预约演示
更新于:2026-05-25

Kangbuk Samsung Medical Center
更新于:2026-05-25
概览
标签
肿瘤
单克隆抗体
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
NCT07396961
Evaluation of the Consistency of the ASIS Line for Lumbar Level Identification in the Lateral Decubitus Position: Comparison With the Tuffier's Line
NCT07336329
Effectiveness of Periodic Use of Continuous Glucose Monitoring After Three Months of Continuous Use in Patients With Non-Insulin-Treated Type 2 Diabetes Patients: A Multicenter, Randomized, Parallel-Group, Open-Label, Non-Inferiority, Investigator-Initiated Trial
KCT0011448
Effectiveness of Periodic Use of Continuous Glucose Monitoring After Three Months of Continuous Use in Patients With Non-Insulin-Treated Type 2 Diabetes Patients: A Multicenter, Randomized, Parallel-Group, Open-Label, Non-Inferiority, Investigator-Initiated Trial
100 项与 Kangbuk Samsung Medical Center 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2026-12-31JOURNAL OF ENZYME INHIBITION AND MEDICINAL CHEMISTRY
Design, synthesis and biological evaluation of novel KRAS-G12D inhibitors
Article
作者: Nale, Sagar Dattatraya ; Kim, Chang Joong ; Moon, ByoungGon ; Ha, JaIn ; Ryu, Sungwook ; Park, JiMin ; Dong, Jae-June ; Jo, Yun Seong ; Baig, Mohammad Hassan
KRAS-G12D mutations are common drivers of pancreatic and colorectal cancers, yet effective targeted therapies remain limited. This study describes the design, synthesis, and biological evaluation of two novel KRAS-G12D inhibitors, GD-2 and GD-4. Both compounds exhibited strong antiproliferative activity in AGS and ASPC1 cancer cell lines, with IC₅。 values ranging from 0.2 to 1.8 µM. The protein binding assay also demonstrated high affinity for KRAS-G12D, with dissociation constants (Kd) of 146 nM for GD-2 and 3.18 nM for GD-4. Mechanistic investigations revealed that both compounds significantly reduced downstream, as evidenced by a clear decrease in phospho-ERK expression. Additionally, molecular dynamics simulations confirmed stable binding interactions within the KRAS-G12D pocket. Collectively, these findings identify GD-2 and GD-4 as promising therapeutic candidates for KRAS-G12D-driven cancers.
2026-07-01AMERICAN HEART JOURNAL
Design and rationale of the clinical trial to obtain the highest efficacy of dual antiplatelet therapy after carotid artery stenting in high bleeding risk patients (CHET): A multicenter, randomized, open-label, superiority trial
Article
作者: Park, Moo-Seok ; Baek, Jang-Hyun ; Kim, Yong-Won ; Park, Hee-Kwon ; Kim, Bum Joon ; Kim, Joong-Goo ; Song, Tae-Jin ; Lee, Seok-Yoon ; Lee, Seung-Jae ; Lee, Jun ; Lee, Seong-Joon ; Kim, Hyung Jun ; Jeong, Darda ; Yoo, Joonsang ; Kang, Hyun Goo ; Cho, Han-Jin ; Joon An, Sang ; Choi, Kang-Ho ; Woo, Ho Geol ; Kim, Young-Dae ; Seo, Woo-Keun ; Eun, Mi-Yeon ; Seo, Jung-Hwa ; Jung, Jin-Man ; Bang, Oh Young ; Shin, Dong-Woo ; Kim, Jun Yup ; Park, Hyungjong
RATIONALE:
Abbreviated dual antiplatelet therapy (DAPT) strategies effective in percutaneous coronary intervention among patients with high bleeding risk (HBR) may not be applicable to carotid artery stenting (CAS) owing to anatomical and procedural differences.
PRIMARY HYPOTHESIS:
Among patients with HBR undergoing CAS, abbreviated DAPT followed by SAPT will reduce clinically significant bleeding compared to prolonged DAPT, while maintaining noninferiority in net clinical outcomes, including ischemic and major bleeding events.
DESIGN:
CHET trial is a multicenter, randomized, open-label, superiority trial in HBR patients undergoing CAS. Assuming a 38% relative reduction in bleeding (10.4%-6.45%), 1,524 participants (762 per group) provide 80% power with a two-sided alpha of 0.05; the final target is 1,556 (778 per group), allowing 2% dropout. Key HBR criteria include age ≥75 years, ischemic stroke within 6 months, renal insufficiency, anemia, and thrombocytopenia. All patients will receive aspirin and clopidogrel for 30 days after CAS (enrichment period). Event-free patients on day 30 were randomized 1:1 to receive SAPT (aspirin 100 mg daily or clopidogrel 75 mg daily, at the treating physician's discretion) or continued DAPT for 11 months. The primary safety endpoint is clinically significant bleeding (BARC 2, 3, or 5) from day 30 to 12 months post-CAS. The secondary efficacy endpoint is a composite of nonfatal stroke, nonfatal myocardial infarction, cardiovascular death, and major bleeding (BARC 3 or 5).
ENROLLMENT DATES AND CURRENT STATUS:
CHET began enrollment on July 15, 2024. As of February 5, 2026, the trial is currently enrolling, with 328 participants enrolled. Enrollment is expected to be completed by November 2029, and follow-up by December 2030.
CONCLUSIONS:
CHET trial is the first randomized controlled trial to define optimal DAPT duration in HBR patients after CAS.
TRIAL REGISTRATION:
www.
CLINICALTRIALS:
gov (NCT06276374).
2026-06-01PSYCHIATRY RESEARCH
Association between premenstrual syndrome and postnatal depression in women with recurrent major depressive disorder
Article
作者: Cho, Sung Joon ; Kim, Won-Hyoung ; Rhee, Sang Jin ; Song, Yoojin ; Lee, Kyu Young ; Lee, Jung Jae ; Jeong, Ji-Woon ; Won, Seunghee ; Lee, Moon Soo ; Kim, Do Hoon ; Ahn, Yong Min ; Joo, Eun-Jeong ; Baek, Ji Hyun ; Kendler, Kenneth S ; Moon, Seok Woo ; Lee, Heon-Jeong ; Lee, Dongyun ; Myung, Woojae ; Song, Joo Yun ; Min, Sooyeon ; Park, Christopher Hyung Keun ; Yang, Jeong Hun ; Park, Jaesub ; Choe, Young Min ; Na, Kyoung-Sae ; Yoo, So Young ; Flint, Jonathan ; Lee, So Hee
Postnatal depression (PND) represents a major mental health concern with significant implications for mothers and children. Premenstrual syndrome (PMS) has been suggested as a potential risk factor for PND, although its role among women with recurrent major depressive disorder (MDD) remains unclear. Using data from the Korean Mood Disorder Genetic Study-Depression (KOMOGEN-D), an analysis of 2309 women with recurrent major depressive disorder and at least one childbirth experience was conducted to investigate the association between PMS and PND.PMS was defined by self-reported premenstrual emotional symptoms, and PND was defined as a depressive episode within 6 months postpartum. Logistic regression analysis was performed. Women with PMS demonstrated significantly higher rates of PND than those without PMS (45.5% vs. 22.5%, p < 0.001). Younger age (odd ratio [OR]: 0.93, 95% confidence interval [CI]: 0.93-0.94, p < 0.001), younger age at menarche (OR: 0.84, 95% CI: 0.8-0.87, p < 0.001), PMS (OR: 2.87, 95% CI: 2.4-3.45, p < 0.001), childhood sexual abuse (OR: 1.65, 95% CI: 1.33-2.04, p < 0.001), and a family history of MDD (OR: 1.76, 95% CI: 1.48-2.1, p < 0.001) were associated with PND. A positive association was observed between PMS symptom burden and PND incidence. Women with PND also exhibited earlier onset of depression, longer illness duration, and higher trauma exposure. These findings identify PMS as a marker of a clinically meaningful vulnerability profile within recurrent MDD, underscoring the need for tailored screening and intervention strategies across the reproductive life cycle.
2026-04-21
2026-04-08
·生物通
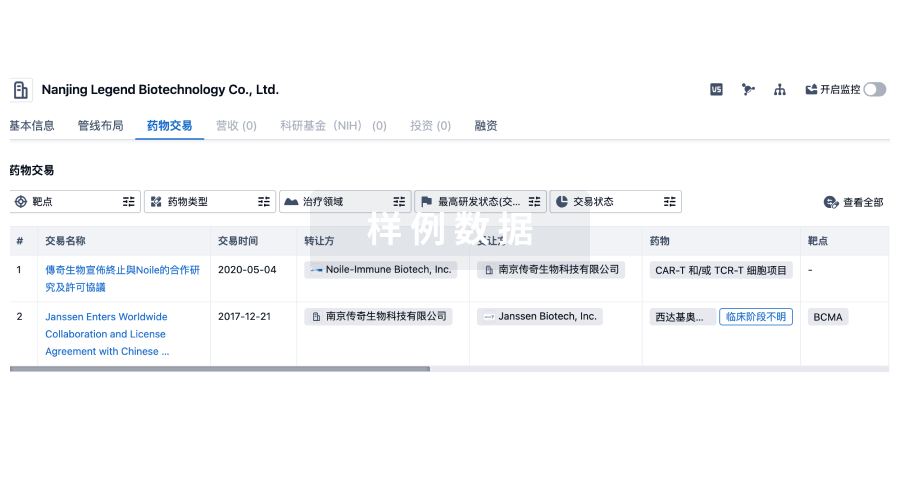
100 项与 Kangbuk Samsung Medical Center 相关的药物交易
登录后查看更多信息
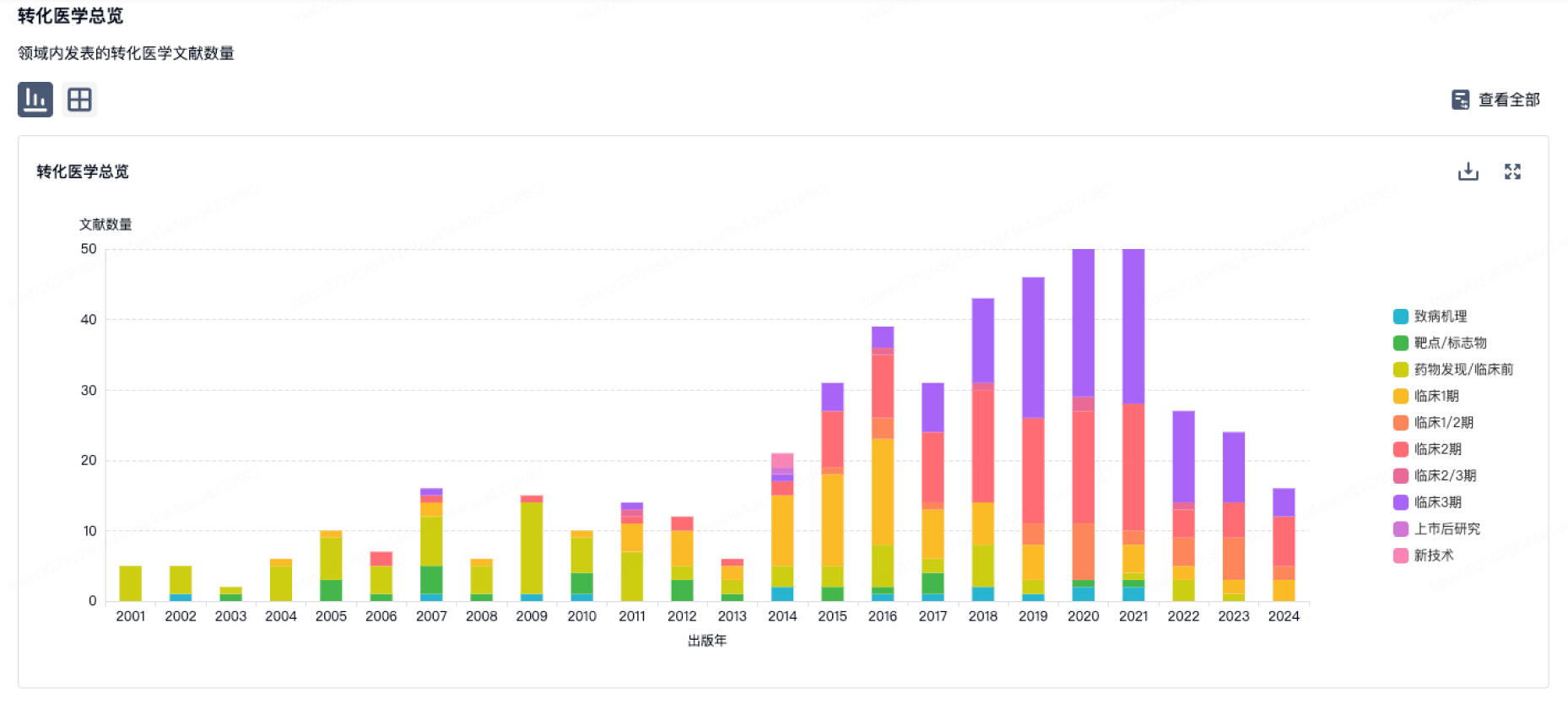
100 项与 Kangbuk Samsung Medical Center 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月30日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
临床1期
1
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
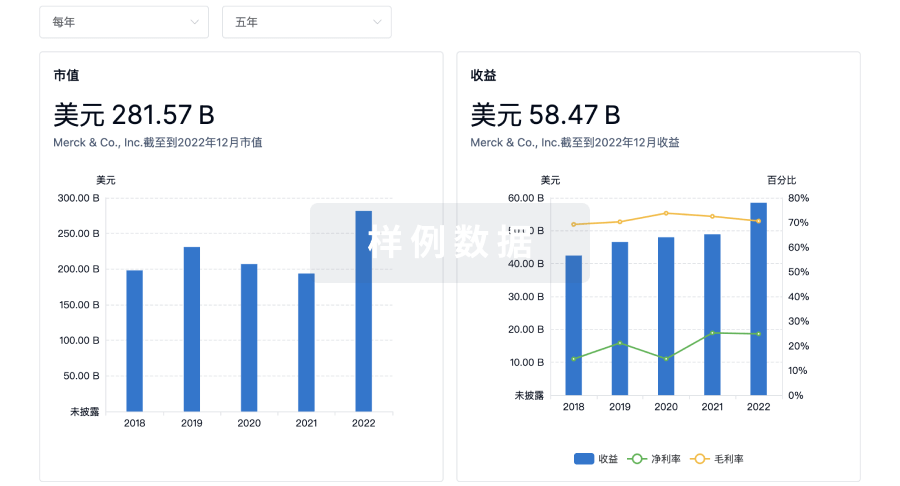
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用