预约演示
更新于:2026-03-17
DV-281
更新于:2026-03-17
概要
基本信息
在研机构- |
权益机构- |
最高研发阶段无进展临床1期 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |

登录后查看时间轴
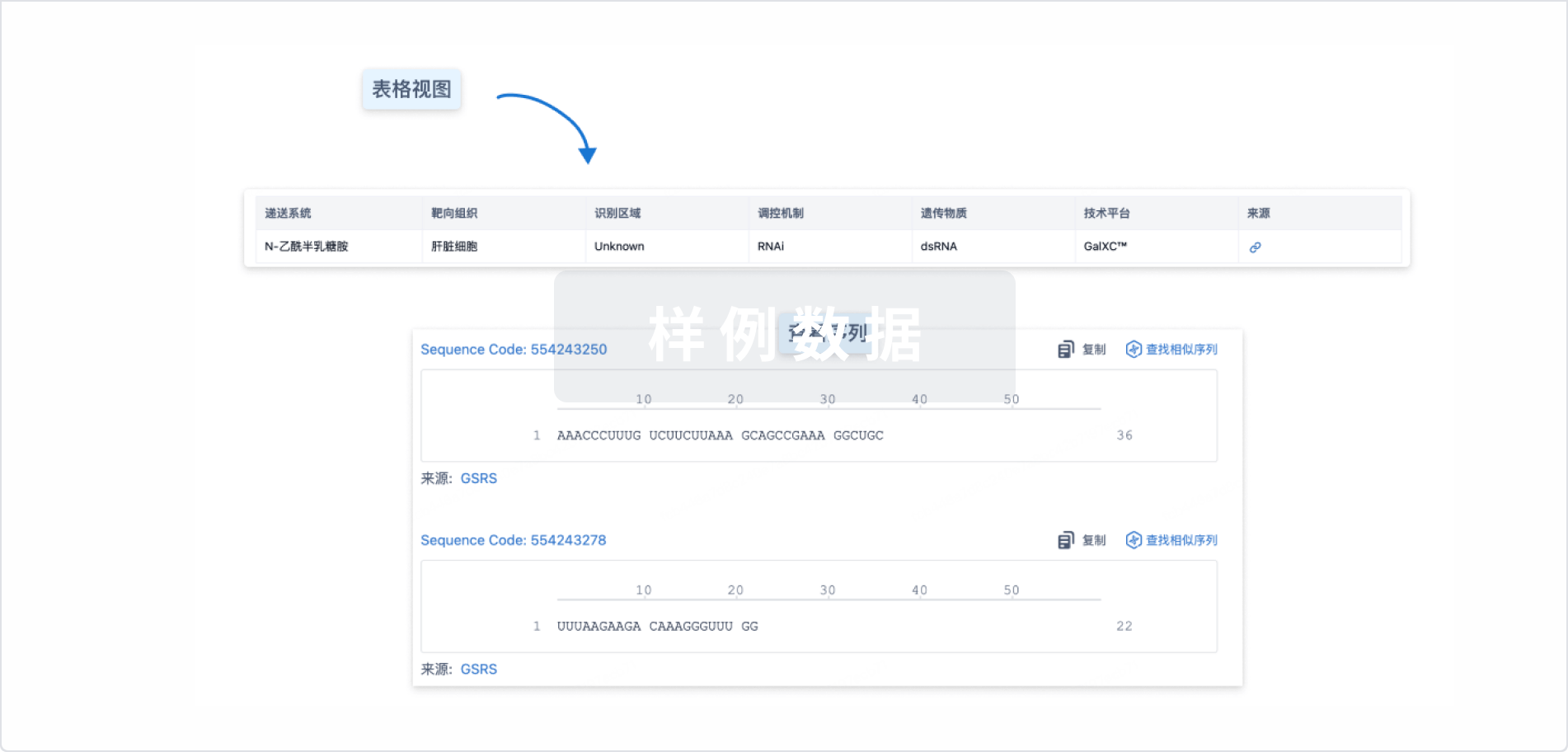
结构/序列
使用我们的RNA技术数据为新药研发加速。
登录
或
关联
1
项与 DV-281 相关的临床试验NCT03326752
Phase 1b Dose Escalation and Dose Expansion Trial of DV281 in Combination With an Approved Anti-PD-1 Inhibitor in Subjects With Advanced Non-Small Cell Lung Cancer
100 项与 DV-281 相关的临床结果
登录后查看更多信息
100 项与 DV-281 相关的转化医学
登录后查看更多信息
100 项与 DV-281 相关的专利(医药)
登录后查看更多信息
2
项与 DV-281 相关的文献(医药)2021-08-15Clinical cancer research : an official journal of the American Association for Cancer Research1区 · 医学
A Phase Ib Open-Label, Multicenter Study of Inhaled DV281, a TLR9 Agonist, in Combination with Nivolumab in Patients with Advanced or Metastatic Non–small Cell Lung Cancer
1区 · 医学
Article
作者: Janatpour, Mary J. ; Candia, Albert ; Leach, Joseph ; Bazhenova, Lyudmila ; Johnson, Melissa ; Janssen, Robert ; Coffman, Robert L. ; Gamelin, Erick ; Spira, Alexander I. ; Chow, Laura Q.M. ; Garon, Edward B. ; Cummings, Amy L.
Abstract:
Purpose::
Although PD-(L)1 inhibitors have shown efficacy in advanced/metastatic non–small cell lung cancer (NSCLC), many patients do not respond to this treatment and more effective combinations with acceptable toxicities are needed. To assess the potential benefit of combining localized innate immune stimulation with checkpoint blockade, the TLR9 agonist DV281 was combined with nivolumab in a phase Ib study.
Patients and Methods::
Patients after one or two prior lines of systemic therapy were enrolled in a dose-escalation study with a 3+3 design. DV281 was administered via inhalation in five dose cohorts at 1 to 25 mg; nivolumab 240 mg was administered intravenously every 2 weeks. Safety, tolerability, pharmacodynamics, and response to treatment were assessed.
Results::
Twenty-six patients with advanced NSCLC enrolled. Baseline programmed death ligand 1 (PD-L1) expression was present in 16 patients (61.5%); 21 (80.7%) had received previous anti–PD-1/PD-L1. Thirteen patients (50%) had stable disease, nine (34.6%) had progressive disease, and four (15.4%) were not evaluable. Median duration of disease control was 124 days. Adverse events were seen in 16 patients (61.5%), mostly grade 1/2 chills, fatigue, flu-like symptoms, diarrhea, and rash; there was only one grade 3 adverse event (dyspnea). Pharmacodynamic assessment, measured by IFN- inducible gene expression, showed target engagement in all dose cohorts. Systemic pharmacodynamic responses plateaued in the 2 highest dose cohorts.
Conclusions::
DV281 with nivolumab was well tolerated with target engagement observed at every dose. Pharmacodynamic advantages at doses above 10 mg were unclear. The long duration of disease control in 50% of patients suggests clinically relevant activity in this population of heavily pretreated patients.
2019-01-01International immunopharmacology2区 · 医学
Preclinical development of the TLR9 agonist DV281 as an inhaled aerosolized immunotherapeutic for lung cancer: Pharmacological profile in mice, non-human primates, and human primary cells
2区 · 医学
Article
作者: Kachura, Melissa A ; Renn, Alex ; Coffman, Robert L ; Traquina, Paula ; Kell, Sariah A ; Campbell, John D
CpG-motif-containing oligodeoxynucleotides (CpG-ODN) activate innate immunity through Toll-Like Receptor (TLR) 9 signaling and generate local immune responses when delivered directly to the lung. Herein we describe pharmacological studies in mice, cynomolgus monkeys, and in human primary cells which support the development of DV281, a C-class CpG-ODN, as an inhaled aerosolized immunotherapeutic for lung cancer to be combined with an inhibitor of the anti-programmed cell death protein 1 (PD‑1) immune checkpoint. In vitro, DV281 potently induced Interferon (IFN)‑α from monkey and human peripheral blood mononuclear cells (PBMCs), stimulated interleukin‑6 production and proliferation in human B cells, and induced TLR9-dependent cytokine responses from mouse splenocytes. Intranasal delivery of DV281 to mice led to substantial but transient cytokine and chemokine responses in the lung. Lung responses to repeated intranasal DV281 were partially to fully reversible 2 weeks after the final dose and were absent in TLR9-deficient mice. Single escalating doses of aerosolized DV281 in monkeys induced dose-dependent induction of IFN-regulated genes in bronchoalveolar lavage cells and blood. In a repeat-dose safety study in monkeys, inhaled DV281 was well-tolerated, and findings were mechanism of action-related and non-adverse. Co-culture of human PBMC with DV281 and anti-PD‑1 antibody did not augment cytokine or cellular proliferation responses compared to DV281 alone, indicating that the combination did not lead to dysregulated cytokine responses. These studies support clinical development of inhaled aerosolized DV281 as a combination therapy with anti-PD‑1 antibody for lung cancer immunotherapy.
100 项与 DV-281 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 晚期非小细胞肺癌 | 临床1期 | 美国 | 2017-09-20 |
登录后查看更多信息
临床结果
临床结果

转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用