导致环丙孕酮治疗的最终结局是增加血清睾酮,没法起到去势作用。
研究人员想了个对策:添加乙酸酯基团,合成Androcur(cyproterone acetate,醋酸环丙孕酮)。醋酸环丙孕酮保留了雄激素拮抗作用,作用于前列腺癌细胞;同时它也是一种孕激素激动剂,能与垂体中的孕激素受体结合,间接降低血清睾酮水平。这种双机制治疗的有效性与口服雌激素大致相当,1973年在欧洲获批上市。
可是,人们发现醋酸环丙孕酮还是有局限性:它对雄激素分泌的影响会导致性欲减退和性功能障碍。业界开始寻找非甾体类的抗雄激素,以避免这些副作用。
图片来源:123RF
Eulexin(flutamide,氟他胺)成为第一个进入临床试验的非甾体类抗雄激素,并于1989年获得FDA批准用于前列腺癌治疗。它和90年代获得FDA批准的Casodex(bicalutamide,比卡鲁胺)、Nilandron(nilutamide,尼鲁米特)组成了第一代抗雄激素,或第一代雄激素受体拮抗剂。
尽管第一代抗雄激素如研究人员期望的,副作用更小,可是后续研究发现它们和环丙孕酮一样,最终还是会穿过血脑屏障,增加LH释放,进而导致血清睾酮升高。在转移性前列腺癌患者的随机试验中,研究人员发现单独使用第一代抗雄激素治疗,与其它药物或去势手术去势相比,尽管耐受性更好,但在总生存期和无进展生存期上,并无优势。
虽有缺陷,但随着第一代抗雄激素的出现,那些LHRH激动剂或拮抗剂治疗无效的患者,可以加入抗雄激素,或者在一开始治疗时就采用LHRH激动剂加抗雄激素的联合雄激素阻断,都能获得更好的治疗效果。
两代抗雄激素改写去势抵抗性前列腺癌治疗格局
不过,即便有了LHRH激动剂、拮抗剂以及第一代抗雄激素,大部分前列腺癌患者治疗后仅能获得几年的缓解,之后肿瘤就会出现耐药,发展成去势抵抗性前列腺癌,最终成为夺走患者生命的主要原因。很长一段时间里,去势抵抗性前列腺癌患者只能依赖多西他赛、卡巴他赛这些化疗,疗效也不理想。面对困难,医药界人士并未低头,研究发现去势抵抗性前列腺癌细胞大多是出现了雄激素受体扩增、点突变、剪接变体表达。不是抑制雄激素信号通路不行,而是第一代抗雄激素抑制不了这些改变了的雄激素信号通路,甚至,第一代抗雄激素在长期使用后能从拮抗剂转为激动剂的缺点还将帮倒忙。
患者需要的是新一代抗雄激素。
而在2010年后,前列腺癌治疗迎来了一个新药井喷期:多个第二代抗雄激素陆续上市,彻底改变了去势抵抗性前列腺癌的治疗格局。
图片来源:123RF
首先打破僵局的是2011年获得FDA批准的Zytiga(abiraterone,阿比特龙),它是一种很特殊的抗雄激素,并不直接作用于雄激素受体,而是抑制雄激素合成。在转移性去势抵抗性前列腺癌的临床试验里,阿比特龙将患者的总生存时间从安慰剂组的10.4个月提升到了15.4个月。
阿比特龙只是一个开始,紧接着2012年,Xtandi(enzalutamide,恩扎卢胺)获得FDA批准,这是一类全新的雄激素受体拮抗剂,不像第一代抗雄激素那样会出现拮抗剂到激动剂的转变。在对化疗耐药的去势抵抗性前列腺癌患者中,临床试验显示恩扎卢胺治疗的总生存期达18.3个月,比安慰剂组的13.6个月有大幅提高。
不过,研究人员发现高剂量恩扎卢胺存在癫痫风险,这又成了后续第二代抗雄激素研发的指引。2018年,Erleada(apalutamide,阿帕他胺)获得FDA批准,它更少透过血脑屏障,缓解了癫痫风险。
2019年,Nubeqa(darolutamide,达罗他胺)成为最新一个获得FDA批准的二代抗雄激素。达罗他胺对所有已知的雄激素受体突变都能维持抑制作用,即便是能导致恩扎卢胺、阿帕他胺耐药的突变也不例外,使它成了应对耐药问题的利器。
2022年与2025年,中国国家药品监督管理局分别批准艾瑞恩(rezvilutamide,瑞维鲁胺)与海纳安(enzalutamide deuterated,氘恩扎鲁胺)上市,这些二代抗雄激素又为患者带来更多选择。
精准治疗进入前列腺癌
针对肿瘤特定分子特征的精准治疗是过去20多年癌症治疗的巨大突破,但很长一段时间里,前列腺癌的精准治疗一直处于空白状态。
前列腺癌就没有精准治疗可以打击的分子特征吗?
一类基因突变引发了业界注意——DNA损伤修复(DDR)基因异常。在乳腺癌、卵巢癌中,基于“合成致死”机制开发的PARP抑制剂是针对BRCA1/2突变或其他DDR异常的有效治疗手段。而研究显示,高达11.8%的晚期前列腺癌患者存在DDR种系变异,约23%的转移性去势抵抗性前列腺癌存在ATM、CHEK2、BRCA1、BRCA2等DDR基因突变。
PARP抑制剂或许对部分前列腺癌患者也能有效!
临床研究证实了这一点。一项在转移性去势抵抗性前列腺癌患者中展开的3期临床试验显示,对于具有BRCA1、BRCA2或ATM中任意一类突变的患者,使用Lynparza(olaparib,奥拉帕利)治疗,患者无进展生存期为7.4个月,远高于使用二代抗雄激素的对照组(3.6个月)。奥拉帕利降低患者癌症进展或死亡的风险达66%。
2020年,奥拉帕利以及Rubraca(rucaparib,芦卡帕利)获得FDA批准用于具有特定DDR异常的转移性去势抵抗性前列腺癌。2023年,另外两个PARP抑制剂Talzenna(talazoparib,他拉唑帕利)和Zejula(niraparib,尼拉帕尼)也进入前列腺癌治疗。
前列腺癌不再是精准治疗的荒漠。
两代免疫治疗造福患者
免疫治疗是另一项近年来深刻改变癌症治疗格局的重大突破。而早在2010年,前列腺癌患者就迎来了第一个免疫治疗:Provenge(sipuleucel-T)。它其实是一种癌症疫苗。从患者血液里分离出来的白细胞会在实验室里和前列腺癌细胞的一种蛋白质,前列腺酸性磷酸酶(PAP)混合,然后这些接受了抗原刺激的白细胞被回输到患者体内,增加对前列腺癌细胞的杀伤。
3期临床试验中,接受sipuleucel-T治疗的转移性去势抵抗性前列腺癌患者的中位生存期为25.9个月,优于安慰剂治疗的21.4个月中位生存期。而与sipuleucel-T类似的另一种自体免疫治疗Apceden也于2017年在印度获批上市。
尽管比很多实体瘤都更早收获免疫治疗,但令人遗憾的是对于大部分前列腺癌患者,以PD-1单抗为代表的肿瘤免疫治疗并不适用。可对少数幸运的患者,情况不同。
2017年,FDA划时代地批准了Keytruda(pembrolizumab,帕博利珠单抗)用于治疗微卫星不稳定性高或错配修复缺陷(MSI-H/dMMR)的癌症,不限癌种。该批准的基础是临床研究发现无论癌症起源于哪个器官,只要具有MSI-H/dMMR这一分子特征,就能从帕博利珠单抗治疗中获益。
从此,具有该分子特征的前列腺癌患者也有了新的治疗选择。此后,更多PD-1/PD-L1抗体,如Jemperli(dostarlimab)、百泽安(tislelizumab,替雷利珠单抗)、恩维达(envafolimab,恩沃利单抗)、普佑恒(pucotenlimab,普特利单抗),也都获批用于MSI-H/dMMR实体瘤治疗。
MSI-H/dMMR在前列腺癌中比较罕见,可对于那少数患者,免疫治疗带来了新的希望。
前列腺癌治疗迎来“定点靶向”放疗
虽然过去20年,去势治疗、精准治疗以及免疫治疗的发展让晚期前列腺癌患者有了很多治疗选择,但转移性去势抵抗性前列腺癌尚无法治愈,这使得那些接受多种治疗后出现疾病进展的患者,亟需新的疗法。
科学家将目光投向了前列腺特异性膜抗原(PSMA),一种在前列腺癌细胞上高表达的跨膜酶,而且大多数转移性去势抵抗性前列腺癌患者的转移灶也表达PSMA,使它成了靶向前列腺癌的优良选择。
箭有了,可配什么箭头能最大程度杀伤癌细胞呢?
这次,研究人员想到了放疗。2006年,美国普渡大学的科学家设计了一种高亲和力的PSMA配体,并提出给该配体连接放射性药物的设计。2012年,德国的研究人员又进一步改善了这种配体的亲和力。
一种全新的药物,结合放射性同位素镥177的PSMA高亲和力配体,逐渐成型。
经过多年临床研究,2022年,前列腺癌治疗迎来了又一变革:FDA批准了第一个用于治疗转移性去势抵抗性前列腺癌的放射性配体药物:Pluvicto(lutetium Lu 177 vipivotide tetraxetan,镥[177Lu]-特昔维匹肽)。
在相关的3期临床研究中,晚期PSMA阳性转移性去势抵抗性前列腺癌患者被随机分配至镥[177Lu]-特昔维匹肽联合标准治疗组或标准治疗组。结果显示,联合治疗组总生存期达15.3个月,显著高于标准治疗组的11.3个月。联合治疗降低死亡风险达38%。而且,联合治疗组中患者的总缓解率达到30%,而只接受标准治疗患者的缓解率仅为2%。
镥[177Lu]-特昔维匹肽的出现是放射性配体药物的重大突破,也为那些穷尽过往治疗手段的晚期前列腺癌患者带来了新的选择。
更多新药研发已在路上
前列腺癌作为男性中发病率最高的癌症之一,曾经夺去无数人的生命。1960年代,即便在欧美发达国家,50-60%的前列腺癌确诊患者生存时间不超过5年。但是,随着去势治疗的不断发展,以及精准治疗、免疫治疗乃至放射性配体药物的出现,仅在过去25年间,全球监管机构便批准了至少20款创新疗法,为无数前列腺癌患者带来了新生,如今90%以上的前列腺癌患者可以实现长期生存。
然而,由于发病率高,前列腺癌尤其是尚无法治愈的转移性去势抵抗性前列腺癌,每年仍造成大量死亡。患者仍然需要疗效更优的治疗方案。好消息是,众多创新机制的疗法已在路上。例如前文提到的基于“合成致死”机制的靶向疗法,目前研发管线中约有40款新药,靶点涵盖PARP、EZH2、ATR、PLK1、POLQ、USP1、PRMT5等。而放射性配体药物方面,全球也有40余款创新药正在临床阶段探索治疗前列腺癌的潜力,靶点主要为PSMA,还包括SSTR2、GRPR、DLL3、NTSR1、KLK2等。靶向配体形式涵盖小分子、抗体与多肽,所用放射性同位素包括Lu 177、Ac 225、Ga 68、In 111等。
此外,靶向蛋白降解药物(TPD)有望成为克服传统雄激素受体拮抗剂耐药性的新生力量。它们通过直接降解雄激素受体蛋白,可更深度、持久地抑制该信号通路。例如,Arvinas公司开发的第二代雄激素受体靶向蛋白降解嵌合体(PROTAC®)ARV-766,在早期临床试验中已表现出能够选择性降解野生型和带有临床耐药相关突变的雄激素受体的能力。公开资料显示,目前已有10多款TPD疗法进入临床阶段,用于治疗前列腺癌。
在助力各类疗法从创新概念走向临床验证的过程中,药明康德致力于支持全球客户加速研发进程,凭借CRDMO平台能够“端到端”助力各类分子从发现、到开发,再到生产交付的全过程。以放射性配体药物为例,药明康德综合性的放射性药物发现平台整合了多肽发现和放射性药物开发能力,提供包括多肽合成、螯合剂合成、放射性标记、成像、药理学研究和监管申报支持等完善的服务。一体化平台能够让多个团队并行攻坚、高度协作,帮助合作伙伴快速推动项目进展,节省宝贵的开发时间。在TPD药物开发方面,药明康德已经助力70多种TPD分子进入临床前候选药物(PCC)阶段,10多种已进入后期开发阶段。
展望下一个25年,我们期待与产业同道继续并肩前行,突破更多疾病领域的治疗瓶颈,将更多创新疗法更快带到患者身边。
参考资料(可上下滑动查看)
[1] Denmeade, S., Isaacs, J. A history of prostate cancer treatment. Nat Rev Cancer 2, 389–396 (2002). https://doi.org/10.1038/nrc801
[2] Lehtonen M, Kellokumpu-Lehtinen P-L. The past and present of prostate cancer and its treatment and diagnostics: A historical review. Sage Open Medicine. 2023;11. doi:10.1177/20503121231216837
[3] Mallah H, Diabasana Z, Soultani S, Idoux-Gillet Y, Massfelder T. Prostate Cancer: A Journey Through Its History and Recent Developments. Cancers. 2025; 17(2):194. https://doi.org/10.3390/cancers17020194
[4] James, Nicholas D et al. The Lancet Commission on prostate cancer: planning for the surge in cases. The Lancet, Volume 403, Issue 10437, 1683 - 1722
[5] Rice MA, Malhotra SV, Stoyanova T. Second-Generation Antiandrogens: From Discovery to Standard of Care in Castration Resistant Prostate Cancer. Front Oncol. 2019 Aug 28;9:801. doi: 10.3389/fonc.2019.00801.
[6] De Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102.
[7] Keam, S.J. Lutetium Lu 177 Vipivotide Tetraxetan: First Approval. Mol Diagn Ther 26, 467–475 (2022). https://doi.org/10.1007/s40291-022-00594-2
免责声明:本文仅作信息交流之目的,文中观点不代表药明康德立场,亦不代表药明康德支持或反对文中观点。本文也不是治疗方案推荐。如需获得治疗方案指导,请前往正规医院就诊。版权说明:欢迎个人转发至朋友圈,谢绝媒体或机构未经授权以任何形式转载至其他平台。转载授权请在「药明康德」微信公众号回复“转载”,获取转载须知。
分享,点赞,在看,传递医学新知
2025-11-28
·医药观澜
编者按:前列腺癌是男性中最常见的癌症之一。近年来,一系列创新疗法的获批,深刻变革了这一疾病的治疗格局。面对临床上目前尚未满足的治疗需求和挑战,当下还有数百项新药管线正在临床研究中探索治疗前列腺癌的潜力。作为全球医药及生命科学行业值得信赖的合作伙伴和重要贡献者,药明康德在过去25年发展历程中,很荣幸见证了多款前列腺癌创新疗法从实验室到临床的突破历程,更通过提供一体化、端到端的新药研发和生产服务,助力全球合作伙伴加速包括前列腺癌在内的各类癌症创新疗法的研发进程、造福病患。
前列腺癌是男性中最常见的癌症之一。随着诊疗手段的进步、人口老龄化趋势等,前列腺癌发病率还在大幅增加。
值得欣慰的是,过去几十年里,前列腺癌的诊疗也在“突飞猛进”。去势治疗、靶向疗法、免疫疗法以及放射性配体药物等一系列创新疗法的问世深刻变革了这一疾病的治疗格局。1960年代,即便在欧美发达国家,50-60%的前列腺癌确诊患者生存时间不超过5年。如今,90%以上的前列腺癌患者可以实现长期生存。
今天这篇文章将回望前列腺癌创新疗法的发展历程,向那些拯救无数患者的英雄们致敬。
图片来源:123RF
诺奖级发现打破前列腺癌治疗僵局
医学界对前列腺癌的探索始于二十世纪初。1904年,泌尿科先驱Hugh Hampton Young博士完成了全球首例前列腺根治性切除术。这一术式至今仍是早期前列腺癌的关键治疗方式。与此同时,放疗研究热潮兴起,并应用于前列腺癌治疗。
由于早期放疗技术尚不成熟,操作过程给患者带来巨大痛苦,难以广泛应用;而手术对已发生转移的晚期患者效果也十分有限。在二十世纪中期,一名70岁出头、已出现骨或软组织转移的前列腺癌患者,往往等于被宣判死刑,生存期通常仅有1~2年。
1940至1941年间,芝加哥大学医学院Charles Brenton Huggins医生与两名学生连续发表三篇论文,指出通过睾丸切除术或雌激素治疗以抑制雄激素活性,可使许多转移性前列腺癌患者的肿瘤缩小。
Huggins的发现开启了前列腺癌治疗的新纪元——去势治疗。由于超过80%的前列腺癌依赖雄激素,去势治疗能缓解绝大多数患者的病情。这一贡献使Huggins荣获1966年诺贝尔生理学或医学奖。值得一提的是,他提出的口服雌激素药物去势疗法也是第一个有效的全身性癌症治疗方法。直至今日,去势疗法仍是前列腺癌最普遍且有效的治疗手段之一。
LHRH激动剂与拮抗剂
口服雌激素与睾丸切除术开启了前列腺癌治疗的全新时代,但这些去势手段的局限性很快显现:口服雌激素在降低血清睾酮的同时,会引发显著的心血管毒性并增加血栓风险;此外,单纯消除雄激素仍不足以治愈晚期前列腺癌。
医学界亟需更安全有效的去势疗法,而这一需求最终催生了另一项诺奖级的突破。
1971年,美国科学家Andrew Schally博士历时艰苦实验,从16万头猪的下丘脑中成功分离出800微克名为“促黄体生成素释放激素(LHRH)”的激素。该激素可刺激脑垂体释放黄体生成素(LH),进而激活睾丸合成雄激素睾酮。
有趣的是,Schally博士发现,虽然LHRH激动剂在初期会引起血清睾酮短暂升高,但长期使用却能抑制垂体LHRH受体功能,最终使血清睾酮降至去势手术相当的水平。基于这一发现,他将LHRH激动剂用于前列腺癌患者的治疗,并观察到患者癌症相关骨痛得到显著缓解。
这一重大成果使沙利博士于1977年荣获诺贝尔生理学或医学奖。1985年,FDA批准了第一个用于治疗晚期前列腺癌的LHRH激动剂Lupron(leuprolide,亮丙瑞林)。随后,Zoladex(goserelin,戈舍瑞林)和Trelstar(triptorelin acetate,醋酸曲普瑞林)相继上市。这类药物能使70–80%患者的肿瘤得到有效抑制,且避免了口服雌激素的心血管与血栓风险,至今仍是去势治疗的首选方案之一。
然而,LHRH激动剂也存在缺点:正如沙利博士最初所观察到的,用药初期睾酮的短暂升高可能导致部分患者病情恶化。为此,科研人员转向研发LHRH拮抗剂。
2008年,皮下注射型LHRH拮抗剂Firmagon(degarelix,地加瑞克)获批上市,它能快速降低血清睾酮,避免治疗初期因睾酮升高带来的癌症恶化风险。2020年,全球首个口服LHRH拮抗剂Orgovyx(relugolix,瑞卢戈利)问世,为患者提供了更为便捷的治疗选择。
图片来源:123RF
抗雄激素药物开辟全新方向
在沙利博士研究LHRH的同一时期,上世纪60年代末,科学家成功发现了雄激素受体,这为去势治疗开辟了全新方向。由于LHRH激动剂和拮抗剂常伴随影响性功能、引发潮热等副作用,研究人员将目光转向靶向雄激素受体本身的抗雄激素药物(即雄激素受体拮抗剂),期望能避免上述问题。不久,首个甾体类抗雄激素——环丙孕酮(cyproterone)问世。
科学界对这款抗雄激素寄予厚望,但很快发现其能够透过血脑屏障,不仅作用于前列腺癌细胞上的雄激素受体,还会与下丘脑和垂体中的受体结合,阻断雄激素合成的负反馈调节,最终反而导致血清睾酮水平上升,无法实现去势治疗效果。
为克服这一局限,研究人员尝试在其分子中引入乙酸酯基团,合成了Androcur(cyproterone acetate,醋酸环丙孕酮)。该药物既保留了对前列腺癌细胞的雄激素拮抗作用,又可作为孕激素激动剂作用于垂体孕激素受体,从而间接降低血清睾酮。凭借这一双重机制,其疗效与口服雌激素大致相当,并于1973年在欧洲获批上市。
然而,Androcur仍存在局限性,尤其是其对雄激素分泌的影响会导致性欲减退和性功能障碍。因此,行业开始转向研发非甾体类抗雄激素,以期减少此类副作用。
Eulexin(flutamide,氟他胺)成为首个进入临床试验的非甾体类抗雄激素,于1989年获美国FDA批准用于前列腺癌治疗。随后在90年代,Casodex(bicalutamide,比卡鲁胺)、Nilandron(nilutamide,尼鲁米特)也相继获批,共同构成了第一代抗雄激素药物,也称为第一代雄激素受体拮抗剂。
尽管副作用更小,后续研究却发现第一代抗雄激素与环丙孕酮类似,仍能穿过血脑屏障,促进黄体生成素释放,导致血清睾酮升高。此外,在针对转移性前列腺癌的随机试验中,单独使用第一代抗雄激素治疗,虽然在耐受性上优于其他药物或去势手术,但在总生存期和无进展生存期方面并未显示出优势。
尽管存在这些缺陷,第一代抗雄激素的出现仍为治疗策略带来重要补充。对于LHRH激动剂或拮抗剂疗效不足的患者,可联合使用抗雄激素药物,或在初始治疗阶段即采用“LHRH激动剂+抗雄激素”的联合雄激素阻断方案,从而获得更好的治疗效果。
改写去势抵抗性前列腺癌治疗格局
尽管已有上述疗法,大多数前列腺癌患者在治疗后仅能获得数年缓解,随后肿瘤便会产生耐药,进展为去势抵抗性前列腺癌,这成为最终导致患者死亡的主要原因。在很长一段时间里,这类患者只能依赖多西他赛、卡巴他赛等化疗药物,疗效仍不理想。
进一步研究发现,去势抵抗性前列腺癌细胞大多出现雄激素受体扩增、点突变或剪接变体表达等问题。这意味着并非雄激素信号通路抑制本身无效,而是第一代抗雄激素难以抑制这些变异后的信号通路。更甚的是,长期使用第一代抗雄激素后,部分药物可能从拮抗剂转变为激动剂,反而促进肿瘤进展。这意味着,患者迫切需要新一代抗雄药物。
2010年后,前列腺癌治疗迎来新药爆发期:多个第二代抗雄激素相继上市,彻底改变了去势抵抗性前列腺癌的治疗格局。比如,2011年获FDA批准的Zytiga(abiraterone,阿比特龙)是一种特殊类型的抗雄激素,它不直接作用于雄激素受体,而是通过抑制雄激素合成发挥作用。
图片来源:123RF
紧随其后,Xtandi(enzalutamide,恩扎卢胺)于2012年获FDA批准。作为新机制的雄激素受体拮抗剂,它不会出现从拮抗剂向激动剂转变的现象,然而高剂量恩扎卢胺存在诱发癫痫的风险,这为后续药物研发提供了重要参考。2018年,Erleada(apalutamide,阿帕他胺)获FDA批准,其更少透过血脑屏障,从而有效降低了癫痫风险。
2019年,Nubeqa(darolutamide,达罗他胺)成为最新获批的二代抗雄激素。该药物对所有已知的雄激素受体突变均保持抑制作用,甚至对导致恩扎卢胺和阿帕他胺耐药的突变也有效,使其成为应对耐药问题的重要工具。
此外,中国NMPA于2022年与2025年分别批准艾瑞恩(瑞维鲁胺)与海纳安(氘恩扎鲁胺)上市,进一步丰富了患者的治疗选择。
“合成致死”机制破局前列腺癌靶向治疗
在过去二十多年中,针对肿瘤特定分子特征的靶向治疗已成为癌症治疗的重要突破。然而,前列腺癌领域在这方面长期进展有限。直到一类基因突变——DNA损伤修复(DDR)基因异常,出现在研发人员的视野中。
在乳腺癌和卵巢癌中,基于“合成致死”原理开发的PARP抑制剂,已被证明对BRCA1/2突变及其他DDR异常有效。研究显示,在晚期前列腺癌患者中,高达11.8%存在DDR种系变异;而在转移性去势抵抗性前列腺癌患者中,约23%携带ATM、CHEK2、BRCA1、BRCA2等DDR基因突变。
这些数据提示,PARP抑制剂或许也能对部分前列腺癌患者产生疗效。
临床研究证实了这一设想。2020年,Lynparza以及Rubraca(rucaparib,芦卡帕利)获得FDA批准,用于治疗携带特定DDR异常的转移性去势抵抗性前列腺癌。2023年,另外两种PARP抑制剂——Talzenna(talazoparib,他拉唑帕利)和Zejula(niraparib,尼拉帕尼)也进入了前列腺癌的治疗领域。
自此,前列腺癌靶向治疗领域不再是一片荒漠。
“不限癌种”免疫疗法造福患者
免疫治疗是近年来深刻改变癌症治疗格局的重要突破之一。早在2010年,前列腺癌领域就迎来了首个免疫疗法——癌症疫苗Provenge(sipuleucel-T)。尽管前列腺癌比许多实体瘤更早拥有免疫治疗选择,但遗憾的是,以PD-1单抗为代表的免疫检查点抑制剂对大多数前列腺癌患者效果有限。然而,对于少数特定分子特征的患者,情况则有所不同。
2017年,FDA划时代地批准了Keytruda(pembrolizumab,帕博利珠单抗)用于治疗微卫星不稳定性高或错配修复缺陷(MSI-H/dMMR)的癌症,不限癌种。自此,具备MSI-H/dMMR特征的前列腺癌患者也拥有了新的治疗希望。此后,更多抗PD-1/PD-L1抗体药物,如Jemperli(dostarlimab)、百泽安(tislelizumab,替雷利珠单抗)、恩维达(envafolimab,恩沃利单抗)、普佑恒(pucotenlimab,普特利单抗)等,也相继获批用于MSI-H/dMMR实体瘤的治疗。
虽然MSI-H/dMMR在前列腺癌中较为罕见,但对这部分少数患者而言,免疫治疗无疑带来了全新的生机。
“定点靶向”放疗提供新选择
尽管拥有了更多治疗选择,但转移性去势抵抗性前列腺癌目前仍无法治愈。对于那些历经多种治疗后病情仍持续进展的患者,开发新疗法显得尤为迫切。
科学家将目光聚焦于前列腺特异性膜抗原(PSMA)。作为一种在前列腺癌细胞表面高表达的跨膜酶,PSMA在大多数转移性去势抵抗性前列腺癌患者的转移灶中也广泛存在,因而成为理想的靶向治疗目标。
有了明确的靶点,接下来需要寻找能精准杀伤癌细胞的“箭头”。研究人员此次将希望寄托于放疗。2006年,美国普渡大学的科学家设计出一种高亲和力的PSMA配体,并提出将其与放射性药物连接。2012年,德国研究人员进一步优化了该配体的亲和力,推动了一种全新药物的成型——即结合放射性同位素镥-177的高亲和力PSMA配体。
经过多年临床研究,前列腺癌治疗在2022年迎来又一次变革:FDA批准了首个用于治疗转移性去势抵抗性前列腺癌的放射性配体药物Pluvicto(lutetium Lu 177 vipivotide tetraxetan,镥[177Lu]-特昔维匹肽)。Pluvicto的获批是放射性配体疗法领域的重大突破,也为那些已用尽传统治疗手段的晚期前列腺癌患者带来了新的希望。
更多新药研发已在路上
尽管各类创新疗法接连出现,极大丰富了前列腺癌患者的治疗选择。但由于发病率高,这类癌症每年仍造成大量死亡。患者仍然需要更优的治疗方案。
令人期待的是,众多创新机制的疗法已在路上。例如前文提到的基于“合成致死”机制的靶向疗法,目前研发管线中约有40款新药,靶点涵盖PARP、EZH2、ATR、PLK1、POLQ、USP1、PRMT5等。此外全球也有40余款放射性配体疗法正在临床阶段探索治疗前列腺癌的潜力,靶点主要为PSMA,还包括SSTR2、GRPR、DLL3、NTSR1、KLK2等。靶向配体形式涵盖小分子、抗体与多肽,所用放射性同位素包括Lu 177、Ac 225、Ga 68、In 111等。
靶向蛋白降解药物(TPD)通过直接降解雄激素受体蛋白,可更深度、持久地抑制该信号通路,有望克服传统雄激素受体拮抗剂耐药性,成为一股新生力量。例如,Arvinas公司开发的第二代雄激素受体靶向蛋白降解嵌合体(PROTAC®)ARV-766,在早期临床试验中已表现出能够选择性降解野生型和带有临床耐药相关突变的雄激素受体的能力。公开资料显示,目前已有10多款TPD疗法进入临床阶段,用于治疗前列腺癌。
在助力各类疗法从创新概念走向临床验证的过程中,药明康德致力于支持全球客户加速研发进程,凭借CRDMO平台能够“端到端”助力各类分子从发现、到开发,再到生产交付的全过程。以放射性配体药物为例,药明康德综合性的放射性药物发现平台整合了多肽发现和放射性药物开发能力,提供包括多肽合成、螯合剂合成、放射性标记、成像、药理学研究和监管申报支持等完善的服务。一体化平台能够让多个团队并行攻坚、高度协作,帮助合作伙伴快速推动项目进展,节省宝贵的开发时间。在TPD药物开发方面,药明康德已经助力70多种TPD分子进入临床前候选药物(PCC)阶段,10多种已进入后期开发阶段。
展望下一个25年,我们期待与产业同道继续并肩前行,突破更多疾病领域的治疗瓶颈,将更多创新疗法更快带到患者身边。
免责声明:本文仅作信息交流之目的,文中观点不代表药明康德立场,亦不代表药明康德支持或反对文中观点。本文也不是治疗方案推荐。如需获得治疗方案指导,请前往正规医院就诊。
版权说明:欢迎个人转发至朋友圈,谢绝媒体或机构未经授权以任何形式转载至其他平台。转载授权请在「医药观澜」微信公众号回复“转载”,获取转载须知。
2025-11-25
·药明康德
编者按:2025年,药明康德迎来创立25周年的重要里程碑。值此契机,我们向所有与我们共同书写产业变革篇章的科学家、医药人和投资者致以衷心感谢与诚挚敬意,也特别推出“致敬时代”系列,回顾全球同仁如何借助科学与合作的力量,不断拓展治疗边界、改善患者命运。
四分之一个世纪的坚守,只为加速每一款新药的诞生。下一个25年,我们将继续心怀感恩与敬畏,依托独特的CRDMO模式,与全球伙伴携手同行,共赴健康未来。
1853年,伦敦医院,一名53岁的男子在与病魔抗争了3年后去世,外科医生John Adams为了搞清楚病因,做了尸检,发现凶手隐藏在患者的前列腺中。Adams在病理报告里写道,患者的前列腺发生了硬化,他进一步评论,这是一种很罕见的疾病。
这是医学史上第一例通过病理检验确诊的前列腺癌。但Adams恐怕不会想到150多年后,自己发现的这种疾病将会成为男性中最常见的癌症之一。2020年,前列腺癌在112个国家中位列男性癌症发病率首位,每年新增病例约140万,占男性癌症的15%,造成约40万人死亡。
前列腺癌发病率确实出现了大幅增加,而且这种上升趋势很可能还会继续,研究预计到2040年,全球每年新增前列腺癌将达290万。
为什么前列腺癌越来越多?背后有多个因素。首先是诊断手段的进步。直到20世纪初,前列腺癌才与其他类型的尿路梗阻区分开来,而如今,通过前列腺特异性抗原(PSA)筛查,临床上可以发现非常早期的前列腺癌。
其次是老龄化趋势。前列腺癌的发病率与年龄密切相关,而且这种随年龄增长的增速几乎超过所有癌症。
其三则与生活方式有关。流行病学研究显示亚洲男性的前列腺癌发病率低于西方,但移居欧美的亚裔男性风险显著上升,提示饮食或环境因素可能影响前列腺癌的发病率。
不过,值得欣慰的是,过去几十年里,前列腺癌的诊疗突飞猛进。对很多患者来说,前列腺癌的确诊报告早已不再是一份宣告生命即将结束的“判决书”。
图片来源:123RF
作为全球医药及生命科学行业值得信赖的合作伙伴和重要贡献者,药明康德在过去25年发展历程中,很荣幸见证了多款前列腺癌创新疗法从实验室到临床的突破历程,更通过提供一体化、端到端的新药研发和生产服务,助力全球合作伙伴加速多款前列腺癌创新疗法的研发进程、造福病患。今天这篇文章将回望前列腺癌创新疗法的发展历程,向那些拯救无数患者的英雄们致敬。
诺奖级发现打破治疗僵局
医学界很早就对前列腺癌发起了挑战,1904年,泌尿科先驱,后来创办了《泌尿外科杂志》(The Journal of Urology)的Hugh Hampton Young博士做了全球首例前列腺根治性切除术。1909年,Young博士报告了19例手术预后,15位患者症状几乎完全缓解,有1位患者术后存活超过5年,可能已被治愈。前列腺根治性切除至今仍是早期前列腺癌的关键治疗手段。
同一时期,居里夫妇发现了镭、钋这两个放射性元素后掀起的放疗研究热进入前列腺癌治疗。法国泌尿科医生Henri Minet尝试用含镭的导管经尿道或耻骨上导管治疗前列腺癌,近距离放疗成了最早用于前列腺治疗的放疗手段。
然而,这些早期突破后,前列腺癌的治疗很快陷入僵局。受限于早期放疗技术缺陷,操作过程对患者来说极痛,难以在前列腺癌中推广。而手术对于已经出现癌细胞转移的晚期前列腺癌患者也意义有限。
20世纪中期,泌尿科医生面对的典型前列腺癌患者会是一位70岁刚出头的老人,癌细胞已经转移到骨骼或软组织。这在当时几乎等于被判了死刑,患者通常在1-2年里就会被癌症夺去生命。
但前列腺癌治疗的革命性突破即将在一所建立不久的医学院里诞生。1927年,刚做完普外科住院医师培训,年仅26岁加拿大裔美国医生Charles Brenton Huggins被招募到刚成立的芝加哥大学医学院,作为整个医学院最初的8名员工之一,Huggins博士被分配到了泌尿科,被迫迅速自学专科知识。
整个30年代,他不断深入研究包括前列腺在内的男性泌尿系统器官。厚积薄发,1940-41年,Huggins博士与他的两名学生连续发表了3篇论文,阐述通过睾丸切除术或雌激素治疗来抑制雄激素活性,可以让许多转移性前列腺癌患者的肿瘤缩小。那些接受治疗的患者短短几天内疼痛就得到了显著缓解,最初接受治疗的21人中,有4人存活超过12年!
Huggins博士的发现开启了前列腺癌治疗的全新时代:去势治疗。由于超过80%的前列腺癌对雄激素存在依赖,去势治疗可以缓解绝大部分患者的病痛。Huggins也因此获得1966年诺贝尔生理学或医学奖。值得一提的是,他提出的口服雌激素药物去势疗法还是第一个有效的全身性癌症治疗方法,是晚期肿瘤治疗的划时代突破。而对于广大前列腺患者,时至今日,Huggins博士开启的去势疗法仍然是最普遍有效的治疗方法。
▲Charles Brenton Huggins博士(图片来源:Nobel Foundation archive)
从LHRH激动剂到拮抗剂
尽管口服雌激素与睾丸切除术开启了前列腺癌治疗的全新时代,但很快这些去势手段的局限性就显现了出来,首先是口服雌激素降低血清睾酮水平会导致显著的心血管毒性,增加血栓风险。其次,通过去势或雌激素治疗来消除雄激素,也不足以治愈晚期前列腺癌。
显然,需要寻找更好的去势治疗手段,而这需要另一个诺奖级别的突破。
1971年,美国科学家Andrew Schally用了16万头猪的下丘脑,分离出800微克的一种名为促黄体生成素释放激素(LHRH)的下丘脑激素。这种激素能刺激脑垂体释放黄体生成素(LH),后者又能与睾丸上的受体结合,激活雄激素睾酮合成。
有趣的是,Schally博士发现尽管LHRH激动剂会导致血清睾酮短暂升高,但长期使用会产生抑制作用,下调垂体LHRH受体,降低血清睾酮,与去势手术相当。于是,他尝试将LHRH激动剂用于前列腺癌患者治疗,发现可以显著缓解癌症相关的骨痛。
▲Andrew Schally博士(图片来源:Nobel Foundation archive)
1977年,Schally博士获得了诺贝尔生理学或医学奖。1985年,FDA批准了第一个用于治疗晚期前列腺癌的LHRH激动剂Lupron(leuprolide,亮丙瑞林),之后,Zoladex(goserelin,戈舍瑞林)、Trelstar(triptorelin acetate,醋酸曲普瑞林)相继上市。70-80%的前列腺癌患者使用这些LHRH激动剂后,肿瘤能被有效抑制,同时,这些药物没有口服激素带来的心血管、血栓风险,至今仍是优先使用的去势治疗手段。
可是,LHRH激动剂也有缺点,如同Schally博士当初观察到的,这类药物刚开始使用时会先增加体内睾酮合成,导致有些前列腺癌患者将经历癌症恶化。于是,业界开始寻找LHRH拮抗剂。
2008年,Firmagon(degarelix,地加瑞克),这种皮下注射的LHRH拮抗剂获批上市,让患者能更快降低血清睾酮,避免了去势治疗初始阶段因睾酮短暂升高而出现癌症恶化的风险。2020年,全球首个口服LHRH拮抗剂Orgovyx(relugolix,瑞卢戈利)获批,又为患者提供了一种更便捷的治疗选择。
突破重重困难的抗雄激素
就在Schally研究LHRH的同一时期,60年代末,科学家发现了雄激素受体,这无疑带来了新的潜在去势疗法研发方向。无论是LHRH激动剂还是拮抗剂,都存在影响性功能、导致潮热等副作用,靶向雄激素受体的抗雄激素(雄激素受体拮抗剂)或许能避免这些副作用。很快科学家们找到了一个甾体类抗雄激素,cyproterone(环丙孕酮)。
科学家们对这第一个抗雄激素充满期望,但挫折很快到来:环丙孕酮能透过血脑屏障,它不仅和前列腺癌细胞上的雄激素受体结合,还与下丘脑和垂体上的雄激素受体结合,阻断雄激素合成的负反馈。这导致环丙孕酮治疗的最终结局是增加血清睾酮,没法起到去势作用。
研究人员想了个对策:添加乙酸酯基团,合成Androcur(cyproterone acetate,醋酸环丙孕酮)。醋酸环丙孕酮保留了雄激素拮抗作用,作用于前列腺癌细胞;同时它也是一种孕激素激动剂,能与垂体中的孕激素受体结合,间接降低血清睾酮水平。这种双机制治疗的有效性与口服雌激素大致相当,1973年在欧洲获批上市。
可是,人们发现醋酸环丙孕酮还是有局限性:它对雄激素分泌的影响会导致性欲减退和性功能障碍。业界开始寻找非甾体类的抗雄激素,以避免这些副作用。
图片来源:123RF
Eulexin(flutamide,氟他胺)成为第一个进入临床试验的非甾体类抗雄激素,并于1989年获得FDA批准用于前列腺癌治疗。它和90年代获得FDA批准的Casodex(bicalutamide,比卡鲁胺)、Nilandron(nilutamide,尼鲁米特)组成了第一代抗雄激素,或第一代雄激素受体拮抗剂。
尽管第一代抗雄激素如研究人员期望的,副作用更小,可是后续研究发现它们和环丙孕酮一样,最终还是会穿过血脑屏障,增加LH释放,进而导致血清睾酮升高。在转移性前列腺癌患者的随机试验中,研究人员发现单独使用第一代抗雄激素治疗,与其它药物或去势手术去势相比,尽管耐受性更好,但在总生存期和无进展生存期上,并无优势。
虽有缺陷,但随着第一代抗雄激素的出现,那些LHRH激动剂或拮抗剂治疗无效的患者,可以加入抗雄激素,或者在一开始治疗时就采用LHRH激动剂加抗雄激素的联合雄激素阻断,都能获得更好的治疗效果。
两代抗雄激素改写去势抵抗性前列腺癌治疗格局
不过,即便有了LHRH激动剂、拮抗剂以及第一代抗雄激素,大部分前列腺癌患者治疗后仅能获得几年的缓解,之后肿瘤就会出现耐药,发展成去势抵抗性前列腺癌,最终成为夺走患者生命的主要原因。很长一段时间里,去势抵抗性前列腺癌患者只能依赖多西他赛、卡巴他赛这些化疗,疗效也不理想。面对困难,医药界人士并未低头,研究发现去势抵抗性前列腺癌细胞大多是出现了雄激素受体扩增、点突变、剪接变体表达。不是抑制雄激素信号通路不行,而是第一代抗雄激素抑制不了这些改变了的雄激素信号通路,甚至,第一代抗雄激素在长期使用后能从拮抗剂转为激动剂的缺点还将帮倒忙。
患者需要的是新一代抗雄激素。
而在2010年后,前列腺癌治疗迎来了一个新药井喷期:多个第二代抗雄激素陆续上市,彻底改变了去势抵抗性前列腺癌的治疗格局。
图片来源:123RF
首先打破僵局的是2011年获得FDA批准的Zytiga(abiraterone,阿比特龙),它是一种很特殊的抗雄激素,并不直接作用于雄激素受体,而是抑制雄激素合成。在转移性去势抵抗性前列腺癌的临床试验里,阿比特龙将患者的总生存时间从安慰剂组的10.4个月提升到了15.4个月。
阿比特龙只是一个开始,紧接着2012年,Xtandi(enzalutamide,恩扎卢胺)获得FDA批准,这是一类全新的雄激素受体拮抗剂,不像第一代抗雄激素那样会出现拮抗剂到激动剂的转变。在对化疗耐药的去势抵抗性前列腺癌患者中,临床试验显示恩扎卢胺治疗的总生存期达18.3个月,比安慰剂组的13.6个月有大幅提高。
不过,研究人员发现高剂量恩扎卢胺存在癫痫风险,这又成了后续第二代抗雄激素研发的指引。2018年,Erleada(apalutamide,阿帕他胺)获得FDA批准,它更少透过血脑屏障,缓解了癫痫风险。
2019年,Nubeqa(darolutamide,达罗他胺)成为最新一个获得FDA批准的二代抗雄激素。达罗他胺对所有已知的雄激素受体突变都能维持抑制作用,即便是能导致恩扎卢胺、阿帕他胺耐药的突变也不例外,使它成了应对耐药问题的利器。
2022年与2025年,中国国家药品监督管理局分别批准艾瑞恩(rezvilutamide,瑞维鲁胺)与海纳安(enzalutamide deuterated,氘恩扎鲁胺)上市,这些二代抗雄激素又为患者带来更多选择。
精准治疗进入前列腺癌
针对肿瘤特定分子特征的精准治疗是过去20多年癌症治疗的巨大突破,但很长一段时间里,前列腺癌的精准治疗一直处于空白状态。
前列腺癌就没有精准治疗可以打击的分子特征吗?
一类基因突变引发了业界注意——DNA损伤修复(DDR)基因异常。在乳腺癌、卵巢癌中,基于“合成致死”机制开发的PARP抑制剂是针对BRCA1/2突变或其他DDR异常的有效治疗手段。而研究显示,高达11.8%的晚期前列腺癌患者存在DDR种系变异,约23%的转移性去势抵抗性前列腺癌存在ATM、CHEK2、BRCA1、BRCA2等DDR基因突变。
PARP抑制剂或许对部分前列腺癌患者也能有效!
临床研究证实了这一点。一项在转移性去势抵抗性前列腺癌患者中展开的3期临床试验显示,对于具有BRCA1、BRCA2或ATM中任意一类突变的患者,使用Lynparza(olaparib,奥拉帕利)治疗,患者无进展生存期为7.4个月,远高于使用二代抗雄激素的对照组(3.6个月)。奥拉帕利降低患者癌症进展或死亡的风险达66%。
2020年,奥拉帕利以及Rubraca(rucaparib,芦卡帕利)获得FDA批准用于具有特定DDR异常的转移性去势抵抗性前列腺癌。2023年,另外两个PARP抑制剂Talzenna(talazoparib,他拉唑帕利)和Zejula(niraparib,尼拉帕尼)也进入前列腺癌治疗。
前列腺癌不再是精准治疗的荒漠。
两代免疫治疗造福患者
免疫治疗是另一项近年来深刻改变癌症治疗格局的重大突破。而早在2010年,前列腺癌患者就迎来了第一个免疫治疗:Provenge(sipuleucel-T)。它其实是一种癌症疫苗。从患者血液里分离出来的白细胞会在实验室里和前列腺癌细胞的一种蛋白质,前列腺酸性磷酸酶(PAP)混合,然后这些接受了抗原刺激的白细胞被回输到患者体内,增加对前列腺癌细胞的杀伤。
3期临床试验中,接受sipuleucel-T治疗的转移性去势抵抗性前列腺癌患者的中位生存期为25.9个月,优于安慰剂治疗的21.4个月中位生存期。而与sipuleucel-T类似的另一种自体免疫治疗Apceden也于2017年在印度获批上市。
尽管比很多实体瘤都更早收获免疫治疗,但令人遗憾的是对于大部分前列腺癌患者,以PD-1单抗为代表的肿瘤免疫治疗并不适用。可对少数幸运的患者,情况不同。
2017年,FDA划时代地批准了Keytruda(pembrolizumab,帕博利珠单抗)用于治疗微卫星不稳定性高或错配修复缺陷(MSI-H/dMMR)的癌症,不限癌种。该批准的基础是临床研究发现无论癌症起源于哪个器官,只要具有MSI-H/dMMR这一分子特征,就能从帕博利珠单抗治疗中获益。
从此,具有该分子特征的前列腺癌患者也有了新的治疗选择。此后,更多PD-1/PD-L1抗体,如Jemperli(dostarlimab)、百泽安(tislelizumab,替雷利珠单抗)、恩维达(envafolimab,恩沃利单抗)、普佑恒(pucotenlimab,普特利单抗),也都获批用于MSI-H/dMMR实体瘤治疗。
MSI-H/dMMR在前列腺癌中比较罕见,可对于那少数患者,免疫治疗带来了新的希望。
前列腺癌治疗迎来“定点靶向”放疗
虽然过去20年,去势治疗、精准治疗以及免疫治疗的发展让晚期前列腺癌患者有了很多治疗选择,但转移性去势抵抗性前列腺癌尚无法治愈,这使得那些接受多种治疗后出现疾病进展的患者,亟需新的疗法。
科学家将目光投向了前列腺特异性膜抗原(PSMA),一种在前列腺癌细胞上高表达的跨膜酶,而且大多数转移性去势抵抗性前列腺癌患者的转移灶也表达PSMA,使它成了靶向前列腺癌的优良选择。
箭有了,可配什么箭头能最大程度杀伤癌细胞呢?
这次,研究人员想到了放疗。2006年,美国普渡大学的科学家设计了一种高亲和力的PSMA配体,并提出给该配体连接放射性药物的设计。2012年,德国的研究人员又进一步改善了这种配体的亲和力。
一种全新的药物,结合放射性同位素镥177的PSMA高亲和力配体,逐渐成型。
经过多年临床研究,2022年,前列腺癌治疗迎来了又一变革:FDA批准了第一个用于治疗转移性去势抵抗性前列腺癌的放射性配体药物:Pluvicto(lutetium Lu 177 vipivotide tetraxetan,镥[177Lu]-特昔维匹肽)。
在相关的3期临床研究中,晚期PSMA阳性转移性去势抵抗性前列腺癌患者被随机分配至镥[177Lu]-特昔维匹肽联合标准治疗组或标准治疗组。结果显示,联合治疗组总生存期达15.3个月,显著高于标准治疗组的11.3个月。联合治疗降低死亡风险达38%。而且,联合治疗组中患者的总缓解率达到30%,而只接受标准治疗患者的缓解率仅为2%。
镥[177Lu]-特昔维匹肽的出现是放射性配体药物的重大突破,也为那些穷尽过往治疗手段的晚期前列腺癌患者带来了新的选择。
更多新药研发已在路上
前列腺癌作为男性中发病率最高的癌症之一,曾经夺去无数人的生命。1960年代,即便在欧美发达国家,50-60%的前列腺癌确诊患者生存时间不超过5年。但是,随着去势治疗的不断发展,以及精准治疗、免疫治疗乃至放射性配体药物的出现,仅在过去25年间,全球监管机构便批准了至少20款创新疗法,为无数前列腺癌患者带来了新生,如今90%以上的前列腺癌患者可以实现长期生存。
然而,由于发病率高,前列腺癌尤其是尚无法治愈的转移性去势抵抗性前列腺癌,每年仍造成大量死亡。患者仍然需要疗效更优的治疗方案。好消息是,众多创新机制的疗法已在路上。例如前文提到的基于“合成致死”机制的靶向疗法,目前研发管线中约有40款新药,靶点涵盖PARP、EZH2、ATR、PLK1、POLQ、USP1、PRMT5等。而放射性配体药物方面,全球也有40余款创新药正在临床阶段探索治疗前列腺癌的潜力,靶点主要为PSMA,还包括SSTR2、GRPR、DLL3、NTSR1、KLK2等。靶向配体形式涵盖小分子、抗体与多肽,所用放射性同位素包括Lu 177、Ac 225、Ga 68、In 111等。
此外,靶向蛋白降解药物(TPD)有望成为克服传统雄激素受体拮抗剂耐药性的新生力量。它们通过直接降解雄激素受体蛋白,可更深度、持久地抑制该信号通路。例如,Arvinas公司开发的第二代雄激素受体靶向蛋白降解嵌合体(PROTAC®)ARV-766,在早期临床试验中已表现出能够选择性降解野生型和带有临床耐药相关突变的雄激素受体的能力。公开资料显示,目前已有10多款TPD疗法进入临床阶段,用于治疗前列腺癌。
在助力各类疗法从创新概念走向临床验证的过程中,药明康德致力于支持全球客户加速研发进程,凭借CRDMO平台能够“端到端”助力各类分子从发现、到开发,再到生产交付的全过程。以放射性配体药物为例,药明康德综合性的放射性药物发现平台整合了多肽发现和放射性药物开发能力,提供包括多肽合成、螯合剂合成、放射性标记、成像、药理学研究和监管申报支持等完善的服务。一体化平台能够让多个团队并行攻坚、高度协作,帮助合作伙伴快速推动项目进展,节省宝贵的开发时间。在TPD药物开发方面,药明康德已经助力70多种TPD分子进入临床前候选药物(PCC)阶段,10多种已进入后期开发阶段。
展望下一个25年,我们期待与产业同道继续并肩前行,突破更多疾病领域的治疗瓶颈,将更多创新疗法更快带到患者身边。
参考资料:
[1] Denmeade, S., Isaacs, J. A history of prostate cancer treatment. Nat Rev Cancer 2, 389–396 (2002). https://doi.org/10.1038/nrc801
[2] Lehtonen M, Kellokumpu-Lehtinen P-L. The past and present of prostate cancer and its treatment and diagnostics: A historical review. Sage Open Medicine. 2023;11. doi:10.1177/20503121231216837
[3] Mallah H, Diabasana Z, Soultani S, Idoux-Gillet Y, Massfelder T. Prostate Cancer: A Journey Through Its History and Recent Developments. Cancers. 2025; 17(2):194. https://doi.org/10.3390/cancers17020194
[4] James, Nicholas D et al. The Lancet Commission on prostate cancer: planning for the surge in cases. The Lancet, Volume 403, Issue 10437, 1683 - 1722
[5] Rice MA, Malhotra SV, Stoyanova T. Second-Generation Antiandrogens: From Discovery to Standard of Care in Castration Resistant Prostate Cancer. Front Oncol. 2019 Aug 28;9:801. doi: 10.3389/fonc.2019.00801.
[6] De Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102.
[7] Keam, S.J. Lutetium Lu 177 Vipivotide Tetraxetan: First Approval. Mol Diagn Ther 26, 467–475 (2022). https://doi.org/10.1007/s40291-022-00594-2
免责声明:本文仅作信息交流之目的,文中观点不代表药明康德立场,亦不代表药明康德支持或反对文中观点。本文也不是治疗方案推荐。如需获得治疗方案指导,请前往正规医院就诊。版权说明:欢迎个人转发至朋友圈,谢绝媒体或机构未经授权以任何形式转载至其他平台。转载授权请在「药明康德」微信公众号回复“转载”,获取转载须知。
分享,点赞,在看,聚焦全球生物医药健康创新
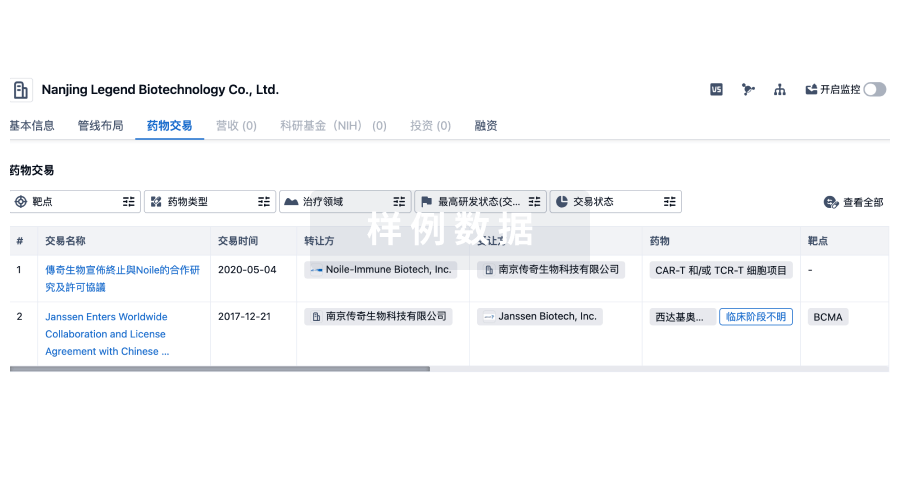
100 项与 Pritzker School of Medicine 相关的药物交易
登录后查看更多信息
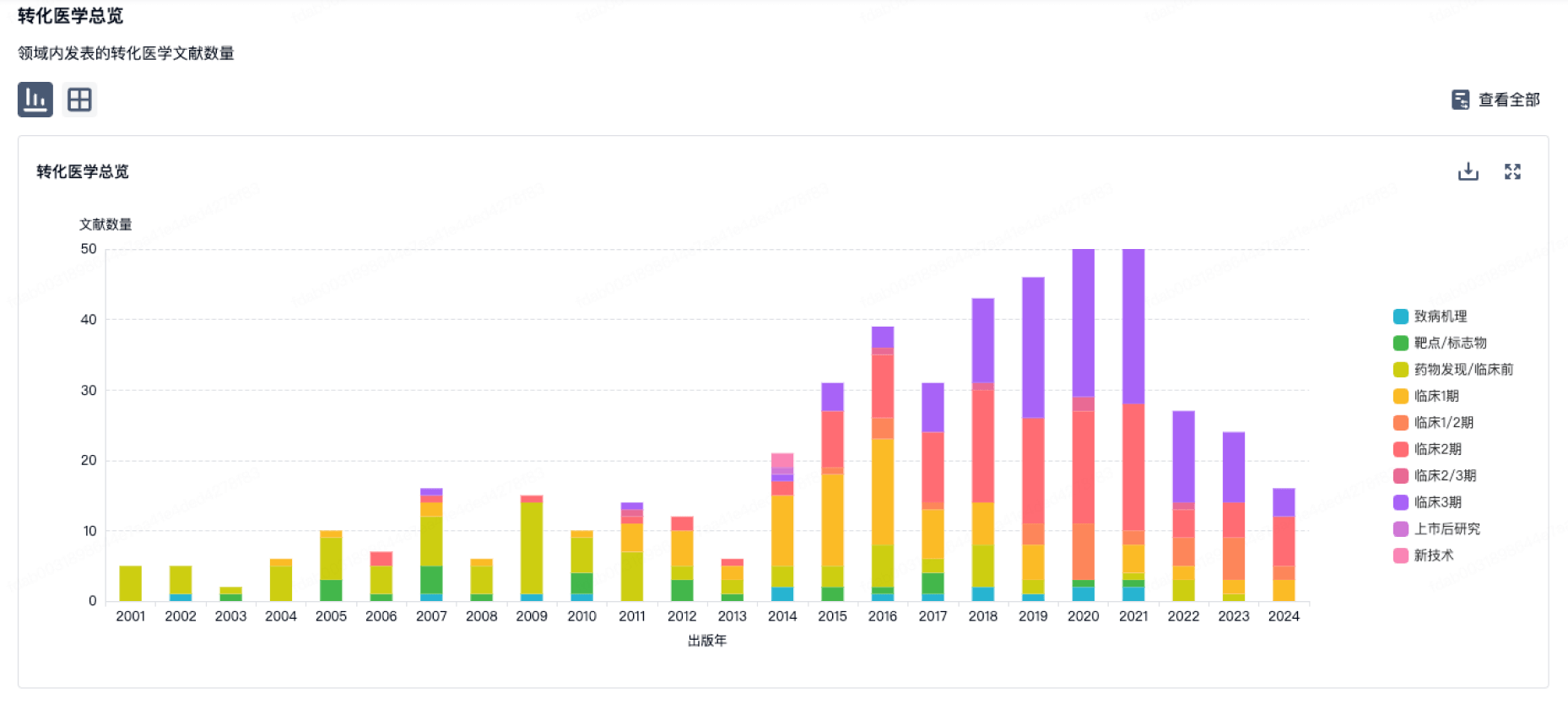
100 项与 Pritzker School of Medicine 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月04日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
其他
1
登录后查看更多信息
当前项目
| 药物(靶点) | 适应症 | 全球最高研发状态 |
|---|---|---|
SND-121 ( mGluRs ) | 神经痛 更多 | 无进展 |
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
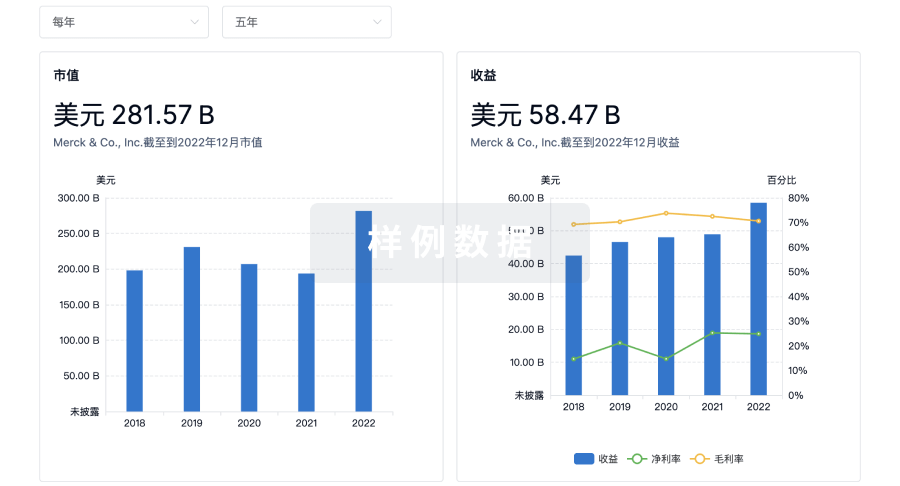
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用