预约演示
更新于:2025-05-07
RECK
更新于:2025-05-07
基本信息
别名 hRECK、RECK、reversion inducing cysteine rich protein with kazal motifs + [3] |
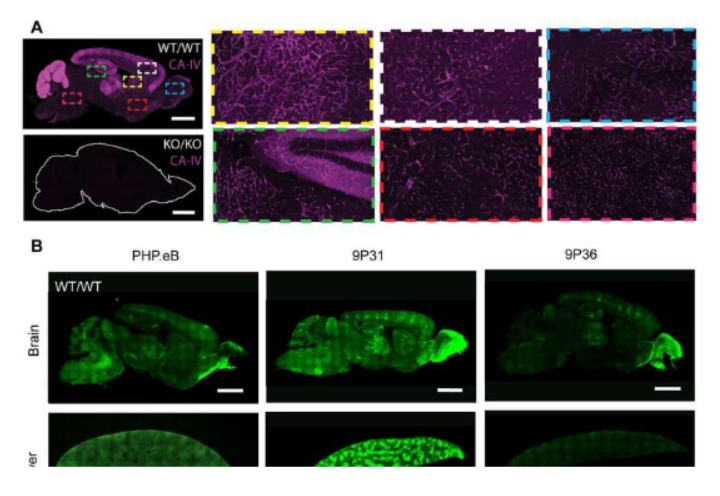
简介 Functions together with ADGRA2 to enable brain endothelial cells to selectively respond to Wnt7 signals (WNT7A or WNT7B) (PubMed:28289266, PubMed:30026314). Plays a key role in Wnt7-specific responses: required for central nervous system (CNS) angiogenesis and blood-brain barrier regulation (By similarity). Acts as a Wnt7-specific coactivator of canonical Wnt signaling by decoding Wnt ligands: acts by interacting specifically with the disordered linker region of Wnt7, thereby conferring ligand selectivity for Wnt7 (PubMed:30026314). ADGRA2 is then required to deliver RECK-bound Wnt7 to frizzled by assembling a higher-order RECK-ADGRA2-Fzd-LRP5-LRP6 complex (PubMed:30026314). Also acts as a serine protease inhibitor: negatively regulates matrix metalloproteinase-9 (MMP9) by suppressing MMP9 secretion and by direct inhibition of its enzymatic activity (PubMed:18194466, PubMed:9789069). Also inhibits metalloproteinase activity of MMP2 and MMP14 (MT1-MMP) (PubMed:9789069). |
关联
100 项与 RECK 相关的临床结果
登录后查看更多信息
100 项与 RECK 相关的转化医学
登录后查看更多信息
登录后查看更多信息
2025-05-01The Spine Journal
Ropivacaine-epinephrine-clonidine-ketorolac is an effective opioid-sparing local anesthetic for patients undergoing posterior spinal fusion
Article
作者: Rahm, Mark D ; Soto, Jose M ; Keith, Kristin A ; Lyon, Kristopher A ; Nguyen, Anthony V ; Huang, Jason H
2025-03-01International Journal of Medical Microbiology
Nasopharyngeal carriage of Staphylococcus aureus in a rural population, Sierra Leone
Article
作者: Rudolf, Viktoria ; Sesay, Maxwell ; Theiler, Tom ; Sesay, Desmond Mohamed ; Mellmann, Alexander ; Schaumburg, Frieder ; Grobusch, Martin P ; Grebe, Tobias ; Kleine, Lisa Maria ; Kanu, Emmanuel Marx ; Loismann, Henning ; Kalkman, Laura C
2025-03-01European Journal of Clinical Microbiology & Infectious Diseases
Multiple regional outbreaks caused by global and local VIM-producing Klebsiella pneumoniae clones in Poland, 2006–2019
Article
作者: Palma, Federica ; Żabicka, Dorota ; Gniadkowski, Marek ; Izdebski, Radosław ; Biedrzycka, Marta ; Brisse, Sylvain ; Urbanowicz, Paweł
分析
对领域进行一次全面的分析。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用