预约演示
更新于:2026-05-30
Nav1.8 inhibitor (Huilun Pharmaceutical)
Nav1.8抑制剂(汇伦医药)
更新于:2026-05-30
概要
基本信息
原研机构 |
在研机构 |
非在研机构- |
权益机构- |
最高研发阶段临床前 |
首次获批日期- |
最高研发阶段(中国)临床前 |
特殊审评- |
关联
100 项与 Nav1.8抑制剂(汇伦医药) 相关的临床结果
登录后查看更多信息
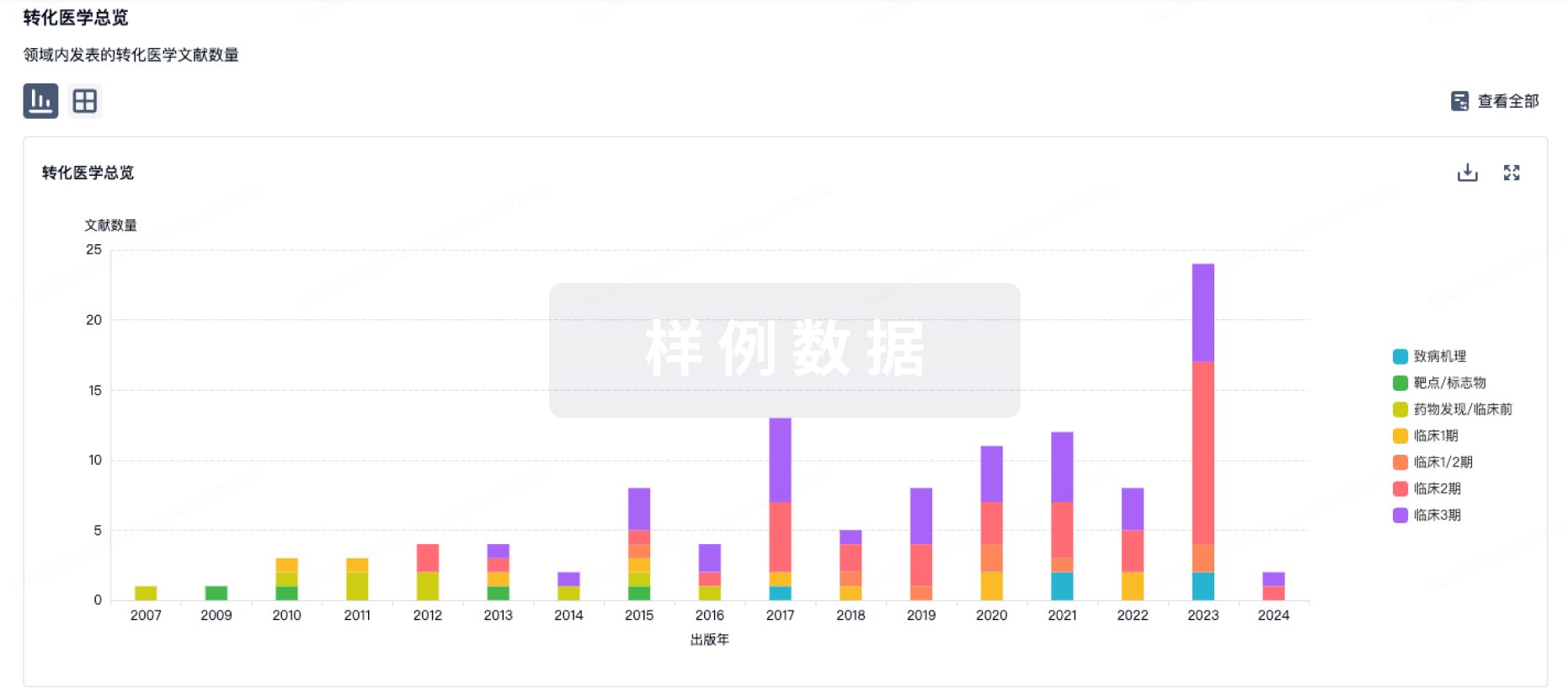
100 项与 Nav1.8抑制剂(汇伦医药) 相关的转化医学
登录后查看更多信息
100 项与 Nav1.8抑制剂(汇伦医药) 相关的专利(医药)
登录后查看更多信息
16
项与 Nav1.8抑制剂(汇伦医药) 相关的文献(医药)2026-04-01·Current Opinion in Anesthesiology
Suzetrigine, a selective NaV1.8 inhibitor in acute and chronic pain: mechanistic insights, clinical outcomes, and future perspectives
Review
作者: Swisher, Matthew W. ; Liu, Matthew A. ; Chen, Steven L.
Purpose of review:
The opioid epidemic and limitations of current nonopioid analgesics have created a need for safer, effective pain therapies. Suzetrigine, a first-in-class selective NaV1.8 inhibitor, was approved by the Food and Drug Administration in 2025 for the treatment of moderate to severe acute pain. The purpose of this review is to discuss the mechanism and clinical efficacy of suzetrigine and its potential for addressing existing therapeutic gaps in pain management.
Recent findings:
Phase 3 trials have demonstrated that suzetrigine provides a statistically significant and clinically meaningful reduction in acute postoperative pain compared to placebo, with efficacy similar to hydrocodone/acetaminophen and a favorable safety profile. Mechanistic studies confirm selective peripheral NaV1.8 inhibition, minimizing central nervous system effects and abuse potential. Ongoing research is evaluating suzetrigine for chronic pain conditions including diabetic peripheral neuropathy and lumbosacral radiculopathy, though long-term efficacy and safety remain to be established.
Summary:
Suzetrigine represents a promising nonopioid alternative for acute pain and has the potential to fill a significant gap in pain management. While initial results are encouraging, future studies are needed to define its role in chronic pain and multimodal analgesia, and to establish long-term safety.
2026-04-01·INTERNATIONAL DENTAL JOURNAL
Suzetrigine as a Complementary Analgesic in Dentistry: Evidence, Limitations, and Future Directions for a Novel NaV1.8 Inhibitor
作者: Nahm, William J ; Park, Tiffany H ; Job, Allen J
2026-03-06·MEDICINE
Suzetrigine (a NaV1.8 inhibitor) versus placebo for acute postoperative pain: A systematic review and meta-analysis of randomized controlled trials
Review
作者: Alvarez-Aguilar, Pablo ; Picado-Loaiza, Susimar
Background::
NaV1.8 channels, expressed in peripheral nociceptors, mediate sustained pain signaling. Their inhibition offers a potential opioid-sparing strategy for postoperative pain, although efficacy and safety remain incompletely defined. We synthesized randomized evidence for suzetrigine versus placebo in postoperative pain.
Methods::
We conducted a Preferred Reporting Items for Systematic Reviews and Meta-Analyses-compliant meta-analysis of randomized controlled trials comparing suzetrigine (a NaV1.8 inhibitor) versus placebo in surgical patients. The primary outcome was 24-hour pain with the Numeric Pain Rating Scale; secondary outcomes included 48-hour pain, change-from-baseline, and adverse events. Risk of bias was assessed with the Cochrane Risk of Bias 2 tool, and for analyses, we used Hartung–Knapp models with heterogeneity and prediction intervals reported. Random-effects models used Hartung–Knapp adjustments (2-sided α = 0.05).
Results::
We included 4 randomized datasets across 2 phase 3 publications (n = 1584; 1009 intervention, 575 placebo). The mean participant age was 44.9 years; 92.3% were women. Procedures included abdominoplasty (n = 823) and bunionectomy (n = 761). Suzetrigine significantly reduced pain at 24 hours (mean difference = −0.93; 95% confidence interval [CI], −1.38 to −0.48;
I2
= 66.0%) and 48 hours (mean difference = −1.02; 95% CI, −1.32 to −0.72;
I2
= 11.8%). Analyses of change-from-baseline confirmed consistent benefit. Subgroup analyses revealed similar effects across surgery types. A lower incidence of nausea (risk ratio = 0.63; 95% CI, 0.42–0.95) and dizziness (risk ratio = 0.57; 95% CI, 0.34–0.96) was observed in the suzetrigine group, with no significant differences in headache, vomiting, or constipation. Meta-regressions showed no moderation by sample size or publication year. Risk of bias was low in 2 studies and raised “some concerns” in 2.
Conclusion::
Suzetrigine produced modest reductions in pain at 24 to 48 hours versus placebo. Because opioid consumption was not consistently reported, no conclusions can be drawn regarding opioid-sparing.
181
项与 Nav1.8抑制剂(汇伦医药) 相关的新闻(医药)2026-05-27
2026
BX-2501片
Nav1.8抑制剂
前言
/ Foreword
↓
2026年4月,武汉熙瑞医药科技有限公司自主研发的新型口服镇痛药——BX-2501片(规格10mg,受理号CXHL2600421;规格50mg,受理号CXHL2600422)正式获得国家药品监督管理局药品审评中心(CDE)的IND受理,标志着该项目正式进入临床开发阶段。
01
靶点清晰,机制明确
BX-2501是一款高选择性Nav1.8抑制剂。Nav1.8通道主要表达于外周伤害感受神经元,在痛觉信号由外周向中枢神经系统的传导中发挥关键作用。通过阻断该通道,BX-2501可在不作用于中枢神经系统的情况下实现镇痛,避免阿片类药物的成瘾性与耐受性问题。
Fig.1
Nav1.8在躯体和内脏组织伤害感受神经元的作用机理[1]
02
临床前数据亮眼,优于同类上市药物
在多项临床前研究中,BX-2501表现出:
01
高抑制活性与优异选择性
对Nav1.8的抑制活性(IC50=0.291 nM)与上市药物Suzetrigine(VX-548)相当,同时对其他Nav亚型(如Nav1.1、Nav1.5、Nav1.7等)选择性显著更优,心脏安全性更佳。
02
更快的起效速度
在小鼠、大鼠、犬及健康受试者中,口服达峰时间(Tmax)为0.25~1.5小时,显著快于VX-548。
03
更高的口服生物利用度
小鼠(71.4%)、大鼠(48.0%)中均优于VX-548。
04
多种疼痛模型验证有效
在醋酸扭体、足切口、坐骨神经痛等模型中均显著减轻疼痛反应,镇痛效果稳定。
05
良好的安全性
hERG IC50>30 μM,无致突变性,在大鼠14天重复给药毒性试验中300 mpk存活率100%,健康受试者7天重复给药未见严重不良事件。
BX-2501拟用于治疗中度至重度急性疼痛,市场潜力巨大。同类药物VX-548已于2025年获FDA批准上市,分析师预测其峰值年销售额可达50亿美元。国内已有恒瑞、宜昌人福、汇伦等企业跟进,BX-2501凭借其更优的PK特性和更快的起效时间,具备差异化竞争优势。
熙瑞计划于2026年6月正式启动I期临床研究,持续推进BX-2501的临床开发,力争早日为患者提供更安全、更有效的镇痛新选择。
可合作开发/转让,欢迎来电洽谈!
参考文献:1. Goodwin G, McMahon S B. The physiological function of different voltage-gated sodium channels in pain[J]. Nature Reviews Neuroscience, 2021, 22(5): 263-274.
THE END
商务合作:15807169865
扫码关注武汉熙瑞医药,获取更多药品研发资讯!
2026-05-13
今天,MSCI 剔除了健康元和恩华药业。
国内主流 MSCI 三大 ETF:512090、512380、512520
根据测算
健康元持有0.75亿左右
恩华药业持有1.3亿左右
恩华药业管线已经梳理过多次
今天梳理健康元管线,含子公司丽珠集团,丽珠生物,丽珠单抗,丽珠疫苗。
权属管线,健康元持有丽珠集团权益,47.18%,直接持有丽珠生物22.58%,健康元合计持有丽珠生物54%左右。丽珠生物1005持有丽珠单抗和丽珠疫苗
先看健康元管线
玛帕西沙韦(壹立康)
流感1类新药,对标国外,
机制:聚合酶抑制剂
进度:2026 年初获批上市,儿童剂型 III 期
意义:国内首个自主研发抗流感创新药
TSLP 单抗
靶点:TSLP
适应症:慢阻肺(COPD)、哮喘
进度:2026 年 3 月 进入 III 期(国内第一梯队)健康元药业集团股份有限公司
市场:国内约 1 亿 慢阻肺患者
MABA 双靶点吸入制剂
适应症:COPD、哮喘
进度:II 期临床中
Nav1.8 抑制剂
类别:非成瘾性镇痛药
机制:选择性钠离子通道阻断
进度:II 期
PREP 抑制剂(口服)
适应症:COPD
进度:I 期完成,II 期准备中
新型 β- 内酰胺酶抑制剂(+ 美罗培南)
适应症:重症肺炎(HAP/VAP)、超级细菌耐药
进度:2026 年 5 月 获临床批件
新一代糖皮质激素(吸入)
适应症:哮喘、COPD
进度:2026 年 3 月 获批临床
临床前 / 布局
呼吸领域:超 10 款创新药,5 个进入 II 期后
抗生素耐药、吸入制剂、口服呼吸药梯队
现在健康元不到200亿市值,
已经上市的还有10多款覆盖哮喘、COPD、支气管扩张、祛痰等。
沙美特罗替卡松吸入粉雾剂
适应症:哮喘、COPD 维持治疗
类别:LABA(长效 β2 受体激动剂)+ ICS(吸入糖皮质激素)复方制剂
妥布霉素吸入溶液
国内首个获批的吸入性抗生素
用于支扩
吸入用布地奈德混悬液
适应症:支气管哮喘
类别:吸入糖皮质激素(ICS),呼吸基础用药
丙酸氟替卡松雾化吸入用混悬液
适应症:哮喘、COPD 抗炎治疗
富马酸福莫特罗吸入溶液
适应症:哮喘、COPD 的支气管扩张
硫酸特布他林吸入溶液
适应症:支气管哮喘、慢性支气管炎等的支气管痉挛
异丙托溴铵气雾剂
适应症:慢性阻塞性支气管炎、肺气肿等 COPD 症状缓解
吸入用乙酰半胱氨酸溶液
适应症:祛痰,用于浓稠痰粘液过多的呼吸系统疾病
抗感染药物
美罗培南注射液
注射用亚胺培南西司他丁钠
盐酸莫西沙星氯化钠注射液
丽珠集团
艾普拉唑(质子泵抑制剂,龙头)、枸橼酸铋钾
银杏叶提取物、氯吡格雷、H001 胶囊(口服 IIa 因子抑制剂)
H001:II 期临床整理中,国内首创无需常规凝血监测
激素 / GnRH:亮丙瑞林微球(前列腺癌 / 内膜异位)
糖尿病 / 减重:司美格鲁肽注射液
丽珠生物
莱康奇塔单抗(IL-17A)上市审批
临床优势:III 期头对头 PASI100(49.5%)优于司库奇尤(40.2%)
托珠单抗(IL-6R)
类风湿关节炎、全身型幼年特发性关节炎
已上市,2025 年放量
其他:IL-23p19、双抗(临床前 / 早期)
疫苗
四价重组蛋白流感疫苗(LZSN2401)
技术:重组蛋白(CHO)+ 佐剂
进度:I 期完成(2025.11),筹备 II 期(2026 上半年)
国内地位:国内无同类上市,唯一重组蛋白流感在研第一梯队
生殖生物药
重组人促卵泡激素(r-FSH)
辅助生殖促排卵
进度:2026 年内获批上市
重组人绒促性素、尿促性素(已上市)
目前丽珠集团市值280亿,本身已经低估,丽珠集团一年利润近5年稳定在19-20亿附近
也就是说每年稳定给健康元贡献10亿利润。而目前健康元却200亿不到市值,还不算健康元自身的呼吸科管线,镇痛领域全球领先的靶点2期管线。
大家说健康元合理市值应该多少,是不是绝对性的低估。市场只给了呼吸科龙头,60亿市值,睁眼瞎。一年5个亿的公司,60亿,这到哪里去说逻辑。
2026-05-06
·肺科麻醉
感谢各位同道的支持。同时我们上海市肺科医院麻醉科目前招收进修医生,发进修届天花板级别补贴,还同等条件下优先提供在职研究生的机会,提供科研机会,协助经济型宿舍,名额有限,先到先得。有兴趣可以私信,当然关于肺科专科麻醉的一些问题也可以交流。
选择性靶向电压门控钠通道以实现镇痛:现状与未来方向
致编辑信
美国食品药品监督管理局(FDA)近期批准苏泽曲林(suzetrigine)作为电压门控钠通道1.8亚型(Nav1.8)选择性抑制剂用于急性疼痛治疗,这是镇痛药理学领域的里程碑。该药被誉为二十余年来首个专门针对疼痛设计的镇痛药,这一进展诞生于非阿片类替代药物的监管压力,以及电压门控钠通道(Nav)作为治疗靶点的科研热潮。
但这一创新并非孤立出现,相关临床经验早已证实其在神经病性疼痛中的价值,尤其适用于激惹型伤害感受器或Nav1.7突变患者等特定表型。
尽管这类药物不具备分子选择性,但其对失活态钠通道的亲和力与良好药效学特征,使其成为一线治疗失败后的替代方案。这一基于观察与表型调整的临床发展路径,在靶向药理学时代依然具有意义。疼痛表型的异质性强调了根据患者个体特征定制钠通道调控策略的重要性。
与之相对,苏泽曲林代表分子精准策略:它选择性抑制Nav1.8,该通道仅表达于外周伤害性神经元,对中枢神经系统与自主神经通路无活性。这种选择性提升了耐受性,避免了Nav1.7抑制剂常见的不良反应。尽管前景广阔,关键临床试验仍存在值得关注的方法学局限:研究仅在小型手术场景(腹壁成形术、拇外翻切除术)中开展,采用低效能阿片类药物作为对照,未报告使用非甾体抗炎药作为补救镇痛;此外,基于48小时数据将适应症外推至“一般性急性疼痛”,未在大型手术或持续性术后疼痛中验证。仍需进一步研究评估苏泽曲林在慢性疼痛中的疗效,因这类疼痛的疾病负担与治疗挑战差异显著。
在此背景下,Gordon等人的综述未提及维克曲林(vixotrigine,BIIB074)令人意外,因其具有互补且具备临床价值的特征。维克曲林是电压与使用依赖性的多亚型钠通道调节剂,作用靶点包括Nav1.7、Nav1.8与Nav1.9,在外周与中枢神经系统均有表达。在CONVEY研究——一项针对特发性或糖尿病相关性痛性小纤维神经病患者的2期富集入组、随机撤药试验中,维克曲林200mg每日两次较安慰剂显著降低疼痛评分,耐受性良好。尽管高剂量(350mg每日两次)未达到主要终点,但在患者总体印象变化量表中应答者比例更高,提示存在临床获益感知。
尽管维克曲林作为慢性疼痛中评估的导航调节剂具有相关性,但未被前述综述排除,缩小了非阿片类镇痛当前发展的范围。苏泽曲林获批用于急性疼痛,但其在慢性疼痛中的作用尚不明确;而维克曲林直接在持续性神经病性疼痛中完成评估,在研究时长、表型分型与功能终点方面方法学设计更完善,尽管尚未获FDA批准。这一缺失凸显了将分子进展与新兴临床证据整合,形成更全面论述的必要性。
苏泽曲林与维克曲林的对比引发批判性思考:如何将分子创新与积累的临床经验相结合?在靶向疗法日益主导的环境中,非选择性钠通道阻滞剂仍扮演何种角色?最重要的是,如何确保社会对非阿片类替代药物的需求,不会损害新型镇痛药审批的科学严谨性?
疼痛领域钠通道阻滞剂的发展历程——从甲酰胺类到分子选择性——是一部延续、精进与学习的叙事。理解这一轨迹不仅是历史视角问题,更是指导疼痛治疗未来决策与监管标准的关键。
摘要
电压门控钠通道在包括伤害感受器在内的可兴奋细胞产生动作电位的过程中发挥核心作用。部分钠通道亚型在伤害感受器中富集,且人类遗传学数据证实其与疼痛疾病相关,因此钠通道一直是关键的镇痛药物靶点。研发能以亚型特异性方式降低通道电导的小分子药物充满挑战,但Nav1.8通道阻滞剂苏泽曲林最终成功进入临床。选择性靶向钠通道亚型的其他策略还包括抗钠通道适配体与寡核苷酸、RNA编辑、亚型特异性抗体以及靶向蛋白降解技术。我们期待,近期苏泽曲林获批用于急性疼痛治疗,仅仅是一系列新型钠通道靶向镇痛药问世的开端。
1引言
电压门控钠通道是可兴奋细胞产生动作电位所必需的,其中优先表达于外周感觉神经元的钠通道亚型已被证实与人类疼痛疾病相关。形成孔道的钠通道α亚基是一条长多肽,包含4个同源结构域(DI-DIV),每个结构域均有高度保守的6个跨膜片段(S1-S6),功能上组成电压感受结构域(S1-S4)与孔道模块(S5-S6及P环)。9种钠通道亚型在孔道内衬跨膜片段、通道功能元件(选择性滤孔、激活与失活门)的序列高度保守,这为研发靶向这些结构的通道抑制剂带来挑战。而细胞外环、跨膜片段连接区及胞内区域的序列差异,则为研发亚型选择性镇痛药提供了丰富基础,例如可降低细胞膜上通道密度的小分子通道抑制剂或生物制剂。本文就研发小分子钠通道抑制剂用于镇痛的成功经验、面临挑战,以及使用生物制剂和基因疗法靶向这些通道的未来机遇进行综述。
2如何实现钠通道的选择性靶向
生物学合理性与遗传学验证均支持靶向外周神经元钠通道以实现镇痛,其中Nav1.7与Nav1.8是镇痛药物研发中最成熟的靶点(图1)。研发临床有效的小分子抑制剂困难重重,目前临床使用的钠通道抑制剂均为非选择性,其对心脏与中枢神经系统钠通道的阻断相关不良反应,限制了其作为镇痛药的全身应用。仅作用于外周神经元的亚型选择性钠通道抑制剂,有望扩大治疗窗。
多数在人体或非人灵长类中测试的靶向钠通道电导的治疗药物,利用孔道模块与电压感受结构域的微小序列差异实现亚型选择性。例如,芳磺酰胺类抑制剂结合Nav1.7电压感受结构域4的胞外位点,实现对其他亚型的选择性,且表现为通道的状态与使用依赖性抑制。ST-2560是另一种非状态依赖的Nav1.7选择性抑制剂,源自石房蛤毒素。近期研究显示,Nav1.8抑制剂VX548(苏泽曲林)与LTGO-33结合电压感受结构域2,通过稳定通道闭合构象抑制Nav1.8。这种对Nav1.8的抑制可被高频去极化解除,提示这类分子以反向使用依赖性方式发挥作用;但近期研究发现,在37℃生理温度下采用动作电位指令的生理相关刺激,无法解除苏泽曲林或LTG-33对Nav1.8的抑制,提示该作用机制不太可能限制这类分子的治疗潜力。包括抗体与毒素衍生物在内的大分子,是另一类不断发展的钠通道抑制剂,可在体内产生镇痛效果。
显著拓展疼痛领域钠通道靶向治疗手段的新机遇,是靶向通道表达而非电导。反义寡核苷酸用于抑制Nav1.7翻译,CRISPR/Cas9用于表观遗传沉默Nav1.7表达。对钠通道(如Nav1.7)的mRNA进行编辑,使其通道可通透钠、钾离子但不通透钙离子,可形成电分流减弱感觉神经元放电,进而实现镇痛。另一种策略是阻断钠通道与已知调控因子的相互作用,例如CRMP2与Nav1.7、Magi-1与Nav1.8。近期研究鉴定出一种肽适配体,可结合河豚毒素敏感型通道(而非河豚毒素抵抗型通道)的保守短线性基序,降低感觉神经元兴奋性并产生镇痛作用。利用靶向蛋白降解技术,概念验证研究显示,通过亚型选择性蛋白降解靶向嵌合体招募泛素连接酶,可降解钠通道。目前已研发出选择性靶向Nav1.8通道的蛋白降解靶向嵌合体,可触发内源性通道表面表达降低,进而使伤害感受器的高兴奋性恢复正常。
绝大多数新兴基因治疗策略采用腺相关病毒将遗传物质递送至神经元。这类方法具有诸多优势:治疗作用持续时间更长;可直接递送至靶组织;不依赖蛋白质翻译后修饰与通道状态;作用可覆盖形态复杂的感觉神经元所有区域。但腺相关病毒治疗存在重要安全性考量,在治疗研发中需谨慎应对。其他致死性神经系统疾病对基因治疗反应极佳,且基因递送技术(包括非病毒递送方法)持续进步。
3我们从临床研发中获得哪些启示?
在编码Nav1.8通道的SCN10a基因被克隆近30年后,选择性靶向钠通道实现镇痛的早期愿景终于落地临床,近期美国食品药品监督管理局批准苏泽曲林用于中重度急性疼痛治疗即是例证。苏泽曲林是Nav1.8选择性抑制剂,临床前测试证实其可降低人类背根神经节的放电。美国食品药品监督管理局的批准基于两项术后急性疼痛的3期随机、双盲、安慰剂与阳性对照试验,结果显示苏泽曲林较安慰剂显著减轻疼痛。该审批属于术后镇痛优先审批程序,阿片类药物与此类术后镇痛的持续使用相关,凸显了非成瘾性镇痛药的需求。Nav1.8不表达于自主神经元与中枢神经系统,苏泽曲林耐受性良好、不良反应少。
苏泽曲林在慢性神经病性疼痛疾病中的疗效尚未证实,目前正在开展更大规模临床试验。鉴于当前慢性神经病性疼痛一线药物疗效与耐受性不佳,该领域存在重要临床需求。临床前研究支持Nav1.8在慢性神经病性疼痛中的作用,但在临床明确验证该靶点前,仍需更多数据。
Nav1.7在伤害感受器放电中的非冗余作用,以及其与疼痛相关的显著人类遗传学数据,推动了众多镇痛药物研发项目。早期芳磺酰胺类抑制剂蛋白结合率高,导致血神经屏障穿透性差、游离药物浓度低,这可能是其在人类临床试验中疗效不佳的原因。后续研发了该类别的新型抑制剂,以及源自石房蛤毒素、成药性更优的药物,可阻断C纤维伤害感受器传导并减轻非人灵长类疼痛行为,但这些药物在非人灵长类与人体中均出现心血管反射受损。这反映Nav1.8不同,Nav1.7表达于交感神经元。与之相对,携带Nav1.7双等位基因功能缺失突变的先天性无痛患者无自主神经症状或体位性低血压,提示发育过程中可出现代偿作用。有研究提出,药物药代动力学(药物浓度升高速率)与自主神经不良反应相关,或可在避免自主神经效应的同时实现镇痛。部分疼痛疾病采用这类抑制剂局部给药可能有效,仅靶向感觉神经元中Nav1.7的空间限制性基因治疗策略也具备优势。
疼痛医学或需实现个体化,以反映个体间差异(包括钠通道的遗传变异)。已有研究证实,这不仅对遗传性红斑肢痛症等单基因疼痛疾病中非选择性钠通道阻滞剂的疗效至关重要,也适用于小纤维神经病等更常见疾病,还可能涉及痛性糖尿病神经病——罕见钠通道变异是该病疼痛的危险因素。若拥有针对特定钠通道亚型的有效治疗药物,明确个体基因型将对治疗选择具有重要意义。
4结论
Nav1.8抑制剂苏泽曲林获批用于急性疼痛治疗令人振奋,因为这是数十年来首个专门针对疼痛设计的获批镇痛药。但该药效应量较小,提示其单药治疗存在潜在局限。尽管其具备阿片类药物节俭潜力,但相较于当前急性疼痛治疗药物,苏泽曲林成本较高,可能限制其应用。多种钠通道原子结构的解析,以及人工智能用于计算机药物发现,有望加速新型镇痛药研发。更深入理解靶点相关不良反应以制定缓解策略,以及采用局部而非全身给药方式,可扩大可治疗疾病的范围。新型生物制剂与基因治疗前景广阔,尤其是其作用方式为降低质膜通道水平,而非抑制电导。尽管Nav1.7抑制剂临床研发失败使钠通道靶向镇痛的热情有所降温,但未来依然光明;Nav1.8抑制剂获批提示,学界与工业界坚持研发钠通道靶向镇痛药终将收获回报。
翻译:辛平平
审校:卫世有
原始文献:Gordon EA, Tyagi S, Dib-Hajj SD, Bennett DL. Selective targeting of voltage-gated sodium channels to achieve analgesia: current status and future directions. Pain. 2025 Nov 1;166(11S):S42-S46. doi: 10.1097/j.pain.0000000000003639. PMID: 41086326.
100 项与 Nav1.8抑制剂(汇伦医药) 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 心律失常 | 临床前 | 中国 | 2024-03-07 | |
| 腓骨肌萎缩症 | 临床前 | 中国 | 2024-03-07 | |
| 咳嗽 | 临床前 | 中国 | 2024-03-07 | |
| 多发性硬化症 | 临床前 | 中国 | 2024-03-07 | |
| 疼痛 | 临床前 | 中国 | 2024-03-07 | |
| 尿失禁 | 临床前 | 中国 | 2024-03-07 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
| 研究 | 分期 | 人群特征 | 评价人数 | 分组 | 结果 | 评价 | 发布日期 |
|---|
No Data | |||||||
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
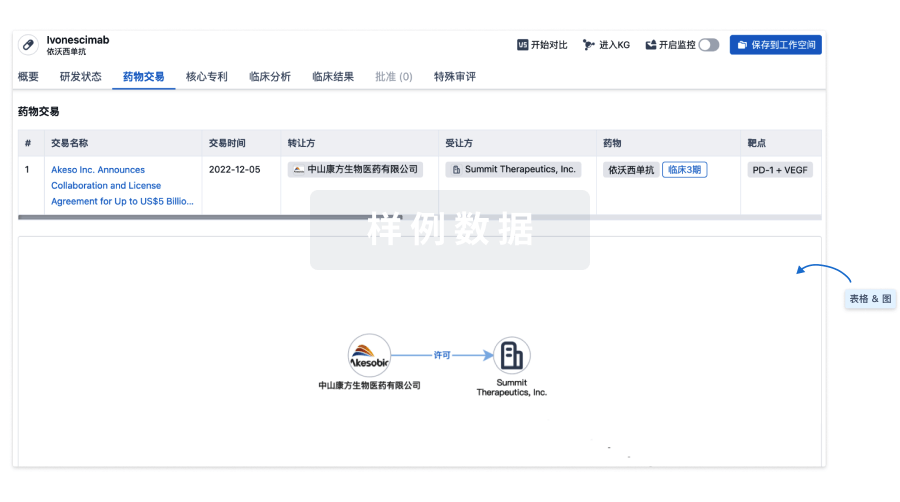
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
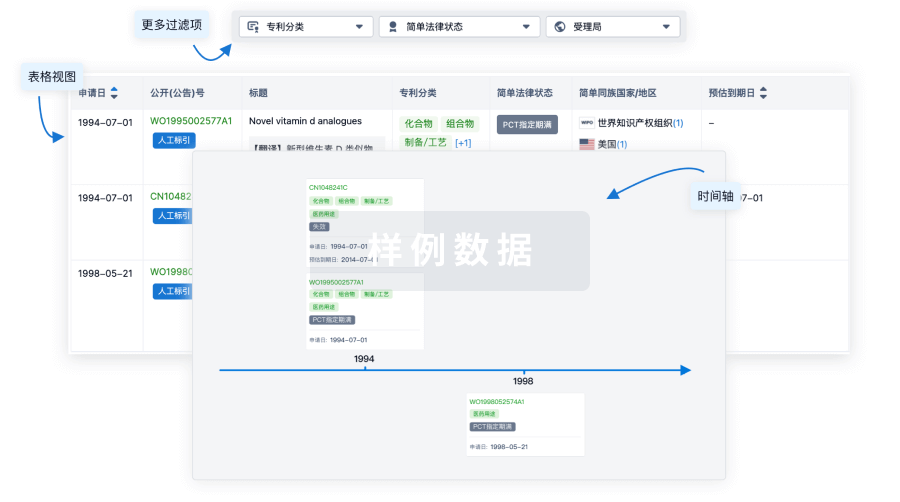
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
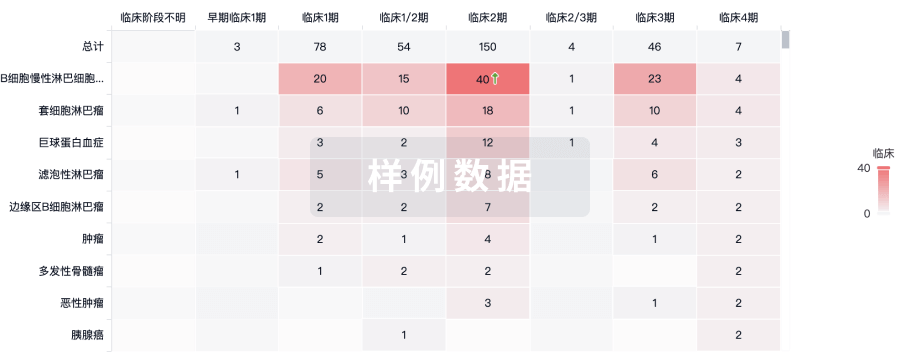
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用