预约演示
更新于:2026-06-14
Prospect Medical Holdings, Inc.
更新于:2026-06-14
概览
关联
NCT04467983
Abaloparatide Added to Ongoing Denosumab vs Continued Denosumab Alone

NCT04517682
SARS -CoV-2 Detection in Saliva Samples: A Test Validation Protocol

NCT03734471
Use of a Novel Chest Tube Insertion Device for Urgent Thoracostomy in an Emergency Department Setting
100 项与 Prospect Medical Holdings, Inc. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-12-01MAYO CLINIC PROCEEDINGS
Impact of Lipid-Lowering Combination Therapy With Statins and Ezetimibe vs Statin Monotherapy on the Reduction of Cardiovascular Outcomes: A Meta-analysis
Article
作者: Ang, Song Peng ; Reiner, Zeljko ; Banach, Maciej ; Toth, Peter P ; Gaita, Dan ; Sawhney, Aanchal ; Amarenco, Pierre ; Jaiswal, Vikash ; Lavie, Carl J ; Pećin, Ivan ; Deb, Novonil ; Penson, Peter E
OBJECTIVE:
To evaluate the efficacy of combination lipid-lowering therapy (LLT) compared with statin monotherapy for low-density lipoprotein cholesterol (LDL-C) reduction, associated adverse events, and outcomes.
METHODS:
A systematic literature search was conducted using PubMed, Embase, and ClinicalTrials.gov to identify relevant articles published from inception until the end of June 2024. The outcomes were assessed using pooled odds ratios (ORs) for categorical data and mean difference for continuous data, with corresponding 95% CIs.
RESULTS:
A total of 14 studies (11 randomized controlled trials and 3 cohort studies) with 108,373 very high-risk patients were included in the final analysis. The mean age of the patients in the combination LLT group and the statin monotherapy group was 67.31 and 67.89 years, respectively. Pooled analysis revealed that combination LLT significantly more effectively reduced the LDL-C level from baseline (mean difference, -12.96 mg/dL; 95% CI, -17.27 to -8.65; P<.001) and significantly reduced all-cause mortality (OR, 0.81; 95% CI, 0.67 to 0.97; P=.02), major adverse cardiovascular events (OR, 0.82; 95% CI, 0.69 to 0.97; P=.02), and stroke incidence (OR, 0.83; 95% CI, 0.75 to 0.91; P<.001), with an insignificant effect on cardiovascular mortality (OR, 0.86; 95% CI, 0.65 to 1.12; P=.26) when compared with statin monotherapy. The risk of adverse events and the therapy discontinuation rate were comparable between groups.
CONCLUSION:
Combination LLT was associated with an overall greater reduction in LDL-C, the same risk of adverse effects, and significantly lower risk of all-cause mortality, major adverse cardiovascular events, and stroke compared with statin monotherapy. Forthcoming guidelines should consider the lipid-lowering combination therapy as early as possible, preferably up-front, for more effective LDL-C goal achievement and significant reduction of cardiovascular disease outcomes and mortality in high- and very high-risk patients.
2025-10-01ANNALS OF SURGERY
Moderate- to High-grade Blunt Liver and Spleen Injuries Warrant Repeat Imaging to Identify Treatable Complications
Article
作者: Thompson, Brevin ; Teichman, Amanda L. ; Bernard, Andrew ; Scantling, Dane ; Mulita, Francesk ; Thurston, Brian ; Gadomski, Stephen ; Carlson, Amanda ; Collom, Morgan ; Craft, Patrick ; Hancin, Emily ; Zorn, Julia ; Almahmoud, Khalid ; Udekwu, Pascal ; Noorbakhsh, Matthew ; Fraser, Douglas ; Frederick, Nicole ; Briggs, Steven ; McNickle, Allison G. ; Bresz, Kellie ; Kirsch, Jordan ; Alvarez, Claudia ; Laudon, Aksel ; Bhattacharya, Bishwajit ; Berne, John D. ; Narveson, Joel ; Nemeth, Zoltan H. ; Goldenberg, Anna ; Lawrence, Jeffrey ; Smith, Alison A. ; Guido, Jenny ; Meizoso, Jonathan P. ; Okorafor, Oluwadara ; O’Neil, Christopher F. ; Morgan, Madison E. ; Bailey, Carolyn ; Grant, Jennifer ; Davis, Greggory ; Lapham, David ; Lewis, Richard ; Ratnasekera, Asanthi ; Jackovich, Alexandra ; Haan, James M. ; Horst, Michael ; Maung, Adrian A. ; Holliday, Tyler ; Streams, Jill ; Oh, John ; Bilaniuk, Jaroslaw W. ; Sais, Erica ; Kundi, Rishi ; Butts, Christopher A. ; Williams, Jamie ; Evans, David ; Collins, Michael ; Glass, Nina ; Wang, Ethan ; Cullinane, Daniel ; Brigode, William ; Michetti, Christopher P. ; Bankhead, Brittany ; Rosenthal, Martin ; Mederos, Dalier Rodriguez ; Jacobson, Lewis A. ; Mehta, Charmi ; Chowdhury, Sharfuddin ; Ewing, Kaily ; Leoni, Jack A. ; Mousafeiris, Vasileios ; Lightwine, Kelly ; Shell, Chloe ; Doris, Stephanie ; Ahmeti, Mentor ; Broderick, Meaghan ; Falank, Carolyne ; Fletcher, Kelsey L. ; Hazelton, Joshua P. ; Bjordahl, Paul ; Nahmias, Jeffry ; Lieser, Mark ; Turcotte, Morgan ; Perea, Lindsey L. ; Dixon, Alexandra ; Marshall, Gary ; Muse, Thomas ; Stecher, Johanna S. ; Choron, Rachel L.
Objective::
The aim of this study was to assess whether blunt liver (BLI) and blunt spleen (BSI) injury patients benefit from repeat imaging to identify injury-related complications.
Background::
No consensus guidelines exist regarding the necessity of, or optimal timing for, repeat imaging in BLI and BSI patients undergoing nonoperative management (NOM). We hypothesize that scheduled repeat imaging of patients undergoing NOM for moderate- to high-grade BLI and BSI would result in identification of complications earlier than if repeat imaging is performed in response to a change in clinical condition.
Methods::
We performed a 4-year, 43-center, multinational, prospective observational study of adult patients undergoing initial NOM of BLI and/or BSI. Patients were grouped by reason for repeat imaging: scheduled imaging (SI) or imaging performed for clinical change (CC), and by whether findings on repeat imaging resulted in procedural or operative intervention.
Results::
We identified 2341 BLI and 2143 BSI patients (528 concomitant BLI/BSI). Repeat imaging was performed in 822 (35.1%) BLI patients [SI: 457 (55.5%), CC: 365 (44.5%)] and 758 (27.9%) BSI patients [SI: 478 (63.1%), CC: 280 (37.0%)]. Complications were identified on repeat imaging in BLI: 167 (7.1%) [SI: 72 (43.1%), CC: 95 (56.9%)] and BSI: 203 (7.5%) [SI: 91 (44.8%), CC: 112 (55.2%)]. Of patients with BLI complications, 96 (57.8%) [SI: 37 (38.5%), CC: 59 (61.5%)] underwent an intervention. Of patients with BSI complications, 133 (65.5%) [SI: 56 (42.1%), CC: 77 (57.9%)] underwent an intervention. Our data demonstrate that in BLI and BSI, most complications were identified within 48 to 72 hours.
Conclusions::
Scheduled repeat imaging for asymptomatic patients with BLI grade 4 to 5 and BSI grade 3 to 5 within 48 to 72 hours from time of diagnosis allows for identification of complications before a change in the patient’s clinical condition.
2025-10-01MOLECULAR IMAGING AND BIOLOGY
Advances in the Molecular Imaging of Sarcoma: An Emphasis on Metabolic Imaging
Review
作者: Naseer, Rizwan ; Lau, Hui Chong ; Mirbod, Melika ; Jonnakuti, Sriya ; Ayubcha, Cyrus ; Ng, Sze Jia ; Jia, Lori
PURPOSE:
Sarcomas, malignancies of mesenchymal origin, present significant diagnostic and therapeutic challenges due to their heterogeneity and low incidence. This review aims to examine the evolving role of fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) in the management of soft tissue and musculoskeletal sarcomas. Specifically, it seeks to evaluate 18F-FDG PET/CT's utility in detecting metastatic lesions, differentiating benign from malignant tumors, and assessing treatment responses.
PROCEDURES:
A comprehensive review of the literature was conducted to analyze advancements in PET imaging for sarcomas. Emphasis was placed on 18F-FDG PET/CT's role in complementing conventional imaging techniques, such as computed tomography (CT) and magnetic resonance imaging (MRI). Key aspects of PET imaging in musculoskeletal and cardiac tumors were examined, including its sensitivity and specificity in identifying metastases and its metabolic characterization of various tumor types.
RESULTS:
18F-FDG PET/CT has demonstrated high sensitivity and specificity in detecting metastatic sarcoma lesions and grading musculoskeletal tumors, such as osteosarcoma, chondrosarcoma, and Ewing sarcoma. Its ability to provide metabolic insights has enhanced differentiation between benign and malignant tumors, including myxomas, lipomas, angiosarcomas, and leiomyosarcomas. Furthermore, in primary and secondary cardiac tumors, 18F-FDG PET/CT has proven valuable for treatment planning by offering detailed metabolic characterization.
CONCLUSIONS:
18F-FDG PET/CT serves as a critical imaging modality in the diagnosis, staging, and treatment monitoring of sarcomas. By complementing conventional imaging techniques, it enhances the accuracy of tumor characterization and facilitates improved clinical decision-making. Its application in both musculoskeletal and cardiac sarcomas underscores its growing significance in oncologic imaging, making it a valuable tool in optimizing patient outcomes.
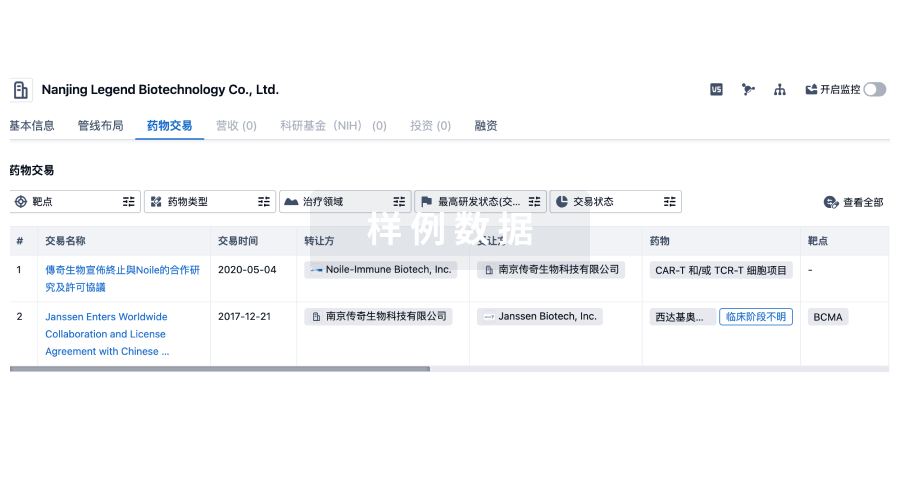
100 项与 Prospect Medical Holdings, Inc. 相关的药物交易
登录后查看更多信息
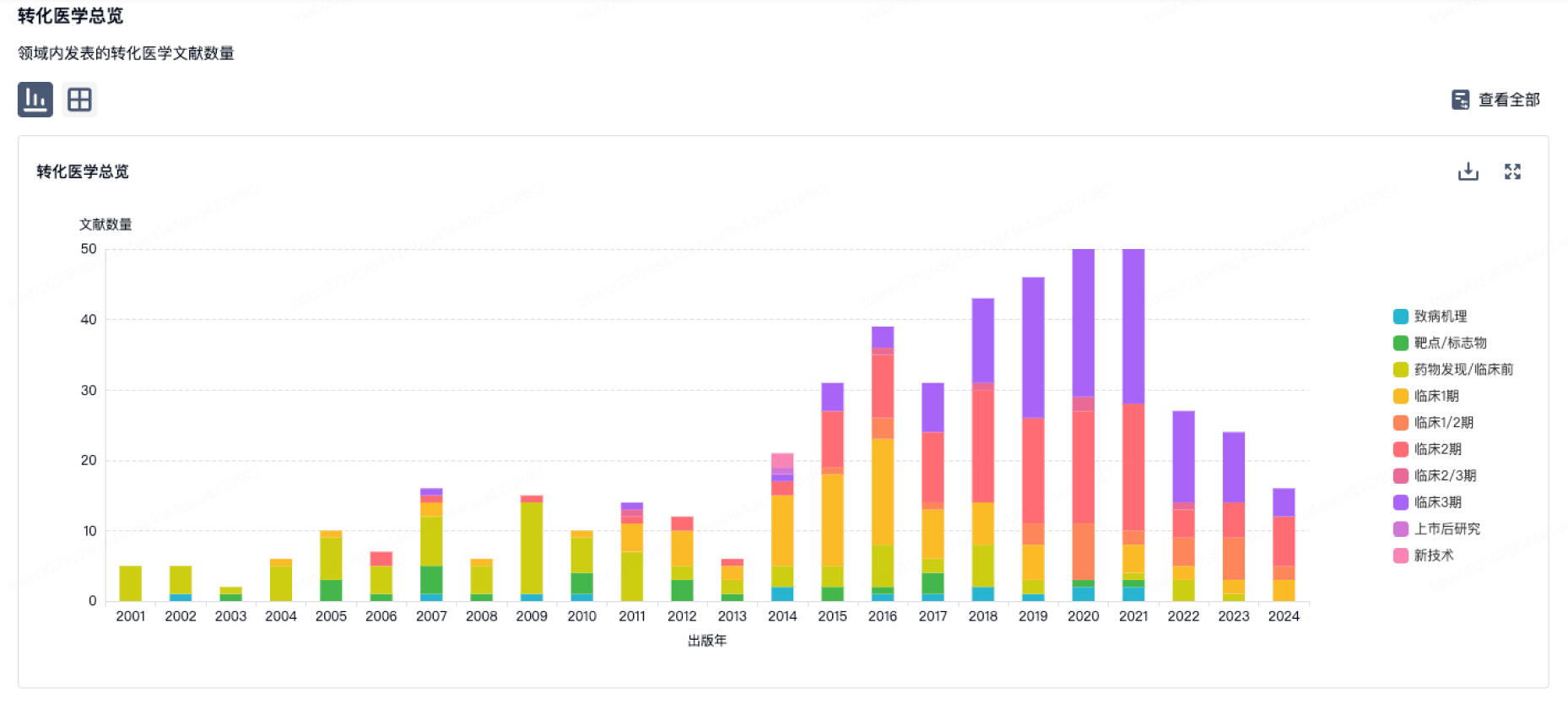
100 项与 Prospect Medical Holdings, Inc. 相关的转化医学
登录后查看更多信息
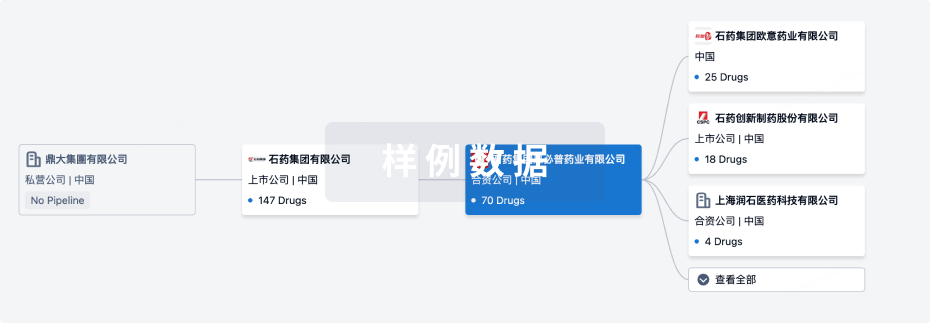
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月25日管线快照
无数据报导
登录后保持更新
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
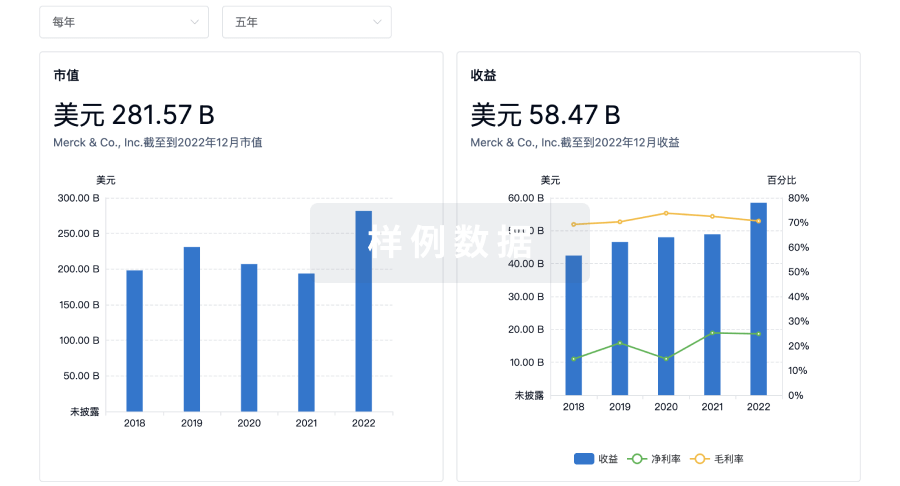
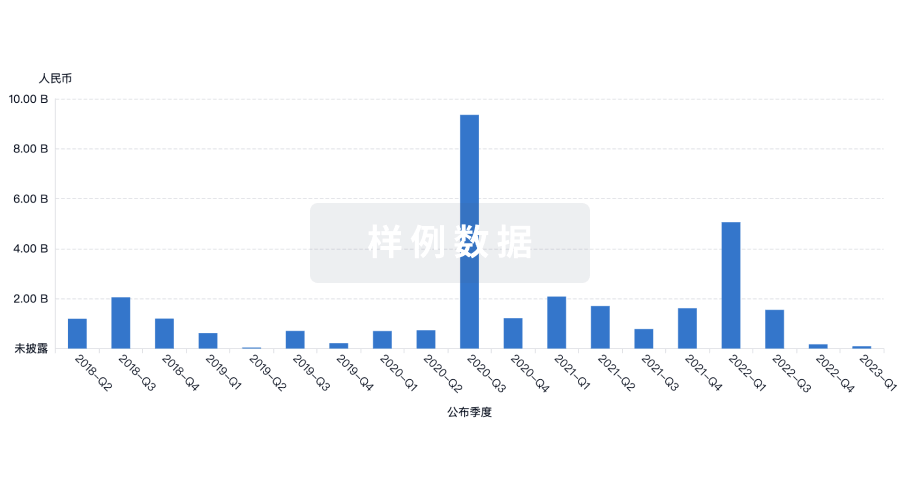
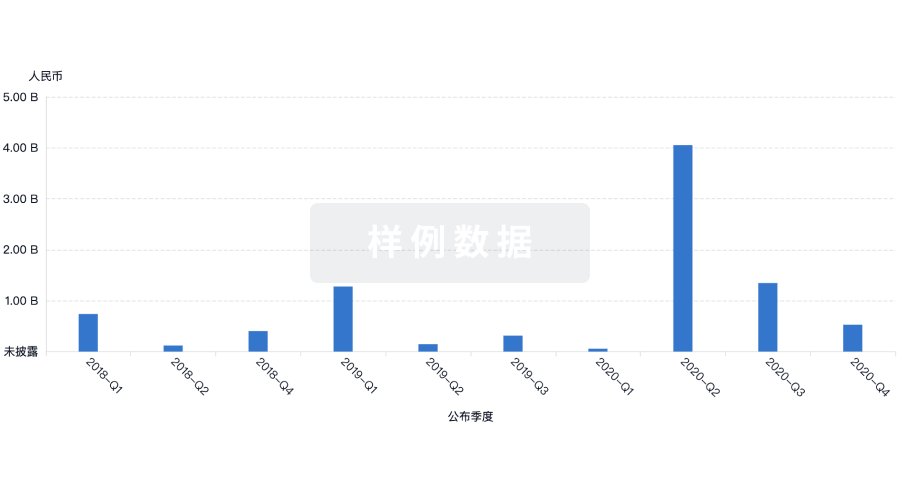
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用