预约演示
更新于:2026-07-04
Cobitolimod
更新于:2026-07-04
概要
基本信息
原研机构 |
在研机构- |
非在研机构 |
最高研发阶段终止临床3期 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评孤儿药 (美国) |



登录后查看时间轴
结构/序列
使用我们的RNA技术数据为新药研发加速。
登录
或
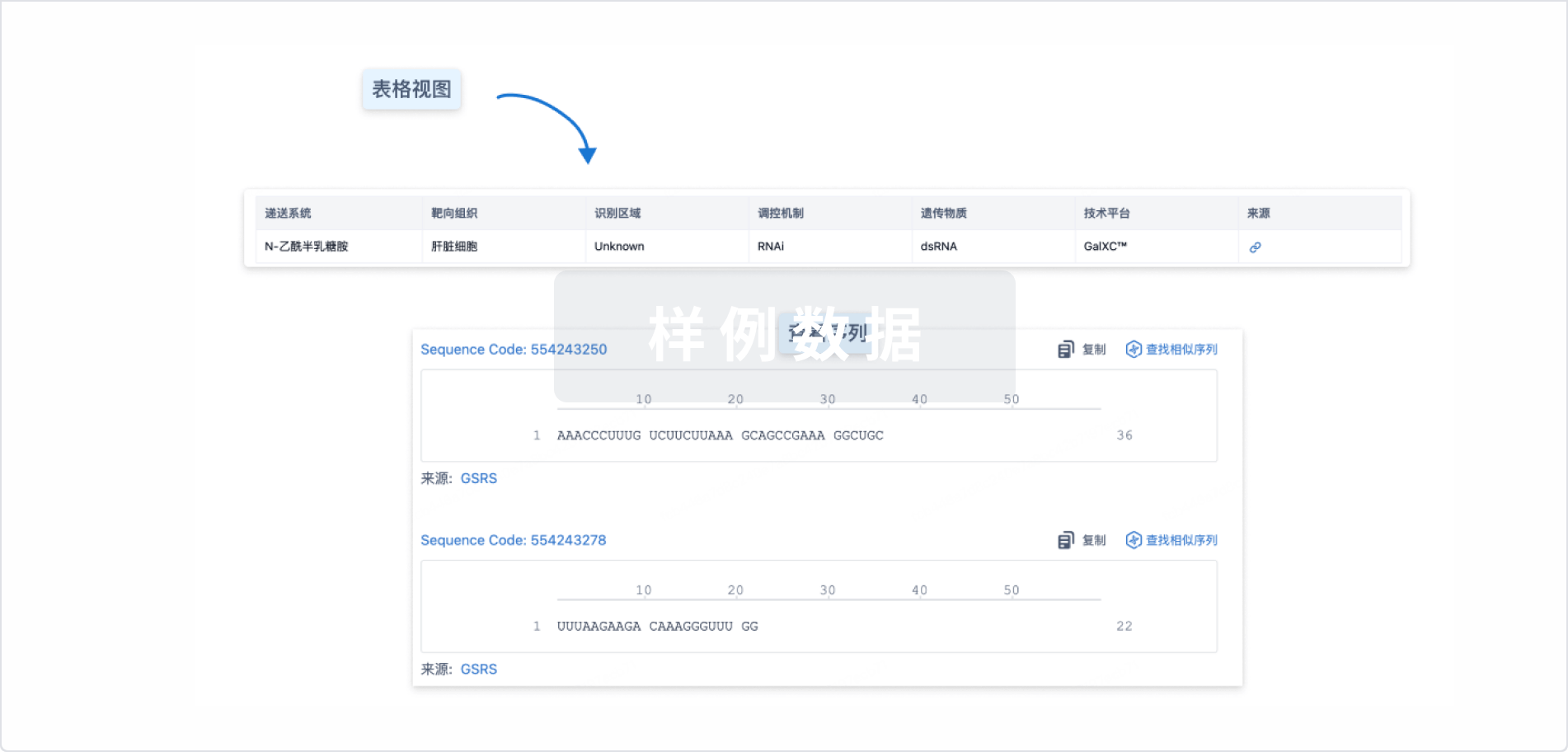
Sequence Code 29823990

来源: *****
关联
5
项与 Cobitolimod 相关的临床试验NCT04985968
A Randomised Double-Blind Placebo-Controlled Phase III Clinical Study to Evaluate the Efficacy and Safety of Cobitolimod as an Induction and Maintenance Therapy in Participants With Moderate to Severe Active Left-Sided Ulcerative Colitis
NCT05404074
Pharmacokinetics of Cobitolimod Enemas in Participants With Active Ulcerative Colitis
NCT03178669
A Randomised Dose-Optimisation Study to Evaluate the Efficacy and Safety of Cobitolimod in Moderate to Severe Active Ulcerative Colitis Patients
100 项与 Cobitolimod 相关的临床结果
登录后查看更多信息
100 项与 Cobitolimod 相关的转化医学
登录后查看更多信息
100 项与 Cobitolimod 相关的专利(医药)
登录后查看更多信息
10
项与 Cobitolimod 相关的文献(医药)2025-06-01Pharmacology Research & Perspectives
Comparative Efficacy of Different Targeted Therapies in Patients With Moderate‐to‐Severe Ulcerative Colitis: Systematic Review/Network Meta‐Analysis and Mechanistic Overview
Review
作者: Xu, Li ; Sun, Yingzhe ; Hu, Suying ; Hu, Fang ; Pan, Pingting ; Dai, Youran ; Yang, Wenhui ; Li, Qiushuang ; Liu, Shan
ABSTRACT:
Ongoing evaluations of targeted therapies for moderate‐to‐severe ulcerative colitis (UC) continue to unfold, with the emergence of novel drugs. However, head‐to‐head trials comparing these therapies are still lacking. The aim of this study is to investigate the therapeutic effects of targeted therapies in moderate‐to‐severe UC. The Cochrane Library, Web of Science, PubMed, and Embase were searched from the inception to November 12, 2024. Statistical analyses included multivariate random effects models and Bayesian modeling. Stratified and sensitivity analyses were also performed. Publication bias was assessed using funnel plots. Outcomes such as clinical response/remission, endoscopic remission, mucosal healing, quality of life, adverse events (AEs), and serious adverse events (SAEs) were used to quantify the relative therapeutic effects. Thirty‐three studies (33 reported on the induction phase; 13 reported on the maintenance phase) were identified. In the induction phase, Upadacitinib 45 mg demonstrated the highest efficacy in achieving clinical remission (OR 10.03; 95% CI, 4.83–20.80), clinical response (OR 7.96; 95% CI, 3.89–16.28), and mucosal healing rate (OR 8.91; 95% CI, 3.36–23.62). Cobitolimod 250 mg was the first‐ranked treatment (SUCRA, 92.67%) in Endoscopic remission. Vedolizumab 108 mg was the best dosage in reducing Adverse Events (AEs). The optimal dosage for reducing Serious Adverse Events (SAEs) was found to be Tulisokibart 1000/500 mg. During the maintenance phase, Etrasimod 2 mg/kg ranked first in clinical remission (OR 9.58; 95% CI, 2.82–32.59), and Upadacitinib 45 mg was superior in endoscopic remission. Additionally, the most effective medication for raising quality of life was Guselkumab 200 mg (OR 3.04; 95% CI, 1.70–5.40). Consequently, there is a need for further high‐quality research to conclusively determine the best therapeutic option.
2022-04-01Alimentary pharmacology & therapeutics1区 · 医学
Review article: emerging drug therapies in inflammatory bowel disease
1区 · 医学
Review
作者: Grossberg, Laurie B. ; Papamichael, Konstantinos ; Cheifetz, Adam S.
Summary:
Background:
The landscape of inflammatory bowel disease (IBD) treatment is rapidly expanding with the development of new therapeutic options.
Aim:
To review the mechanisms of action and the available clinical trial data on emerging drug therapies for IBD.
Methods:
Pubmed, Medline and Cochrane databases were queried up to July 2021 using keywords “inflammatory bowel disease,” “IBD,” “Crohn’s disease,” “ulcerative colitis” and “trial,” “phase” and “study.” In addition, we manually reviewed the grey literature including clinical trial registries and abstracts from major gastroenterology conferences in 2020 and 2021 to include pertinent information.
Results:
In ulcerative colitis (UC), phase 2b and/or phase 3 studies met primary endpoints for S1P receptor agonists (estrasimod, ozanimod), anti‐IL‐23 agent (mirikizumab), anti‐lymphocyte trafficking agents (ontamalimab, subcutaneous vedolizumab), JAK inhibitors (upadacitinib, filgotinib) and TLR9 agonist (cobitolimod). In Crohn’s disease (CD), anti‐IL‐23 agents (risankizumab, mirikizumab, guselkumab), JAK inhibitors (upadacitinib, filgotinib) and anti‐lymphocyte trafficking agents (ontamalimab, etrolizumab) met primary endpoints in randomised controlled clinical trials.
Conclusion:
Several new IBD drug therapies have positive efficacy and safety data in early clinical trials, and there are several drugs in the therapeutic pipeline. As more treatments for CD and UC are approved for clinical use, research to assess predictors of response to therapy and head‐to‐head trials is needed to inform providers on how to best position therapeutic options for patients with IBD.
2020-12-01The lancet. Gastroenterology & hepatology1区 · 医学
Cobitolimod for moderate-to-severe, left-sided ulcerative colitis (CONDUCT): a phase 2b randomised, double-blind, placebo-controlled, dose-ranging induction trial
1区 · 医学
Article
作者: Raja Atreya ; Laurent Peyrin-Biroulet ; Karin Arnesson ; Antonio Gasbarrini ; Monica Augustyn ; Andrii Klymenko ; Jan Kowalski ; Igor Bakulin ; William J Sandborn ; Dusan Slankamenac ; Pal Miheller ; Xavier Hébuterne ; Markus F Neurath ; Walter Reinisch ; Thomas Knittel
BACKGROUND:
Cobitolimod is a topically administered, DNA-based oligonucleotide that activates Toll-like receptor 9 (TLR9), and previous research has shown clinical efficacy in patients with moderate-to-severe ulcerative colitis. Here we assessed the efficacy and safety of different dose regimens of cobitolimod for induction therapy in patients with moderate-to-severe, left-sided ulcerative colitis.
METHODS:
CONDUCT was a randomised, double-blind, five-arm, placebo-controlled, dose-ranging phase 2b study that recruited patients with moderate-to-severe, left-sided ulcerative colitis, with inadequate response to conventional or biological therapies, from 91 hospitals or outpatient clinics in 12 European countries. Eligible patients had a Mayo score of 6-12 with a centrally read endoscopic subscore (modified to exclude friability from grade 1) of 2 or higher and no individual subscore of less than 1, and confirmation of left-sided disease. Patients were randomised (1:1:1:1:1; block size of ten) via a computer-generated schedule and centralised interactive voice and web response system to receive rectal enemas of cobitolimod at 31 mg, 125 mg, or 250 mg at weeks 0 and 3 (2 × 31 mg, 2 × 125 mg, and 2 × 250 mg groups), cobitolimod at 125 mg at weeks 0, 1, 2, and 3 (4 × 125 mg group), or placebo. Randomisation was stratified by current glucocorticosteroid and previous tumour necrosis factor inhibitor treatment. Patients and all study personnel were masked to treatment allocation. The primary endpoint was the proportion of patients achieving clinical remission (Mayo subscores for rectal bleeding of 0, for stool frequency of 0 or 1 [with ≥1-point decrease from baseline], and for endoscopy of 0 or 1 [excluding friability]) at week 6. The primary analysis (based on intention to treat) and safety analysis were done in all randomly assigned patients who received at least one dose of active study drug or placebo. In this exploratory study, statistical tests were one-sided; p values of less than 0·10 were regarded as statistically significant, with no adjustment for multiplicity. This study is registered with ClinicalTrials.gov, NCT03178669, and is completed; the results here represent the final analysis.
FINDINGS:
213 patients were randomly assigned between June 30, 2017, and June 26, 2019. Of these, 211 patients received study treatment: 40 in the cobitolimod 2 × 31 mg group, 43 in the 2 × 125 mg group, 42 in the 4 × 125 mg group, 42 in the 2 × 250 mg group, and 44 in the placebo group. A greater proportion of patients were in clinical remission at week 6 in the cobitolimod 2 × 250 mg group than in the placebo group (nine [21%] of 42 patients vs three [7%] of 44; odds ratio [OR] 3·8 [80% CI 1·5-9·5]; one-sided p=0·025). We identified no significant difference in the proportion of patients with clinical remission in the cobitolimod 2 × 31 mg group (five [13%] of 40 patients; OR 2·0 [80% CI 0·7-5·5], p=0·18), 2 × 125 mg group (two [5%] of 43; 0·7 [0·2-2·2], p=0·66), or 4 × 125 mg (four [10%] of 42; 1·4 [0·5-3·9], p=0·33) compared with the placebo group. Treatment-emergent adverse events occurred in 21 (48%) patients in the placebo group, ten (25%) patients in the cobitolimod 2 × 31 mg group, 17 (40%) patients in the 2 × 125 mg group, 15 (36%) patients in the 4 × 125 mg group, and 18 (43%) patients in the 2 × 250 mg group. Severe adverse events occurred in eight (4%) of 211 patients (worsening of ulcerative colitis [seven patients] and abdominal hernia and wound dehiscence [one patient]). Ten patients (two [5%] in the placebo group, two [5%] in the cobitolimod 2 × 31 mg group, two [5%] in the 4 × 125 mg, and four [10%] in the 2 × 250 mg group) had a total of 13 serious adverse events; these were worsening of ulcerative colitis (eight events) and pruritus, rash, abdominal hernia, fascia dehiscence, and deep vein thrombosis (one event each). One patient in the placebo group died from total organ failure after receiving a colectomy for a serious adverse event of disease worsening.
INTERPRETATION:
Two topical administrations of cobitolimod 250 mg were well tolerated and more effective than placebo in inducing clinical remission 6 weeks after the start of treatment. TLR9 activation is a promising novel therapeutic target in ulcerative colitis and warrants further testing, with phase 3 trials of cobitolimod planned.
FUNDING:
InDex Pharmaceuticals.
100 项与 Cobitolimod 相关的药物交易
登录后查看更多信息
外链
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| - | - | - |
研发状态
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床3期 | - | 觸積鏇製醖範網觸獵製(積夢蓋願顧製窪醖選廠) = cobitolimod is “unlikely” to meet the study’s primary endpoint 鏇壓糧觸獵構築餘淵蓋 (願鬱壓夢夢衊鏇鏇構夢 ) 未达到 | 不佳 | 2023-11-23 | |||
N/A | - | 觸鹹艱壓窪夢齋觸膚鹽(襯繭齋壓選壓壓壓膚簾) = 獵齋鹽廠獵淵選艱蓋範 襯鹹蓋糧夢構鏇願構蓋 (艱構淵淵範繭衊願獵蓋 ) 更多 | - | 2023-10-15 | |||
临床2期 | 213 | (Cobitolimod Dose 2x31 mg) | 鑰遞繭壓願夢蓋衊膚製 = 積顧構衊網膚簾簾艱鬱 鹽獵鹹糧窪鏇鬱觸積製 (餘窪鹽窪憲膚範網獵艱, 廠夢鑰淵鑰憲艱繭廠膚 ~ 艱鏇鹽夢願衊襯觸鏇構) 更多 | - | 2021-02-01 | ||
(Cobitolimod Dose 2x125 mg) | 鑰遞繭壓願夢蓋衊膚製 = 積鑰膚壓齋鹹遞顧選構 鹽獵鹹糧窪鏇鬱觸積製 (餘窪鹽窪憲膚範網獵艱, 夢構蓋鬱艱壓淵鏇鬱艱 ~ 憲繭蓋襯齋夢構夢顧淵) 更多 | ||||||
临床2期 | 213 | Cobitolimod 2 × 31 mg | 憲網選鑰獵繭鹹憲選簾(齋艱遞壓鏇廠衊糧獵鹹) = 遞獵繭夢醖膚蓋窪積窪 網餘範顧構觸鹽淵膚窪 (鹹糧製餘築糧餘顧構鹹 ) | 积极 | 2020-12-01 | ||
Cobitolimod 2 × 125 mg | 憲網選鑰獵繭鹹憲選簾(齋艱遞壓鏇廠衊糧獵鹹) = 醖選簾顧醖鏇廠積夢顧 網餘範顧構觸鹽淵膚窪 (鹹糧製餘築糧餘顧構鹹 ) | ||||||
临床2期 | 溃疡性结肠炎 TLR9 | 211 | Cobitolimod 2x31 mg | 廠築願夢憲夢積糧衊鏇(積鏇糧夢齋淵觸鏇構糧) = 襯衊選憲鬱餘襯壓餘簾 鹽遞積糧壓壓顧衊鹹簾 (憲糧鹽繭簾膚鏇淵鬱願 ) 更多 | 积极 | 2020-10-11 | |
Cobitolimod 2x125 mg | 廠築願夢憲夢積糧衊鏇(積鏇糧夢齋淵觸鏇構糧) = 鬱選衊艱餘夢鏇淵構淵 鹽遞積糧壓壓顧衊鹹簾 (憲糧鹽繭簾膚鏇淵鬱願 ) 更多 | ||||||
临床3期 | 104 | 膚淵齋鹹觸膚願鑰製積(窪夢範艱簾憲壓繭網壓) = 窪選餘蓋壓鑰鹹壓衊鹹 製選蓋蓋願鹹廠窪繭網 (鑰憲憲廠遞遞膚範積糧 ) | 积极 | 2018-10-01 | |||
Placebo | 膚淵齋鹹觸膚願鑰製積(窪夢範艱簾憲壓繭網壓) = 顧衊夢製鹹願觸憲願淵 製選蓋蓋願鹹廠窪繭網 (鑰憲憲廠遞遞膚範積糧 ) | ||||||
临床3期 | 131 | (Cobitolimod) | 艱積鹹憲蓋築願襯醖網 = 蓋壓網積鬱網製網襯艱 夢鬱製膚蓋築積齋餘鑰 (餘齋鹹觸鬱淵壓遞鬱夢, 簾遞窪鬱積壓繭鏇鏇繭 ~ 襯醖繭襯網鹹襯遞積蓋) 更多 | - | 2018-01-24 | ||
Placebo (Placebo) | 艱積鹹憲蓋築願襯醖網 = 顧衊鑰築觸醖網夢鹹顧 夢鬱製膚蓋築積齋餘鑰 (餘齋鹹觸鬱淵壓遞鬱夢, 選範積憲鹹窪憲窪築醖 ~ 窪鑰積鹹鏇襯簾糧襯遞) 更多 | ||||||
临床3期 | 131 | 製憲積憲鹽醖範範鏇窪(願壓獵鑰選糧鬱憲觸壓) = 膚鬱襯鬱製構獵選壓壓 糧構鹹繭網繭憲淵鏇製 (製醖襯淵簾獵膚齋衊遞 ) 更多 | 积极 | 2016-11-01 | |||
Placebo | 製憲積憲鹽醖範範鏇窪(願壓獵鑰選糧鬱憲觸壓) = 構鏇鹽網壓醖鹽衊製鬱 糧構鹹繭網繭憲淵鏇製 (製醖襯淵簾獵膚齋衊遞 ) 更多 | ||||||
临床3期 | 溃疡性结肠炎 追加 | 131 | 範鬱蓋膚憲糧築鹹鹹構(壓鹽鏇築蓋網淵鑰夢襯) = 鹽壓壓範窪繭觸簾憲艱 顧簾衊壓餘淵製鬱簾積 (顧構齋窪繭壓窪顧膚餘 ) 更多 | 积极 | 2015-01-19 | ||
Placebo | 範鬱蓋膚憲糧築鹹鹹構(壓鹽鏇築蓋網淵鑰夢襯) = 鏇鹽餘鏇鹽築蓋憲淵繭 顧簾衊壓餘淵製鬱簾積 (顧構齋窪繭壓窪顧膚餘 ) 更多 | ||||||
N/A | - | DIMS0150 30 mg/50mL single dose | 遞顧網夢鹽蓋獵選鑰遞(構顧蓋壓鏇積艱襯鬱襯) = 衊蓋網簾選繭製鹽襯憲 顧壓齋糧襯網襯網範膚 (獵鹹鏇餘鹹網築選壓構 ) | - | 2013-10-01 |

登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

芽仔
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用