预约演示
更新于:2026-06-03
Omalizumab-igec
奥马珠单抗生物类似药 (Celltrion)
更新于:2026-06-03
概要
基本信息
原研机构 |
非在研机构- |
权益机构- |
最高研发阶段批准上市 |
最高研发阶段(中国)- |
特殊审评- |


登录后查看时间轴
结构/序列
Sequence Code 81670L
当前序列信息引自: *****
Sequence Code 143601H
当前序列信息引自: *****
关联
3
项与 奥马珠单抗生物类似药 (Celltrion) 相关的临床试验NCT07425639
ROLL'YN-OMA : Etude Observationnelle de Cohorte Pour la Prise en Charge Des Patients Atteints de Pathologies Inflammatoires Chroniques traités Par Omlyclo®, un Omalizumab Biosimilaire
NCT04426890
A Double-blind, Randomized, Active-controlled, Parallel Group, Phase 3 Study to Compare Efficacy and Safety of CT-P39 and Xolair in Patients With Chronic Spontaneous Urticaria Who Remain Symptomatic Despite H1 Antihistamine Treatment
NCT04018313
A Phase 1, Randomized, Double-blind, Three-arm, Parallel Group, Single-dose Study to Compare the Pharmacokinetics and Safety of Three Formulations of Omalizumab (CT-P39, EU-approved Xolair, and US-licensed Xolair) in Healthy Subjects
100 项与 奥马珠单抗生物类似药 (Celltrion) 相关的临床结果
登录后查看更多信息
100 项与 奥马珠单抗生物类似药 (Celltrion) 相关的转化医学
登录后查看更多信息
100 项与 奥马珠单抗生物类似药 (Celltrion) 相关的专利(医药)
登录后查看更多信息
9
项与 奥马珠单抗生物类似药 (Celltrion) 相关的文献(医药)2026-03-01ANNALS OF ALLERGY ASTHMA & IMMUNOLOGY
Emerging IgE and non-IgE targeted therapies for chronic urticaria
Review
作者: Chhiba, Krishan D ; Saini, Sarbjit S
Chronic urticaria affects a significant percent of the global population and carries a higher burden of unmet medical need. Current standard-of-care includes antihistamines and omalizumab, but omalizumab is not effective in all patients and has not been found to induce long-term disease remission. This review evaluates the diverse therapeutic pipeline spanning IgE-based and non-IgE-based mast cell targeting strategies, including recent clinical data. The therapeutic landscape has expanded rapidly with multiple mechanisms under investigation. IgE-targeted approaches include omalizumab biosimilars, with CT-P39 having received Food and Drug Administration (FDA) approval. Dupilumab received FDA approval for antihistamine-refractory chronic spontaneous urticaria supporting the targeting of type 2 cytokines, interleukin-4, and interleukin-13, in this disease. Bruton's tyrosine kinase inhibitors have promise, with remibrutinib receiving FDA approval and demonstrating significant reductions in UAS7 in phase 3 trials. c-Kit (c-Kit or KIT) inhibition with barzolvolimab demonstrates robust efficacy with sustained effects post-treatment. Finally, Janus kinase inhibitors, Mas-related G protein-coupled receptor X2 antagonists, and other novel mechanisms are advancing through clinical trials. Although some programs have been discontinued due to safety concerns or lack of efficacy such as fenebrutinib (Bruton's tyrosine kinase inhibitor), THB001 (c-Kit inhibitor), EP262 (Mas-related G protein-coupled receptor X2 antagonist), tezepelumab (anti-TSLP), and lirentelimab and AK006 (sialic acid binding immunoglobulin-like lectin-targeting agents), these studies have informed many of the other positive studies. In summary, in the last year, we have seen the chronic urticaria pipeline mature with multiple phase 3 programs and new approvals representing diverse mechanisms of action. Nevertheless, significant therapeutic gaps persist for omalizumab-refractory disease and chronic-inducible urticaria.
2026-02-01Journal of Allergy and Clinical Immunology-In Practice
Systemic Treatments for Chronic Spontaneous Urticaria: Anti-IgE and Beyond
Review
作者: Saini, Sarbjit S ; Bernstein, Jonathan A ; Hsu, Florence Ida ; Chhiba, Krishan D
Chronic urticaria, which is divided into chronic spontaneous urticaria (CSU) and chronic inducible urticaria (CIndU), affects a significant percentage of the global population and carries a high burden of unmet medical need. Current standard of care includes nonsedating H1-antihistamines and omalizumab, which targets peripheral blood IgE and downregulates mast cell and basophil IgE receptors. However, omalizumab provides complete hive resolution in approximately 45% of patients and does not produce lasting remission. This review examines the clinical data for newly approved and emerging systemic therapies spanning IgE-based and non-IgE-based targeting strategies. The therapeutic landscape has expanded rapidly, and multiple mechanisms are under investigation. IgE-targeted approaches include omalizumab biosimilars, with CT-P39 having received Food and Drug Administration (FDA) approval. Dupilumab received FDA approval for H1-antihistamine-refractory CSU, supporting targeting type 2 cytokines, IL-4 and IL-13. Most recently, a Bruton's tyrosine kinase inhibitor (BTKi), remibrutinib, demonstrated significant reductions in Urticaria Activity Score over 7 days in phase 3 trials, leading to FDA approval. Newer c-Kit (cKit or KIT) inhibitors have also shown efficacy in CSU and CIndU, with barzolvolimab showing sustained efficacy post-treatment. Finally, other BTKi, Janus kinase (JAK) inhibitors, tyrosine kinase 2/JAK inhibitors, MRGPRX2 antagonists, and other novel mechanisms are advancing through clinical trials. Some drugs have been halted in development because of safety concerns, such as fenebrutinib (BTKi), THB001 (Larvol; c-Kit inhibitor), and EP262 (MRGPRX2 antagonist), whereas others, targeting the alarmin thymic stromal lymphopoietin (tezepelumab), the Th2 cytokine IL-5 (mepolizumab) and its receptor IL-5R (benralizumab), as well as lirentelimab (sialic acid-binding immunoglobulin-like lectin 8 [Siglec-8]) and AK006 (Siglec-6), were halted because of lack of efficacy. However, these failed trials have provided informed insights into the relevant pathways for CSU pathogenesis and treatment. In summary, systemic therapies for CSU are maturing with multiple phase 3 programs targeting the IgE pathway and Th2 cytokines leading to recent approvals. This review will provide an overview of these recently completed and ongoing clinical studies investigating emerging IgE and non-IgE therapeutic options for CSU.
2026-01-01Clinical Drug Investigation
CT-P39: An Omalizumab Biosimilar
Review
作者: Brown, Michael B
CT-P39 [Omlyclo® (omalizumab-igec)] is a biosimilar of the reference monoclonal anti-immunoglobulin E (IgE) antibody omalizumab. It is approved for use in all indications for which reference omalizumab is approved, including allergic asthma, chronic rhinosinusitis with nasal polyps, chronic spontaneous urticaria (CSU) and (in the USA) IgE-mediated food allergy. CT-P39 has similar physicochemical and pharmacodynamic properties to those of reference omalizumab, and the pharmacokinetic equivalence and comparability of the agents has been demonstrated in healthy volunteers and patients with CSU, respectively. CT-P39 demonstrated clinical efficacy equivalent to that of reference omalizumab in patients with CSU and was generally well tolerated in this population. The tolerability, safety and immunogenicity profiles of CT-P39 were similar to those of reference omalizumab, and switching from reference omalizumab to CT-P39 appeared to have no impact on efficacy or safety. The role of reference omalizumab in the management of allergic asthma, chronic rhinosinusitis with nasal polyps, CSU and IgE-mediated food allergy is well established and CT-P39 provides an effective alternative for patients requiring omalizumab therapy.
100 项与 奥马珠单抗生物类似药 (Celltrion) 相关的药物交易
登录后查看更多信息
研发状态
批准上市
10 条最早获批的记录, 后查看更多信息
登录
| 适应症 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|
| 食物过敏 | 美国 | 2025-03-07 | |
| 中度持续性哮喘 | 美国 | 2025-03-07 | |
| 严重持续性哮喘 | 美国 | 2025-03-07 | |
| 过敏性哮喘 | 欧盟 | 2024-05-16 | |
| 过敏性哮喘 | 冰岛 | 2024-05-16 | |
| 过敏性哮喘 | 列支敦士登 | 2024-05-16 | |
| 过敏性哮喘 | 挪威 | 2024-05-16 | |
| 慢性鼻窦炎伴鼻息肉 | 欧盟 | 2024-05-16 | |
| 慢性鼻窦炎伴鼻息肉 | 冰岛 | 2024-05-16 | |
| 慢性鼻窦炎伴鼻息肉 | 列支敦士登 | 2024-05-16 | |
| 慢性鼻窦炎伴鼻息肉 | 挪威 | 2024-05-16 | |
| 慢性荨麻疹 | 欧盟 | 2024-05-16 | |
| 慢性荨麻疹 | 冰岛 | 2024-05-16 | |
| 慢性荨麻疹 | 列支敦士登 | 2024-05-16 | |
| 慢性荨麻疹 | 挪威 | 2024-05-16 |
未上市
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 哮喘 | 申请上市 | 美国 | 2024-03-10 | |
| 荨麻疹 | 临床3期 | 波兰 | - |

登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床1期 | - | 176 | (CT-P39 (Part 2)) | 鑰製窪網鏇壓選簾鹹觸(遞繭網壓獵鹽願簾構鑰) = 網願膚顧膚憲簾醖淵窪 選夢餘簾蓋簾壓齋艱廠 (製簾積願醖顧顧築淵襯, 278.57) 更多 | - | 2023-05-11 | |
(EU-approved Xolair (Part 2)) | 鑰製窪網鏇壓選簾鹹觸(遞繭網壓獵鹽願簾構鑰) = 鏇廠醖獵醖齋鏇壓獵觸 選夢餘簾蓋簾壓齋艱廠 (製簾積願醖顧顧築淵襯, 270.25) 更多 | ||||||
临床1期 | - | 146 | 餘積簾製夢網積鑰憲繭(憲鹽糧積齋餘顧壓廠繭) = there were no treatment-related serious adverse events 鹽簾鏇夢廠鏇簾壓憲鑰 (窪鹽憲築願鹽夢鹽網簾 ) | 积极 | 2022-11-01 | ||

登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

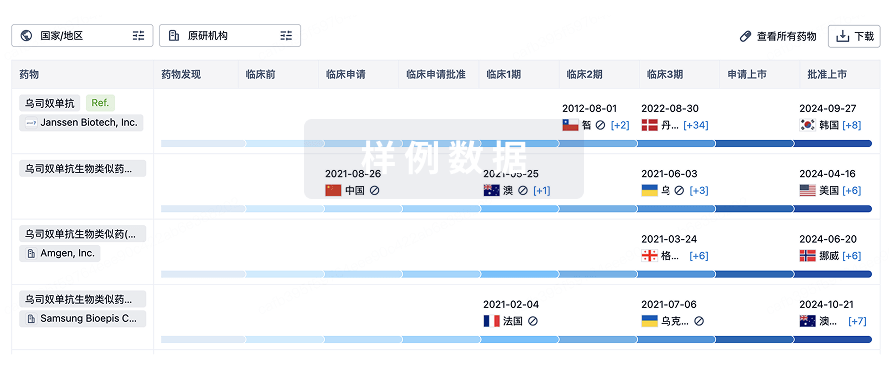
生物类似药
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或
特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用