预约演示
更新于:2025-05-07
CALCB
更新于:2025-05-07
基本信息
别名 Beta-CGRP、Beta-type CGRP、CALC2 + [6] |
简介 CALCB/CGRP2 is a peptide hormone that induces vasodilation mediated by the CALCRL-RAMP1 receptor complex (PubMed:1318039, PubMed:9620797). Dilates a variety of vessels including the coronary, cerebral and systemic vasculature. Its abundance in the CNS also points toward a neurotransmitter or neuromodulator role (PubMed:3492492). |
关联
100 项与 CALCB 相关的临床结果
登录后查看更多信息
100 项与 CALCB 相关的转化医学
登录后查看更多信息
0 项与 CALCB 相关的专利(医药)
登录后查看更多信息
138
项与 CALCB 相关的文献(医药)2025-04-01·Allergy
Human Pulmonary Neuroendocrine Cells Respond to House Dust Mite Extract With PAR ‐1 Dependent Release of CGRP
Article
作者: Armbruster, Marie ; Puttagunta, Lakshmi ; Mandal, Shivani ; Forsythe, Paul ; Mann‐Nüttel, Ritu
2024-12-01·Neurology Genetics
Shared Genetics of Migraine and Gastrointestinal Disorders Implicates Underlying Neurologic Mechanisms Yet Heterogeneous Etiologies
Article
作者: Chasman, Daniel I. ; Staller, Kyle ; Chan, Andrew T. ; Rist, Pamela M. ; Guo, Yanjun
2024-05-01·European Journal of Neuroscience
Characterizing enteric neurons in dopamine transporter (DAT)‐Cre reporter mice reveals dopaminergic subtypes with dual‐transmitter content
Article
作者: Gruenheid, Samantha ; Premachandran, Shobina ; Recinto, Sherilyn Junelle ; Yaqubi, Moein ; Mukherjee, Sriparna ; Stratton, Jo Anne ; Allot, Alexis ; MacDonald, Adam ; Trudeau, Louis‐Eric
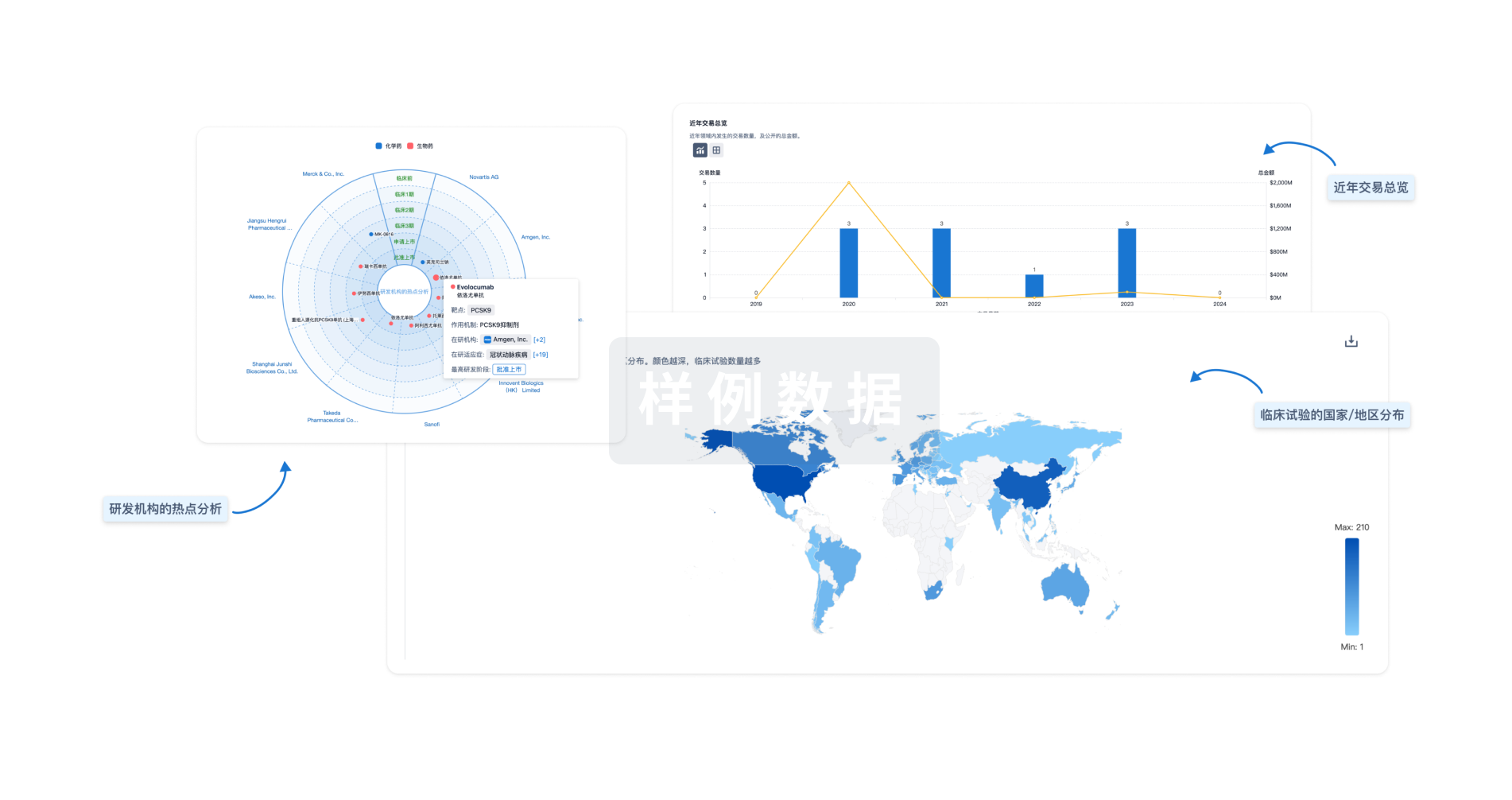
分析
对领域进行一次全面的分析。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用