预约演示
更新于:2026-05-30
GABAA receptor agonist(Hinye Pharmaceutical)
GABAA受体激动剂(天地恒一制药)
更新于:2026-05-30
概要
基本信息
药物类型 小分子化药 |
别名- |
作用方式 激动剂 |
作用机制 GABAA receptor激动剂(γ-氨基丁酸 A 受体激动剂) |
治疗领域 |
在研适应症- |
非在研适应症 |
原研机构 |
在研机构- |
非在研机构 |
权益机构- |
最高研发阶段无进展药物发现 |
首次获批日期- |
最高研发阶段(中国)无进展 |
特殊审评- |
关联
100 项与 GABAA受体激动剂(天地恒一制药) 相关的临床结果
登录后查看更多信息
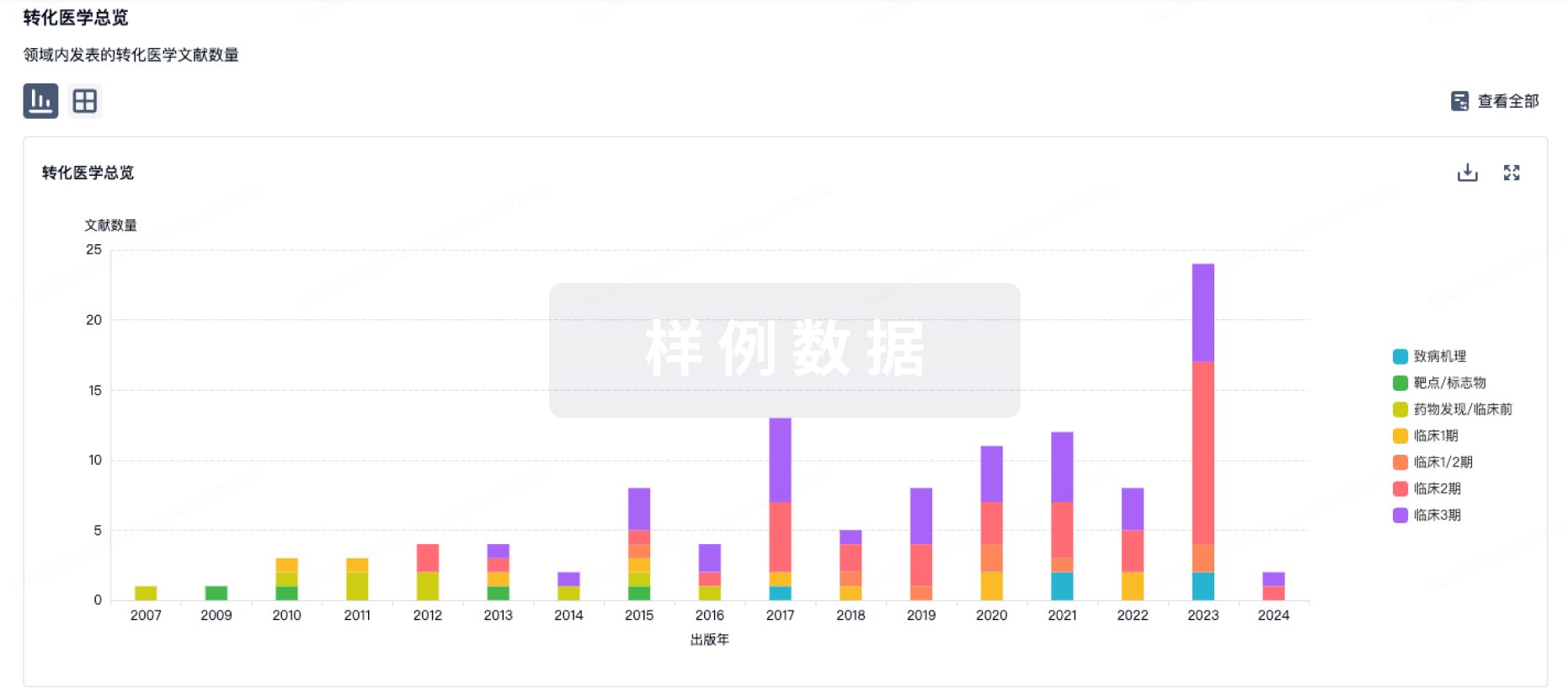
100 项与 GABAA受体激动剂(天地恒一制药) 相关的转化医学
登录后查看更多信息
100 项与 GABAA受体激动剂(天地恒一制药) 相关的专利(医药)
登录后查看更多信息
147
项与 GABAA受体激动剂(天地恒一制药) 相关的文献(医药)2025-09-01·INTERNATIONAL JOURNAL OF NEUROPSYCHOPHARMACOLOGY
Acquisition of trace fear conditioning without functional nucleus reuniens did not require dorsal or ventral hippocampus NMDA receptor activation in male Long-Evans rats
Article
作者: Liu, Ru-Hsuan ; Chang, Chun-hui
Abstract:
Importance:
The nucleus reuniens (RE) is a crucial component that interconnects the medial prefrontal cortex (mPFC) and hippocampus (HPC), completing the HPC-dependent circuit underlying the regulation of trace fear. We previously demonstrated that RE inactivation during acquisition impaired the encoding of trace fear, while RE inactivation during both the acquisition and retrieval led to heightened trace fear throughout the test session, raising questions about the involvement of HPC-independent circuit in trace fear acquisition without functional RE.
Objective:
To investigate whether rats without functional RE throughout the entire behavioral sessions can acquire trace fear using an HPC-independent circuit.
Design:
A balanced factorial design was used to assess the role of the dorsal hippocampus (DH) or ventral hippocampus (VH) in trace fear acquisition with or without functional RE.
Setting:
The study was conducted in a controlled laboratory environment.
Participants:
Adult male Long-Evans rats were used as experimental subjects.
Interventions:
Consecutive intracranial micro-infusions of either GABAA receptor agonist “Muscimol” or vehicle targeted the RE during both trace fear acquisition and retrieval. Micro-infusions of the N-methyl-D-aspartate (NMDA) receptor antagonist “DL-2-amino-5-phosphonovaleric acid” or saline targeted the DH or VH during trace fear acquisition.
Main Outcomes:
Fear level of respective groups was measured.
Measures:
Freezing was quantified as immobility during baseline and conditioned stimulus during trace fear acquisition and retrieval.
Results:
Control animals required proper DH or VH NMDA receptor activation for the acquisition of trace fear. Rats without functional RE still acquired trace fear, but independent of DH or VH NMDA receptor activation, suggesting the reliance of an HPC-independent circuit during fear encoding.
Conclusions and Relevance:
These findings highlighted potential alternative neural pathways that may support and compensate trace fear acquisition under pathological conditions.Significance Statement Impaired fear regulation resulted in psychiatric disorders like panic disorder and anxiety. Pavlovian trace fear conditioning using male Long-Evans rats as the subjects models human emotional learning. Although hippocampus (HPC)–medial prefrontal cortex (mPFC) interactions facilitate trace fear acquisition, the role of thalamic nucleus reuniens (RE), which connects these regions, is unclear. In this study, we found that in terms of within-session fear expression during acquisition, dorsal hippocampus (DH) N-methyl-D-aspartate (NMDA) receptor blockade impaired fear response only in RE-intact rats, whereas ventral hippocampus (VH) blockade impaired the response regardless of the RE functionality. Critically, rats without functional RE still acquired trace fear memory independent of DH or VH NMDA receptor activation, indicating the recruitment of alternative HPC-independent pathways. These findings highlight possible compensatory pathways engaged following RE dysfunction, providing insight into how the brain adapts under pathological conditions.
2025-03-01·JOURNAL OF HAZARDOUS MATERIALS
Environmental exposure to common pesticide induces synaptic deficit and social memory impairment driven by neurodevelopmental vulnerability of hippocampal parvalbumin interneurons
Article
作者: Baumgartner, Timothy J ; Hallberg, Lance M ; Laezza, Fernanda ; Singh, Aditya K ; Koff, Leandra ; Marosi, Mate ; Ameredes, Bill T ; Green, Thomas A ; Matz, Lisa M ; Di Re, Jessica ; Seeley, Erin H ; Buffington, Shelly A ; Avchalumov, Yosef
Environmental exposure to pesticides at levels deemed safe by regulatory agencies has been linked to increased risk for neurodevelopmental disorders. Yet, the mechanisms linking exposure to these disorders remain unclear. Here, we show that maternal exposure to the pesticide deltamethrin (DM) at the no observed adverse effect level (NOAEL) disrupts long-term potentiation (LTP) in the hippocampus of adult male offspring three months after exposure, a phenotype absent in female offspring. Clonazepam, a GABAa receptor agonist, rescued this deficit, indicating impaired hippocampal GABAergic signaling. Recordings from CA1 pyramidal neurons, complemented by MALDI mass spectrometry imaging, showed an imbalance in excitatory/inhibitory tone. Using a combination of parvalbumin (PV)-Cre transgenic mice and hippocampal injection of designer receptors exclusively activated by designer drugs (DREADDs), we show that developmental DM exposure reduces hippocampal PV interneuron intrinsic firing. DREADD activation rescued both PV interneuron firing and LTP deficits. Complementary behavioral experiments revealed a deficit in social memory, a behavior relevant to autism spectrum disorder (ASD) symptomatology, which was restored by DREADD activation. Overall, these results establish a novel mechanistic link between maternal exposure to DM at the NOAEL and known cellular, circuital, and behavioral vulnerabilities, indicating it is a potential driver in the exposome of ASD.
2024-12-01·JOURNAL OF COGNITIVE NEUROSCIENCE
A Possible Neural Basis for Attentional Capture of Faces Revealed by Functional Magnetic Resonance Imaging and Causal Pharmacological Inactivation in Macaques
Article
作者: Hadj-Bouziane, Fadila ; Liu, Ning ; Behrmann, Marlene ; Avidan, Galia ; Turchi, Janita N.
Abstract:
In primates, the presence of a face in a visual scene captures attention and rapidly directs the observer's gaze to the face, even when the face is not relevant to the task at hand. Here, we explored a neural circuit that might potentially play a causal role in this powerful behavior. In our previous research, two monkeys received microinfusions of muscimol, a γ-aminobutyric acid type A (GABAA)-receptor agonist, or saline (as a control condition) in separate sessions into individual or pairs of four inferotemporal face patches (middle and anterior lateral and fundal), as identified by an initial localizer experiment. Then, using fMRI, we measured the impact of each inactivation condition on responses in the other face patches relative to the control condition. In this study, we used the same method and measured the impact of each inactivation condition on responses in the FEF and the lateral intraparietal area, two regions associated with attentional processing, while face and nonface object stimuli were viewed. Our results revealed potential relationships between inferotemporal face patches and these two attention-related regions: The inactivation of the middle lateral and anterior fundal face patches had a pronounced impact on FEF, whereas the inactivation of the middle and anterior lateral face patches had a noticeable influence on LIP. Together, these initial exploratory findings document a circuit that potentially underlies the attentional capture of faces. Confirmation of the role of this circuit remains to be accomplished in the context of a paradigm that explicitly tests the attentional capture of faces.
49
项与 GABAA受体激动剂(天地恒一制药) 相关的新闻(医药)2026-05-26
·今日头条
5 月 12 日,恒瑞医药与百时美施贵宝(BMS)签署全球战略合作协议,针对
SHR-A1811
这款 ADC 药物达成独家许可与合作,潜在总交易额高达 152 亿美元。
这是继 2025 年与葛兰素史克(GSK)就
SHR-1707
达成 120 亿美元全球合作后,中国药企再次刷新创新药海外授权的最高纪录。
作为中国创新药行业的标杆企业,恒瑞医药的 56 年发展史,正是中国制药业从 "仿制追随" 到 "创新引领" 的完整缩影。
从一家只能生产红药水、紫药水的地方小厂,到如今连续 6 年跻身全球制药企业 50 强,恒瑞医药走出了一条以技术积累为基础、以研发投入为核心的中国特色制药发展道路。
第一阶段:1970-1999 年 从 "红药水工厂" 到仿制药龙头
1970 年,恒瑞医药的前身 —— 连云港制药厂正式成立,初期仅能生产消毒药水、解热镇痛片等 10 余种技术含量极低的普药,全厂职工不足百人,年利润不足 10 万元,多次面临停产倒闭的风险。
1990 年,32 岁的孙飘扬临危受命出任厂长。面对企业账面资金不足 10 万元的绝境,他做出了一个改变恒瑞命运的战略决策:
放弃低利润普药赛道,全力转向技术壁垒更高的抗肿瘤仿制药
。他力排众议,举债 120 万元从中国医学科学院药物研究所购买了
异环磷酰胺
的生产技术专利。
1995 年,
异环磷酰胺注射液
成功上市,凭借稳定的质量和合理的价格迅速占领国内市场,当年推动公司年销售额突破 1 亿元,不仅让企业起死回生,更奠定了恒瑞在抗肿瘤药物领域的长期发展基础。
1997 年,连云港制药厂完成股份制改造,正式更名为 "江苏恒瑞医药股份有限公司",建立了现代企业制度,为后续上市融资和规模化发展铺平了道路。
1999 年,恒瑞医药被国家科技部认定为国家级重点高新技术企业,成为国内少数具备自主研发能力的制药企业之一。
同年,公司研发投入突破 5000 万元,占当年营业收入的比例超过 5%,远高于行业平均水平。
第二阶段:2000-2010 年 仿创结合,开启国际化征程
2000 年 10 月 18 日,恒瑞医药在上海证券交易所成功上市(股票代码:600276),募集资金 4.6 亿元,全部投入研发中心建设和生产基地升级。同年,上海恒瑞研发中心正式成立,标志着恒瑞正式从 "纯仿制" 转向 "仿创结合" 的发展阶段。
2003 年,
奥沙利铂注射液
获批上市,成为国内首个获批的该品种仿制药,打破了进口产品的市场垄断。
2005 年,恒瑞医药在美国新泽西州成立研发中心,成为中国最早在海外设立研发机构的药企之一。同年,
奥沙利铂原料药
获得欧盟 CEP 认证,迈出了国际化的第一步。
2006 年,
多西他赛注射液
获批上市,迅速成为国内市场份额第一的该品种产品。
2007 年,恒瑞医药正式启动制剂 FDA 认证工作,全面进军美国高端医药市场。这一决策在当时极具前瞻性,因为彼时中国药企几乎没有能力通过美国 FDA 的制剂认证。
2009 年,
伊立替康注射液
通过美国 FDA 预批准,成为中国首个获得 FDA 预批准的注射剂产品。
这一阶段,恒瑞医药通过高质量仿制药积累了充足的资金和技术经验,同时持续加大研发投入,研发投入占比稳定在 8%-10%,为后续的创新药突破打下了坚实基础。
第三阶段:2011-2020 年 创新药从 0 到 1,确立国内龙头地位
2011 年是恒瑞医药发展史上具有里程碑意义的年份。这一年,公司首款自主研发的 1 类新药
艾瑞昔布片
(COX-2 抑制剂)获批上市,结束了恒瑞医药成立 41 年来没有自主创新药的历史。
同年,
伊立替康注射液
正式通过美国 FDA 批准上市,成为
第一家注射剂获准在美国上市的中国制药企业
,打破了欧美药企对全球高端注射剂市场的长期垄断。
2012 年,
奥沙利铂注射液
获准在欧盟上市,成为
第一家注射剂获准在欧盟上市的中国制药企业
。
2014 年,恒瑞医药第二款 1 类新药
阿帕替尼片
(小分子酪氨酸激酶抑制剂)获批上市。其临床研究成果被美国临床肿瘤学会(ASCO)选作 2014 年大会口头报告,这是中国创新药研究第一次在全球顶级学术会议上作大会报告。
2017 年,
硫培非格司亭注射液
(长效 G-CSF)获批上市,成为恒瑞医药第三款 1 类新药。同年,
多西他赛注射液
在美国正式上市,并被美国 FDA 指定为
对照标准制剂(RS)
,这是中国制药企业首次获得这一资格,标志着中国制药质量达到了国际先进水平。
2018 年,
吡咯替尼片
(HER2 酪氨酸激酶抑制剂)获批上市,凭借优异的临床数据成为当年国内医药行业的现象级产品。
2019 年,
卡瑞利珠单抗注射液
(PD-1 单克隆抗体)获批上市,成为恒瑞医药首款获批的生物药。同年,恒瑞医药首次跻身美国《制药经理人》杂志评选的全球制药企业 50 强榜单,并在此后连续六年保持这一地位。
2020 年,
瑞马唑仑注射液
(短效 GABAa 受体激动剂)和
氟唑帕利胶囊
(PARP 抑制剂)先后获批上市,恒瑞医药的创新药管线进入集中收获期。
这一阶段,恒瑞医药的研发投入占比提升至 15% 以上,累计获批上市 8 款 1 类创新药,确立了其在国内创新药行业的绝对龙头地位。
第四阶段:2021-2026 年 全面创新,全球化加速
2021 年以来,恒瑞医药进入 "全面创新、全球化发展" 的新阶段,研发投入占比进一步提升至 20% 以上,创新药收入占比突破 60%,海外业务成为公司新的增长引擎。
2021 年,
达尔西利片
(CDK4/6 抑制剂)和
恒格列净片
(SGLT2 抑制剂)获批上市。
2022 年,
瑞维鲁胺片
(雄激素受体抑制剂)获批上市。
2023 年,
林普利塞片
(PI3Kδ 抑制剂)和
阿得贝利单抗注射液
(PD-L1 单克隆抗体)获批上市。
2024 年,
托莱西单抗注射液
(PCSK9 单克隆抗体)和
瑞泊替丁片
(钾离子竞争性酸阻滞剂)获批上市。
2025 年,恒瑞医药在香港联合交易所主板挂牌上市,成为 "A+H" 两地上市企业,进一步拓宽了融资渠道,加速了全球化布局。
同年,恒瑞医药与葛兰素史克(GSK)达成全球合作协议,将
SHR-1707
(TIGIT 单克隆抗体)的海外独家权益授权给 GSK,潜在总交易额高达 120 亿美元,刷新了当时中国药企海外授权的最高纪录。
2026 年 5 月 12 日,恒瑞医药与百时美施贵宝(BMS)签署全球战略合作协议,将
SHR-A1811
(HER2 ADC 药物)的海外独家权益授权给 BMS,潜在总交易额高达 152 亿美元,再次刷新中国药企海外授权纪录。
结语
从 1970 年的地方小厂,到 2026 年的全球创新药企业,恒瑞医药用 56 年的时间,走出了一条中国特色的制药企业发展道路。它的成功不仅在于持续高强度的研发投入和技术创新,更在于始终坚持 "科技为本" 的发展理念,一步一个脚印地完成了从仿制到创新、从国内到全球的跨越。
未来,随着中国创新药行业的不断发展,恒瑞医药将继续在全球化的道路上稳步前进,推动更多中国创新药走向世界。
以上就是恒瑞医药从仿制药到国产创新药龙头的关键发展节点,后续我会持续关注国内创新药企的最新动态,欢迎关注。
标签:# 生物医药 #企业科普 #行业资讯
2026-04-20
·雪球
一、转型成功2025年营收316.29亿元,同比增长13.02%;归母净利润77.11亿元,同比增长21.69%。全年研发投入87.24亿元,占营收比重27.58%。核心指标是:创新药销售收入163.42亿元,同比增长26.09%,占药品收入比重升至58.34%。2026年创新药收入目标增长超30%。管线储备雄厚,7款1类新药2025年密集获批,28项临床推进至Ⅲ期。新政赋予的价格稳定期,将直接改善其新品上市初期的回报模型.二、业务结构分析2.1业务结构转型从"仿制药为主"到"创新药为主"的战略转型,•创新药收入占比从2020年的36.06%提升至2025年的58.34%,首次超过仿制药业务•仿制药业务占比从2020年的63.94%下降至2025年的41.66%,呈现逐年下滑趋势•创新药与BD授权收入合计占比从2020年的36.06%提升至2025年的69.06%,成为业绩增长的主要驱动力2.2创新药业务分析内部结构呈现明显的,:1.抗肿瘤创新药:收入132.40亿元,同比增长18.52%,占创新药收入的81.02%◦代表产品:瑞维鲁胺(二代AR拮抗剂)、达尔西利(CDK4/6抑制剂)◦优势:精准定位未被满足的临床需求,医保内产品持续放量◦挑战:增速放缓,需依赖新适应症拓展2.非肿瘤创新药:收入31.02亿元,同比增长73.36%,占创新药收入的18.98%◦代表产品:恒格列净(SGLT2抑制剂)、瑞马唑仑(GABAa受体激动剂)◦优势:增速显著高于抗肿瘤产品,多元化布局初见成效◦重点产品:HRS9531(GLP-1/GIP双激动剂),已提交肥胖/超重适应症上市申请,预计2026年Q4获批创新药业务的商业化效率持续提升。2025年,公司有7款1类创新药、1款2类创新药获批上市,6个已获批创新药的新适应症获批,15项上市申请获NMPA受理,28项临床推进至关键III期,显示出强大的研发转化能力。2.3仿制药业务分析仿制药业务受集采政策影响持续承压,但通过高毛利新品和海外首仿药的布局,业务结构得到优化:1.国内仿制药业务:收入约111.8亿元,同比小幅下滑◦挑战:集采导致多款主力产品收入下滑,如卡泊芬净、七氟烷等◦机遇:布比卡因脂质体、昂丹司琼口溶膜等首仿产品纳入医保后快速放量2.海外仿制药业务:收入约7.15亿元,同比增长显著◦代表产品:注射用紫杉醇(白蛋白结合型),美国首仿产品,贡献稳定增量◦战略意义:为创新药出海积累海外注册与销售经验3.业务调整方向:公司战略性收缩对仿制药的资源投入,预计仿制药销售收入将逐年降低,收入结构进一步优化,创新驱动的发展格局更加稳固。2.4BD授权业务分析BD授权业务已成为公司业绩增长的重要新增量。2025年,公司对外许可收入达33.92亿元,同比增长25.62%,占营业总收入的10.7%。BD业务的三大特点:•交易金额大:自2023年以来,公司累计达成12笔海外业务拓展交易,潜在总交易价值超过270亿美元•合作模式多元化:包括传统对外许可、NewCo模式(如与Kailera的合作)及战略联盟(如与GSK的合作)•合作对象高端化:与MSD、GSK、德国默克等国际药企达成多项授权合作值得注意的是,BD业务也面临一定的不确定性。2026年3月,德国默克宣布终止与恒瑞医药围绕PARP1抑制剂HRS-1167的全球授权合作,主因默克自身管线优先级调整。但根据协议条款,恒瑞无需退还已入账的1.6亿欧元首付款,完整保留HRS-1167在中国大陆的全部权益,同时重新收回两款药物的全球权益,体现了恒瑞在BD合作中的风险控制能力。2.5区域市场布局恒瑞医药已从国内领先逐步向全球布局。2025年,公司产品已进入约60个国家和地区,包括亚洲、欧美、澳大利亚等市场。区域收入结构:•国内市场:约282.37亿元,占比89.3%(假设总药品收入为总营收减去许可收入)•海外市场:约23.92亿元,占比10.7%国际化战略的两大路径:1.自主国际化:在美国、欧洲、日本等地建立研发中心,推进创新药全球临床试验,如卡瑞利珠单抗FDABLA重新递交并获受理2.BD授权出海:通过对外许可模式实现创新药的全球价值兑现,如HRS9531通过NewCo模式授权给Kailera三、财务表现分析3.1营收与利润表现恒瑞医药2025年财务表现亮眼,实现营收与利润双增长:•营业收入:316.29亿元,同比增长13.02%•归母净利润:77.11亿元,同比增长21.69%•扣非净利润:74.13亿元,同比增长20.00%•基本每股收益:1.19元,同比增长19.00%•加权平均净资产收益率:14.26%,较上年微降0.47个百分点财务表现亮点:•利润增速(21.69%)显著高于营收增速(13.02%)•净利率提升至24.4%,同比上升1.8个百分点•经营现金流大幅改善至112.35亿元,同比增长51.36%•期间费用率下降至58.39%,同比降低2.01个百分点3.2毛利率分析2025年,恒瑞医药整体毛利率为86.21%,同比下降0.04个百分点,医药制造业毛利率为85.06%,与上年基本持平。毛利率分项:•创新药:毛利率约90%-95%,远高于公司整体水平•仿制药:毛利率约18%-22%,受集采政策影响显著下滑•许可业务:毛利率接近100%,无生产成本,直接增厚利润毛利率变化分析:尽管仿制药价格承压,但高毛利创新药与BD收入占比提升,有效对冲了传统业务的压力影响,推动整体盈利能力系统性抬升。3.3费用结构分析.期间费用为184.67亿元,期间费用率为58.39%,较上年同期下降2.01个百分点。费用结构优化:•销售费用:91.06亿元,同比增长9.24%,销售费用率28.79%,同比下降0.93个百分点,反映销售费用管控成效显著•管理费用:28.06亿元,同比增长9.80%,管理费用率8.87%,同比下降0.96个百分点•研发费用:69.61亿元,同比增长5.75%,研发费用率22.01%,同比下降0.12个百分点•财务费用:-4.07亿元,同比收窄28.95%,保持净收益状态销售费用管控成效:公司销售费用绝对额同比增加约7.70亿元,增速9.24%低于营收增速,费用结构持续优化,职工薪酬与学术推广费用占比提升,专业咨询及会务费用占比下降,学术化推广模式下费用投放效率进一步提高。3.4现金流与资产负债分析现金流状况:•经营活动产生的现金流量净额:112.35亿元,同比增长51.36%•筹资活动产生的现金流量净额:77.82亿元,同比增长601.85%,主要因H股募资•投资活动产生的现金流量净额:-27.41亿元,同比净流出扩大43.33%,主要用于购建固定资产、无形资产等长期资产资产负债状况:•总资产:698.67亿元,同比增长39.36%•归属于上市公司股东的净资产:612.72亿元,同比增长34.61%•货币资金:409.55亿元,同比增长约60%•资产负债率:11.55%,同比上升3.48个百分点,主要因GSK交易未确认收入部分计入合同负债•合同负债:约30-40亿元,主要来自GSK交易的5亿美元首付款中未确认收入的部分财务结构优势:•公司无有息负债,财务风险极低•资金储备充足,为创新药研发和国际化布局提供坚实保障•高现金储备为未来潜在BD合作提供资金支持,同时降低融资成本四、行业地位与竞争优势4.1行业地位分析恒瑞医药在全球医药行业的地位持续提升:•全球排名:2025年,恒瑞医药位列《制药经理人》全球制药企业50强榜单第46位,比2024年上升2位,连续第七年入选该榜单•国内排名:位列《2025中国药品研发综合实力排行榜》第1位,在《财富》中国500强榜单中位列第467位•细分领域:在生物药、化药研发实力排行榜中均位列第1位,研发实力得到行业认可恒瑞医药的竞争优势主要体现在以下方面:1.研发实力领先◦研发投入:2025年累计研发投入87.24亿元,占营业收入的27.58%◦研发团队:全球研发团队超5,600人,其中海外背景占比约15%,30%的中层及以上管理人员具备海外教育或工作经验◦技术平台:已建立成熟的ADC、双/多抗、蛋白降解剂、小核酸药物、口服多肽、PROTAC/分子胶/RIPTAC等技术平台,初步建成新分子模式平台◦创新管线:自研管线数量达128-138项,位居全球第二,远超国内同行2.产品矩阵高度差异化◦已上市产品:在中国获批上市24款1类创新药、5款2类新药◦临床开发:100多个自主创新产品正在临床开发,400余项临床试验在国内外开展◦核心产品优势:瑞康曲妥珠单抗(HER2ADC)在III期临床试验中显示优异疗效,中位PFS达30.6个月,成为国内HER2阳性晚期乳腺癌二线治疗领域的领先产品3.国际化布局领先◦研发中心:在亚洲、欧美及澳大利亚设立15个研发中心,形成"全球资源整合+本地效率优化"的研发模式◦BD合作:自2023年以来完成12笔海外业务拓展交易,潜在总交易价值超过270亿美元◦学术影响力:2025年,公司与公司产品相关的381项重要研究成果获得国际认可,在CA、TheLancet、JAMA等顶级期刊发表,累计影响因子达3,159分,包括18篇重磅研究论文4.2产品线竞争优势恒瑞医药在多个治疗领域均具备显著竞争优势:1.抗肿瘤药物领域◦市场地位:国内抗肿瘤药市场领先企业,2025年抗肿瘤药收入占比52.71%◦代表产品:卡瑞利珠单抗(PD-1抑制剂),已获批9项适应症◦竞争优势:产品线丰富,覆盖多种靶点,如CDK4/6、PARP、TPO-R等2.神经科学领域◦市场地位:国内麻醉药市场领导者,市场份额22.3%◦代表产品:瑞马唑仑(GABAa受体激动剂),全球首仿产品◦竞争优势:七氟烷等产品占据国内主要市场份额,如七氟烷占国内吸入麻醉药市场62.5%3.造影剂领域◦市场地位:国内造影剂市场领先企业◦代表产品:碘佛醇(2024年上半年品牌市占率18.09%)、钆布醇(打破拜耳垄断)◦竞争优势:多款产品为国内首家过评,如钆布醇注射液4.代谢和心血管领域◦市场地位:2025年收入占比7.70%◦代表产品:恒格列净(SGLT2抑制剂),HRS9531(GLP-1/GIP双激动剂)◦竞争优势:HRS9531在III期临床试验中显示优异疗效,平均减重达19.2%五、未来发展战略与增长驱动因素5.1未来三年创新药管线规划恒瑞医药已形成清晰的创新产品上市节奏规划,预计未来三年将有大量创新成果获批:•2026年:预计12项创新产品及适应症获批上市◦代表产品:瑞拉芙普α(PD-L1/TGF-β双抗,用于胃癌一线治疗)、瑞康曲妥珠单抗(HER2ADC,用于乳腺癌二线治疗)•2027年:预计13项创新产品及适应症获批上市◦代表产品:HRS9531(GLP-1/GIP双激动剂,用于肥胖/超重治疗)•2028年:预计23项创新产品及适应症获批上市◦代表产品:多个代谢疾病、自免疾病领域的新药创新药销售目标:公司提出力争2026年创新药销售收入实现超过30%的增长,显著高于2025年的26.09%增速,彰显管理层对创新药商业化能力的信心。5.2国际化战略加速推进恒瑞医药的国际化战略已从"借船出海"向"自主出海"与"借船出海"双轮驱动转变,未来将进一步加速:1.自主国际化◦研发中心建设:2025年新增美国波士顿临床研发及合作中心,形成全球研发网络◦临床试验推进:多个创新药启动首项海外临床试验,如瑞康曲妥珠单抗联合阿得贝利和化疗用于胃癌或胃食管结合部腺癌获美国FDA孤儿药资格认定◦FDA审评推进:卡瑞利珠单抗联合阿帕替尼治疗肝癌的方案将于2026年7月在美国FDA审评,有望实现中国PD-1出海"零的突破"2.BD合作深化◦合作模式创新:从传统对外许可向NewCo模式、战略联盟等多元化模式转变◦与GSK合作:双方共同开发包括PDE3/4抑制剂HRS-9821在内的至多12款创新药,恒瑞获得5亿美元首付款,潜在总金额约120亿美元◦与MSD合作:就Lp(a)抑制剂HRS-5346达成大中华区外独家许可,获得2亿美元首付款及最高17.7亿美元里程碑付款3.海外生产基地布局◦美国市场:计划在美国建设生产基地,支持创新药在美国的商业化◦欧洲市场:在瑞士等地建立研发中心,支持欧洲市场拓展◦新兴市场:通过Glenmark等合作伙伴拓展东南亚、中东等新兴市场5.3核心增长驱动因素恒瑞医药未来三年的核心增长驱动因素主要来自以下方面:1.创新药放量◦已上市产品:瑞维鲁胺、达尔西利等医保内创新药持续放量◦新上市产品:2026-2028年预计53项创新产品及适应症获批,形成持续增长动力◦非肿瘤领域:恒格列净、瑞马唑仑等产品在非肿瘤领域增速高达73.36%,多元化布局成效显著2.创新药出海◦自主出海:卡瑞利珠单抗、瑞康曲妥珠单抗等产品有望实现海外商业化◦BD授权:与GSK、MSD等合作的BD项目将为公司带来持续收入◦Kailera上市:恒瑞持有Kailera13.6%股权,若其成功在纳斯达克上市,将为公司带来股权增值收益3.研发平台价值释放◦ADC平台:已有10余款差异化ADC分子进入临床,如瑞康曲妥珠单抗◦PROTAC平台:ARPROTAC抑制剂HRS-5041已获批开展Ib/II期临床试验◦AIDD平台:与华为云合作开发AI药物发现模型,年节约1/3以上翻译费用六、潜在风险分析尽管恒瑞医药发展前景良好,但仍面临以下潜在风险:6.1研发与商业化风险新药研发周期长、失败率高,是恒瑞医药面临的主要风险之一:1.研发失败风险◦新药从研制、临床试验到报批的周期长、环节多,通常需要10年以上时间◦近年来新药审评和监管政策不断收紧,国家对新药开发各阶段的审评标准不断提高◦为应对同质化竞争,公司采取创新靶点前移策略,但也面临更高的研发风险2.审批延迟风险◦审批过程中存在资料补充、审批流程变化等因素导致的审批周期延长风险◦部分产品如HRS9531尚未开展与已获批药物的头对头临床试验,可能影响审批速度◦卡瑞利珠单抗FDABLA重新递交后,审批结果存在不确定性3.商业化不及预期风险◦随着国内药品审评审批制度逐步与国际接轨,国外医药企业产品进入国内速度加快◦本土医药企业数量增多,医药产业同质化竞争加剧◦部分创新药如瑞卡西单抗虽在临床试验中显示良好疗效,但因未进医保,医院处方量仅占潜在需求的15%左右6.2集采政策风险集采政策常态化对仿制药业务构成持续压力:1.国内集采影响◦前9批国家组织药品集采中选的1600多个产品中,国产仿制药占比为96%◦集采导致仿制药价格平均降幅超50%,恒瑞医药2024年集采导致仿制药收入减少约8.44亿元◦仿制药业务收入占比虽逐年下降,但仍占总收入的41.66%,集采政策变化仍可能影响业绩2.海外集采风险◦2025年下半年国家拟开展第五批集采,涉及15个心血管及内分泌类药物,恒瑞多个核心品种可能再次被纳入◦海外市场如欧洲、美国等也逐步推行集采政策,可能影响创新药海外销售价格6.3BD合作不确定性BD合作虽为公司带来丰厚回报,但也存在不确定性:1.BD合作终止风险◦2026年3月,德国默克宣布终止与恒瑞医药的PARP1抑制剂合作,主因默克自身管线调整◦其他BD合作项目也可能因合作方战略调整而终止,导致里程碑付款无法实现2.BD收入波动风险◦BD收入主要来自首付款和里程碑付款,收入确认具有不确定性◦2025年BD收入33.92亿元,若未来BD交易减少或合作方付款延迟,可能影响业绩稳定性3.NewCo模式风险◦恒瑞通过NewCo模式与Kailera合作,虽降低了退货风险,但需承担合作方IPO失败或临床失败的连带风险◦Kailera2025年净亏损达1.49亿美元,若其IPO不成功,可能影响恒瑞的股权价值6.4海外市场竞争加剧恒瑞医药在海外市场的竞争将日益激烈:1.ADC赛道竞争◦恒瑞的ADC药物面临复星医药、信达生物等企业的同类产品竞争◦部分竞品已提前进入医保目录,可能挤压恒瑞的市场空间2.GLP-1赛道竞争◦国内已有信达生物玛仕度肽等产品获批,与恒瑞的HRS9531形成直接竞争◦国际市场上,礼来替尔泊肽已实现全球销售,2024年全球销售额达49.26亿美元◦恒瑞HRS9531虽在III期临床试验中显示良好疗效,但与已获批产品的头对头试验尚未开展,市场接受度存在不确定性3.海外法规风险◦海外市场药品注册审批标准严格,如美国FDA对创新药的审评要求不断提高◦海外生产基地建设需符合当地GMP标准,建设周期长、投资规模大,存在进度不及预期风险七、投资价值与估值分析7.1创新药龙头地位确立恒瑞医药已成功确立其在中国创新药领域的龙头地位:•研发投入领先:2025年研发费用87.24亿元,占营收27.58%,远高于行业平均水平•管线深度领先:自研管线数量达128-138项,位居全球第二,覆盖肿瘤、代谢、自免、神经科学等多个高潜力领域•创新药收入领先:2025年创新药销售收入163.42亿元,同比增长26.09%,占药品销售收入的比重达58.34%•国际化布局领先:与GSK、MSD等跨国药企达成多项BD合作,潜在交易总额超270亿美元7.2估值分析根据多家券商机构的研报,恒瑞医药2026年的估值水平如下:•高盛:目标价72.8元,预计2026年归母净利润89亿元,对应PE约37倍•中信证券:目标价72.3元,预计2026年归母净利润90亿元,对应PE约41倍•国信证券:目标价70.2元,预计2026年归母净利润87亿元,对应PE约39倍•国金证券:目标价73.5元,预计2026年归母净利润93亿元,对应PE约38倍估值合理性分析:恒瑞医药的估值水平略高于行业平均水平,但考虑到其创新药龙头地位、丰富的研发管线和国际化战略的推进,当前估值具备一定合理性。7.3投资建议长期投资价值显著:恒瑞医药已从"中国的恒瑞"向"世界的恒瑞"稳步转型,创新药业务占比持续提升,研发投入强度行业领先,国际化布局日益完善,长期投资价值显著。短期关注点:•2026年创新药销售收入增速能否达到30%以上•瑞康曲妥珠单抗、HRS9531等核心产品的商业化进展•卡瑞利珠单抗FDABLA审评结果•Kailera纳斯达克IPO进展及恒瑞股权价值变化风险控制建议:•关注集采政策变化对仿制药业务的影响•跟踪BD合作项目的里程碑付款确认情况•关注创新药临床试验数据及审批进展•评估海外市场竞争加剧对公司产品定价的影响八、结论恒瑞医药作为中国医药行业的领军企业,已成功实现从仿制药向创新药的战略转型,2025年创新药销售收入占比达58.34%,成为业绩增长的核心驱动力。公司通过"科技创新+国际化"双轮驱动战略,持续提升研发投入,已形成全球领先的创新管线布局,自研管线数量位居全球第二,并与GSK、MSD等跨国药企达成多项BD合作,潜在交易总额超270亿美元。在财务表现方面,公司2025年实现营业收入316.29亿元,同比增长13.02%;归母净利润77.11亿元,同比增长21.69%,经营现金流显著改善至112.35亿元,同比增长51.36%。公司资产负债结构持续优化,总资产698.67亿元,同比增长39.36%;归属于上市公司股东的净资产612.72亿元,同比增长34.61%,为公司长期发展奠定了坚实基础。未来三年,恒瑞医药预计有约53项创新产品及适应症获批上市,有望为业绩增长提供持续动能。公司将进一步加速国际化战略,通过自主出海与BD授权双轮驱动,推动创新药的全球价值兑现。同时,公司也将继续优化业务结构,集中资源发展创新药业务,战略性收缩对仿制药的投入。
财报临床3期上市批准引进/卖出
2026-03-30
·今日头条
恒瑞医药2025年业绩实现"双创新高",营收316.29亿元(+13.02%),净利润77.11亿元(+21.69%),
创新药收入占比首次超过50%
,标志着公司已完成从仿制药巨头到创新药领军企业的战略转型。
公司研发投入87.24亿元(占营收27.58%),增速放缓至6.03%,但管线推进效率显著提升,2026-2028年预计有53项创新成果获批,为未来3年业绩高增长奠定基础。非肿瘤业务(31.02亿元,+73.36%)增速远超肿瘤业务,GLP-1/GIP双靶点药物HRS9531、全氟己基辛烷滴眼液等创新产品商业化加速,成为公司第二增长曲线。
国际化战略全面提速
,与GSK合作的HRS-9821潜在交易金额达120亿美元,自2023年以来累计达成12笔BD交易,潜在总交易价值超270亿美元,国际化正成为公司业绩增长的新引擎。恒瑞医药已构建"全球资源整合+本地效率优化"的研发模式,研发团队超5,600人,海外占比约15%,技术平台覆盖ADC、双抗、PROTAC等前沿领域,具备与国际巨头竞争的实力。
展望未来,公司有望通过创新药密集获批和国际化合作深化,实现从"中国龙头"向"全球创新药企"的跨越式发展。
01 基本财务数据:营收净利双创新高,创新药占比首次过半
恒瑞医药2025年业绩实现"双创新高",全年营业收入达316.29亿元,同比增长13.02%;
归属于上市公司股东的净利润为77.11亿元,同比增21.69%;
扣非净利润74.13亿元,同比增长20.00%。
净利润增速显著高于营收增速
,主要得益于创新药占比提升带动整体毛利率优化,以及公司精细化管控下费用率保持相对稳定,规模效应逐步显现。
2025年,恒瑞医药整体毛利率为86.21%,同比下降0.04个百分点,医药制造业毛利率为85.06%,与上年基本持平。
期间费用率为58.39%
,较上年同期下降2.01个百分点,其中: 销售费用率:28.79%(同比下降0.93个百分点),增速9.24%低于营收增速,反映销售费用管控成效显著;管理费用率:8.87%(同比下降0.96个百分点);研发费用率:22.01%(同比下降0.12个百分点)。
2025年,恒瑞医药经营活动产生的现金流净额为112.35亿元,同比增长51.36%;筹资现金流同比增长601.85%,主要因公司于2025年11月成功登陆港交所实现"A+H"上市,募集资金113.74亿港元(约100亿元人民币),成为近5年港股医药板块最大IPO。截至2025年末,公司账面货币资金达409.55亿元,较去年同期增加六成,为公司创新药研发和国际化布局提供了充足资金保障。
恒瑞医药已完成收入结构的根本重塑:仿制药占比从75%(2020年)降至48%(2024年),2025年进一步下降,创新药占比则从不足25%(2020年)升至58.34%(2025年),
创新药销售收入已占药品销售收入的绝对主力
。这一转型是双重驱动的结果:一方面集采政策倒逼,仿制药平均降价超50%,传统盈利模式难以为继;另一方面是临床需求拉动,肿瘤、自身免疫等领域的未满足需求为创新药打开了市场空间。
2025年,恒瑞医药BD合作模式持续创新,共达成5笔创新药海外业务拓展交易,对外许可收入达33.92亿元,同比增长25.62%。其中与GSK达成的战略合作尤为瞩目:双方共同开发包括PDE3/4抑制剂HRS-9821在内的至多12款创新药,恒瑞获得5亿美元首付款,潜在总金额约120亿美元的选择权行使费和里程碑付款及相应的销售提成。自2023年以来,恒瑞医药已完成12笔海外业务拓展交易,潜在总交易价值超过270亿美元,授权对象包括葛兰素史克、默克、默沙东等跨国药企。
2025年,恒瑞医药研发管线显著进展,共有15项上市申请获NMPA受理,28项临床推进至关键III期,61项进入II期,并有28项创新产品首次推进至临床I期。全年取得药物临床批件180个,获得8项CDE突破性治疗品种认定与2项优先审评品种认定。在临床开发环节,公司成功招募了超过22,000名临床试验参与者,展现出强大的临床开发执行力。
创新药矩阵梯度清晰
:目前公司已在中国获批上市24款1类创新药、5款2类新药,另有100多个自主创新产品正在临床开发,400余项临床试验在国内外开展。在创新药销售收入中,抗肿瘤产品收入132.40亿元,同比增长18.52%,占整体创新药销售收入的81.02%;非肿瘤产品实现收入31.02亿元,同比增长73.36%,占整体创新药销售收入的18.98%。
医保准入与国际化。
2025年,恒瑞医药共有20款产品/适应症通过新版国家医保目录调整,其中10款产品首次进入医保,5款产品新增适应症进入医保,5款产品完成目录内续约,覆盖肿瘤、代谢、心血管、自身免疫、眼科等多个疾病领域。同时,公司国际化进程迈出了实质性一步,成功登陆港交所实现"A+H"上市,海外业务拓展、研发合作与机构建设同步推进。
02 研发投入情况:高强度投入延续,资本化率维持低位,研发效率显著提升
研发投入规模与占比
恒瑞医药2025年全年累计研发投入87.24亿元,占营业收入的27.58%,研发投入强度仍位居国内医药企业前列。其中费用化研发投入69.61亿元,资本化研发投入17.63亿元。
研发投入增速与营收增速比较
2025年,恒瑞医药研发投入总额同比增长6.03%,其中费用化研发投入同比增长5.75%,研发投入增速首次低于营收增速(13.02%),
研发投入增速与营收增速的差值扩大至7个百分点
,表明公司研发策略从"高投入换管线"转向"投入效率优化+商业化反哺研发"的新阶段。
研发投入资本化政策
恒瑞医药自2021年11月起调整研发支出资本化政策,将研发费用从全部费用化变更为根据研发项目所处的不同阶段区别对待:研发阶段的支出(即进入III期临床试验前的所有支出)仍于发生时计入当期损益;而开发阶段的支出(即进入III期临床试验后的支出)则计入开发支出,并在开发项目达到预定用途时结转为无形资产。
恒瑞医药的资本化率维持在20.21%的相对保守水平
,低于百济神州(35%)、信达生物(30%)等纯创新药企,高于复星医药(12%)等综合药企。这一比例处于行业合理区间,与公司"进入III期临床试验后开始资本化"的时点选择相匹配,且80%的资本化项目为III期及NDA阶段,完全符合会计准则对资本化的要求。
研发团队与全球布局
截至2025年,恒瑞医药全球研发团队超5,600人,其中海外团队占比约15%,涵盖来自罗氏、辉瑞等国际巨头的资深科学家。公司在中国、美国、日本、澳大利亚及瑞士等14个国家和地区设立14个研发中心,2025年新增美国波士顿临床研发及合作中心,形成"全球资源整合+本地效率优化"的研发模式。
技术平台建设
恒瑞医药已建立成熟的多项技术平台,包括:ADC(抗体偶联药物):瑞康曲妥珠单抗(HER2 ADC)于2025年5月获批用于HER2突变NSCLC,III期临床试验显示ORR达74.5%,mPFS为11.5个月,疗效显著;双/多抗:SHR-1701(PD-L1/TGF-β双抗)针对胃癌适应症的全球III期临床试验持续推进;蛋白质降解剂:PROTAC平台持续推进,如HRS-5041(AR PROTAC抑制剂)于2025年10月获批开展Ib/II期临床试验;小核酸药物、口服多肽等。
此外,恒瑞医药大力发展人工智能药物发现(AIDD),与华为云合作开发的"AI翻译与eTMF分档分类质控模型"已落地,年节约1/3以上翻译费用,翻译周期从数周缩短至数小时。2025年,公司还与英矽智能等AI药物研发公司展开合作,加速分子筛选与药物发现进程。
研发投入产出效率
恒瑞医药研发投入产出效率持续提升,2025年共有7款1类创新药、1款2类创新药获批上市,6个已获批创新药的新适应症获批。
公司已累计获批上市24款1类创新药
,创新药年度营收163.42亿元,药均营收9.6亿元,同比增长约10%。同时,公司研发管线推进高效,28项临床推进至III期,61项进入II期,28项创新产品首次推进至临床I期。
资本结构与研发投入保障
截至2025年末,恒瑞医药账面货币资金达409.55亿元,较去年同期增加六成。公司解释现金分红比例(17.20%)低于30%的原因时指出,公司正处于仿制药向创新药转型的关键阶段,需大量资金投入国内外临床试验及创新药研发;同时,公司在广东、北京、天津等地进行厂区的新扩建,以及计划通过加大与国际研发机构合作,储备更多创新药品种以增强全球竞争力,均需较高资金支持。
公司现金储备充足,可覆盖约4.7年研发投入
(按年均17.3亿元计算),为公司长期创新转型提供了坚实保障。
03 非肿瘤业务发展情况:高增长开启第二曲线,GLP-1/GIP双靶点药物HRS9531即将上市
非肿瘤业务整体表现
2025年,恒瑞医药非肿瘤业务实现收入31.02亿元,同比增长73.36%,增速显著高于肿瘤业务(18.52%),占创新药销售收入的18.98%。
非肿瘤业务已成为公司增长的新引擎
,标志着公司从单一肿瘤领域向多元化治疗领域拓展的战略初见成效。
三大非肿瘤业务板块分析
(1) 麻醉业务
麻醉业务是恒瑞医药非肿瘤业务中成熟度最高的板块,核心产品为瑞马唑仑(GABAa受体激动剂)。
产品表现
:瑞马唑仑2025年销售额约18亿元(假设年销量120万支,单价150元/支),同比增长近40%。该产品已获批适应症包括"非气管插管的手术/操作中的镇静和麻醉"以及"全身麻醉诱导与维持",2025年8月新增适应症"作为镇静药物用于重症监护期间机械通气时的镇静"。
竞争优势
:恒瑞医药在麻醉领域市占率长期领先,瑞马唑仑作为超短效GABAa受体激动剂,具有起效快、代谢快、苏醒快且恢复质量高等独特优势,已在全身麻醉诱导与维持领域建立领先地位。
市场空间
:2024年中国公立医疗机构终端神经系统药物(化+生)销售规模超过900亿元,恒瑞医药凭借麻醉领域的创新药布局,有望进一步扩大市场份额。
(2) 眼科药物
眼科药物是恒瑞医药非肿瘤业务中增长最快的板块,核心产品为全氟己基辛烷滴眼液(商品名:恒沁)。
产品表现
:恒沁全氟己基辛烷滴眼液于2025年7月获批上市,用于治疗睑板腺功能障碍(MGD)相关干眼。该产品在京东健康线上首发,零售价468元/盒(3ml*1支),上线3个多月销量突破5000盒,跻身"眼干涩"药品热卖榜第8。2025年12月,恒沁纳入2026年医保目录,降价至190元/盒,预计2026年公立医院端销量将爆发,销售额有望破亿。
技术优势
:恒沁是目前全球唯一一款用于治疗MGD相关干眼的药品,基于无水药物递送技术平台EyeSol研发,由单一组分全氟己基辛烷(F6H8)组成,不含油脂、表面活性剂和防腐剂等赋形剂,拥有极低的表面张力,可迅速扩散至眼表面,改善脂质层等级,抑制泪液蒸发,促进角膜上皮修复。
市场空间
:据《中国干眼临床诊疗指南(2023年)》,我国干眼的发病率为21%-30%,约69%-86%的干眼人群患有MGD。2025年MGD相关干眼治疗市场规模约33-41亿元,恒沁作为唯一获批药物,渗透率提升空间大。
(3) 代谢性疾病药物
代谢性疾病药物是恒瑞医药非肿瘤业务中最具潜力的板块,核心产品为恒格列净(SGLT2抑制剂)和HRS9531(GLP-1/GIP双受体激动剂)。
产品表现
:恒格列净2025年收入约10亿元,同比增长超60%,主要用于糖尿病和慢性肾病治疗。HRS9531注射液(GLP-1/GIP双受体激动剂)治疗中国肥胖或超重受试者的III期临床试验(HRS9531-301)于2025年7月15日获得积极顶线结果,与安慰剂相比,6mg剂量组平均体重降低19.2%(安慰剂调整后为17.7%),体重降低≥5%的受试者比例达85.7%。恒瑞医药已向中国国家药监局提交用于长期体重管理的新药上市申请(NDA),预计2026年Q2获批。
技术优势
:HRS9531注射液在III期临床试验中显示出良好的安全性和耐受性,大多数治疗期间出现的不良事件为轻度至中度,主要为胃肠道相关事件,无严重不良事件。该药物同时激活GLP-1和GIP受体,通过协同作用实现减重疗效与药物安全性的平衡。
市场空间
:中国肥胖人群已超50.7%,若不干预,到2030年成年人超重肥胖率可能升至70.5%,市场规模或超500亿元。HRS9531若能在国内获批,有望成为公司首个年销售额超10亿元的非肿瘤创新药。
3. 非肿瘤业务增长驱动因素
非肿瘤业务高增长的主要驱动因素包括:
产品管线丰富
:公司在代谢、麻醉、心血管等领域布局了多款创新药,形成了差异化的产品矩阵。
医保覆盖扩大
:恒沁等创新药纳入医保后价格大幅下降(如恒沁从468元/盒降至190元/盒),显著提高了可及性与患者支付意愿。
渠道优势
:公司商业化网络覆盖中国30多个省级行政区的超过25,000家医院及超过200,000家线下零售药店,强大的销售团队为新产品快速放量提供了保障。
临床价值凸显
:非肿瘤创新药针对未被满足的临床需求,如恒沁填补了国内MGD相关干眼治疗药物的空白。
4. 非肿瘤业务未来增长点
非肿瘤业务未来增长点主要包括:
GLP-1/GIP双靶点药物HRS9531
:2026年Q2有望获批肥胖适应症,随后可能拓展至2型糖尿病、慢性肾脏病等适应症,预计峰值销售额可达50-70亿元。
口服GLP-1药物HRS-7535
:已进入III期临床试验,作为HRS9531的补充,覆盖不能接受注射的患者群体。
PDE3/4抑制剂HRS-9821
:与GSK合作开发,潜在交易金额达120亿美元,虽处于临床开发阶段,但已显示出强效的PDE3和PDE4抑制作用,有望成为COPD治疗领域的重磅药物。
其他代谢药物
:如GLP-1/GIP/GCGR三重受体激动剂等,针对代谢相关脂肪性肝病(MASLD)等疾病领域。
5. 非肿瘤业务挑战与风险
非肿瘤业务面临的挑战与风险包括:
GLP-1赛道竞争加剧
:诺和诺德、礼来等国际巨头已在国内布局GLP-1药物,HRS9531需在减重效果与安全性方面建立差异化优势。
医保谈判压力
:随着更多创新药纳入医保,价格可能进一步下降,需通过规模化生产与成本控制维持盈利能力。
适应症拓展难度
:如HRS9531的慢性肾脏病适应症需与已获批的SGLT2抑制剂竞争,需证明其在心血管保护方面的独特优势。
04 未来展望:创新药密集获批,国际化战略提速,从"中国龙头"向"全球创新药企"跃迁
1. 短期增长引擎(2026-2027年)
恒瑞医药已明确提出力争2026年创新药销售收入实现超过30%增长的目标,这一目标在163.42亿元的高基数上实现,需要新增约50亿元的创新药收入。
这一增量有望通过以下产品实现
:
HRS9531肥胖适应症
:2026年Q2有望获批,假设首年市占率10%,销售额可达15-20亿元;若减重效果显著,市占率可能进一步提升。
瑞康曲妥珠单抗新适应症
:HER2阳性结直肠癌、乳腺癌一线治疗适应症获批后,销售有望从2025年约15亿元增至2027年30亿元+。
恒格列净放量
:用于糖尿病和慢性肾病治疗,2025年收入约10亿元,2026年有望突破15亿元。
BD授权收益
:GSK合作5亿美元首付款已确认,后续里程碑付款(如HRS-9821 III期成功、上市)将贡献现金流。
其他非肿瘤创新药
:如瑞马唑仑新适应症放量、全氟己基辛烷滴眼液医保后公立医院端销量爆发等。
2. 中长期战略(2028年后)
恒瑞医药的中长期战略主要包括:
管线深度拓展
:2026-2028年预计有53项创新成果获批上市,其中代谢、肿瘤、呼吸等领域是核心增长点。公司已建立成熟的PROTAC、双/多抗、小核酸药物等前沿技术平台,有望诞生FIC(First-in-Class)或BIC(Best-in-Class)药物,提升国际竞争力。
全球化布局深化
:美国波士顿研发中心落地后,海外临床试验效率提升,如瑞康曲妥珠单抗胃癌适应症FDA孤儿药资格可缩短审批周期。同时,与MSD、GSK等国际巨头的合作将加速创新药进入欧美市场。
创新药国际化
:恒瑞医药已与GSK、MSD等多家跨国药企达成战略合作,潜在交易价值超270亿美元。如HRS-9821与GSK合作潜在价值120亿美元,HRS-5346与MSD合作潜在价值19.7亿美元,这些合作将为公司带来稳定的国际化收入。
创新药出海模式升级
:从早期单一的权益授权,向多元化、高阶化方向发展,包括"自主出海"开展全球多中心临床、与国际巨头开展"联合开发"、借助设立合资公司(JV/Co-Co)达成"资本+技术+市场"的生态融合等模式。
3. 创新药管线国际竞争力分析
恒瑞医药创新药管线的国际竞争力主要体现在以下方面:
技术平台领先
:公司已建立成熟的ADC、双/多抗、蛋白降解剂等技术平台,技术实力获国际认可。如瑞康曲妥珠单抗(HER2 ADC)获FDA快速通道资格认定,HLX43(PD-L1 ADC)获FDA孤儿药资格认定,显示其在ADC领域的全球竞争力。
临床研究质量高
:2025年,公司共有381项重要研究成果获得国际认可,在CA(临床医师癌症杂志)、The Lancet(柳叶刀)、JAMA(美国医学会杂志)等全球顶级期刊发表,累计影响因子达3,159分,其中18篇为重磅研究论文(肿瘤领域影响因子≥30分、非肿瘤领域影响因子≥20分的国际期刊)。
国际化人才团队
:公司聘请多名具备国际医药行业从业经验的管理人员,包括冯佶(总裁)、朱国新(高级副总裁、全球早研负责人)、Yu Liu(国际首席医学官)、Karen Atkin(国际商业和组合策略负责人)等,构建了全球化的组织能力。
BD合作模式创新
:与GSK的合作模式为"联合开发+选择权",恒瑞主导I期临床后由GSK负责全球开发,降低了出海风险并加速商业化。类似模式还应用于其他管线,如HRS-1893以NewCo模式授权Braveheart Bio。
4. 创新药管线未来增长预测
根据公司年报披露,2026-2028年预计有53项创新成果获批上市,其中:
2026年
:预计获批上市创新药及适应症12项,包括HRS9531肥胖适应症、瑞康曲妥珠单抗新适应症等。
2027年
:预计获批上市创新药及适应症22项,包括口服GLP-1药物HRS-7535、双抗药物SHR-1701等。
2028年
:预计获批上市创新药及适应症19项,包括PROTAC药物HRS-5041、小核酸药物等前沿领域产品。
若53项创新成果顺利获批并商业化,预计到2028年创新药收入可达250-300亿元,年复合增长率(CAGR)约25-30%
。
恒瑞医药已构建"全球资源整合+本地效率优化"的研发模式
,研发团队超5,600人,海外占比约15%,技术平台覆盖ADC、双抗、PROTAC等前沿领域,具备与国际巨头竞争的实力。展望未来,公司有望通过创新药密集获批和国际化合作深化,实现从"中国龙头"向"全球创新药企"的跨越式发展。
05 结论:创新转型成功落地,国际化战略加速推进,估值修复空间可期
恒瑞医药2025年年报显示,公司已完成从仿制药巨头到创新药领军企业的战略转型,创新药收入占比首次超过50%。
研发投入增速首次低于营收增速
,表明公司研发策略从"高投入换管线"转向"投入效率优化+商业化反哺研发"的新阶段。非肿瘤业务(31.02亿元,+73.36%)增速远超肿瘤业务,GLP-1/GIP双靶点药物HRS9531、全氟己基辛烷滴眼液等创新产品商业化加速,成为公司第二增长曲线。
国际化战略全面提速,与GSK合作的HRS-9821潜在交易金额达120亿美元,自2023年以来累计达成12笔BD交易,潜在总交易价值超270亿美元,国际化正成为公司业绩增长的新引擎。公司现金储备充足(409.55亿元),可覆盖约4.7年研发投入,为长期创新转型提供了坚实保障。
展望未来,恒瑞医药有望通过创新药密集获批和国际化合作深化,实现从"中国龙头"向"全球创新药企"的跨越式发展。
公司已构建"全球资源整合+本地效率优化"的研发模式
,研发团队超5,600人,海外占比约15%,技术平台覆盖ADC、双抗、PROTAC等前沿领域,具备与国际巨头竞争的实力。若53项创新成果顺利获批并商业化,预计到2028年创新药收入可达250-300亿元,年复合增长率(CAGR)约25-30%。
尽管面临集采压力、BD合作不确定性、GLP-1赛道竞争白热化等风险,但恒瑞医药凭借强大的研发实力、丰富的管线储备和成功的国际化战略,已具备穿越行业周期的能力。
财报抗体药物偶联物IPO蛋白降解靶向嵌合体
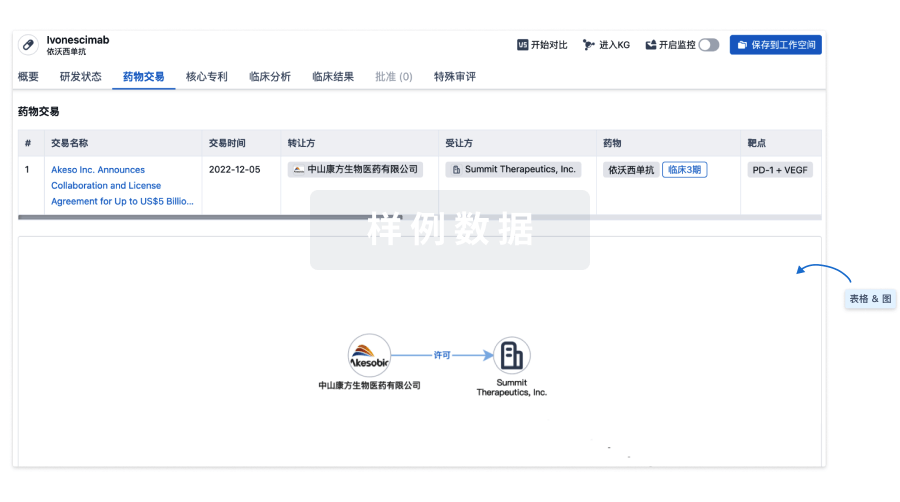
100 项与 GABAA受体激动剂(天地恒一制药) 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 中枢神经系统疾病 | 药物发现 | 中国 | 2021-01-28 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
| 研究 | 分期 | 人群特征 | 评价人数 | 分组 | 结果 | 评价 | 发布日期 |
|---|
No Data | |||||||
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
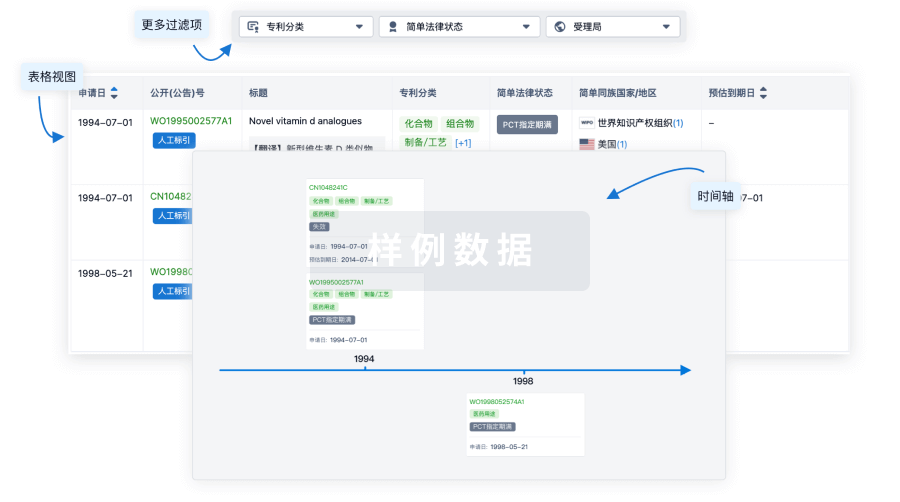
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
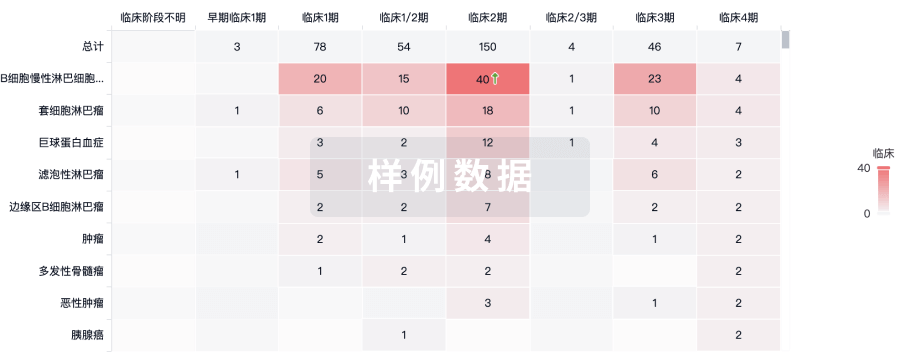
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用