预约演示
更新于:2026-03-04
Singlera Genomics, Inc.
更新于:2026-03-04
概览
关联
NCT06842563
A Multicenter Clinical Trial to Evaluate the Clinical Performance and Accuracy of the Human DAB2IP, CHFR, and GRASP Gene Methylation Kit (PCR-fluorescence Probe) in Patients With Suspected Hepatocellular Carcinoma
NCT06440018
INSPIRE: Integrating Circulating DNA Methylation and Fragmentomics to Scan and Pinpoint Cancer Signals Effectively
NCT06178809
Clinical Research on Dynamic Monitoring MRD Via Plasma ctDNA Predicting Postoperative Recurrence and Progression After Systemic Therapy of Hepatocellular Carcinoma
100 项与 江苏鹍远生物科技股份有限公司 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-06-01Phenomics (Cham, Switzerland)
Amyotrophic Lateral Sclerosis and Risk of Common Cancer: Mendelian Randomization Interrogation of Causality and Mediation
Article
作者: Li, Xiangnan ; Wang, Haijian ; Zhong, Fan ; Tan, Xiaoxue ; Liu, Gaifen ; Su, Zhixi
Supplementary Information:
The online version contains supplementary material available at 10.1007/s43657-024-00159-9.
2025-01-01International Journal of Endocrinology
Molecular Diagnosis of Thyroid Nodules Using Next‐Generation Sequencing in the Chinese Population
Article
作者: Wu, Jiajia ; Chen, Hui ; Chen, Yan ; Liu, Wei ; Ren, Yuanyuan ; Zhang, Hongfeng ; Liu, Rui ; Ji, Yuan ; Zhu, Min ; Jiang, Zhengzeng
Background:
Fine‐needle aspiration (FNA) cytology remains a challenge in the diagnosis of indeterminate thyroid nodules. Molecular testing can bridge the gap left by FNA cytology and improve the diagnostic accuracy of FNA.
Methods:
786 FNA samples and 40 formalin‐fixed paraffin‐embedded (FFPE) specimens from thyroid nodules were enrolled in next‐generation sequencing (NGS) molecular testing, which included gene mutation and gene fusion analysis. The molecular diagnostic performance was assessed by analyzing sensitivity, specificity, accuracy, negative predictive value (NPV), and positive predictive value (PPV).
Results:
Among 826 thyroid nodules, 409 were NGS‐positive (49.52%), with a high prevalence of
BRAF
V600E (36.32%, 300/826) and
RAS
(9.32%, 77/826) mutations, a low prevalence of
TERT
promoter mutations (1.69%, 14/826), and gene fusions involving
RET
(1.82%, 15/826),
NTRK3
(0.73%, 6/826),
ALK
(0.24%, 2/826), and
PAX8-PPARG
(0.12%, 1/826). With the analysis of genetic profiles in thyroid nodules,
BRAF
V600E,
TERT
mutations, and gene fusions were included in the 6‐gene test panel. The overall diagnostic performance of the 6‐gene test panel, including sensitivity, specificity, accuracy, NPV, and PPV, was 84.87%, 89.61%, 86.26%, 71.13%, and 95.15%, respectively. For thyroid nodules in Bethesda III, IV, and V, the diagnostic sensitivity, specificity, accuracy, NPV, and PPV of the panel were 85.71%, 88.89%, 86.36%, 61.54%, and 96.77%, respectively.
Conclusion:
The results reveal that the 6‐gene test panel as a “rule in” test in a clinical setting improves the accuracy of FNA cytology, potentially assisting in the diagnosis of the thyroid nodules with indeterminate FNA cytology.
2024-02-01Translational research : the journal of laboratory and clinical medicine
A diagnostic model based on DNA methylation haplotype block characteristics for identifying papillary thyroid carcinoma from thyroid adenoma
Article
作者: Shen, Yuling ; Xu, Dong ; Lai, Yi ; Li, He ; Liu, Yiying ; Gong, Chengxiang ; Feng, Ningning ; Zhang, Yunzhi ; Zhou, Jiaqing ; Liu, Hongmei
Papillary thyroid carcinoma (PTC) is the most prevalent form of thyroid cancer. Methylation of some genes plays a crucial role in the tendency to malignancy as well as poor prognosis of thyroid cancer, suggesting that methylation features can serve as complementary markers for molecular diagnosis. In this study, we aimed to develop and validate a diagnostic model for PTC based on DNA methylation markers. A total of 142 thyroid nodule tissue samples containing 84 cases of PTC and 58 cases of thyroid adenoma (TA) were collected for reduced representation bisulfite sequencing (RRBS) and subsequent analysis. The diagnostic model was constructed by the logistic regression (LR) method followed by 5-cross validation and based on 94 tissue methylation haplotype block (MHB) markers. The model achieved an area under the receiver operating characteristic curve (AUROC) of 0.974 (95% CI, 0.964-0.981) on 108 training samples and 0.917 (95% CI, 0.864-0.973) on 27 independent testing samples. The diagnostic model scores showed significantly high in males (P = 0.0016), age ≤ 45 years (P = 0.026), high body mass index (BMI) (P = 0.040), lymph node metastasis (P = 0.00052) and larger nodules (P = 0.0017) in the PTC group, and the risk score of this diagnostic model showed significantly high in recurrent PTC group (P = 0.0005). These results suggest that the diagnostic model can be expected to be a powerful tool for PTC diagnosis and there are more potential clinical applications of methylation markers to be excavated.
2026-01-10
优先审批诊断试剂临床研究
2026-01-08
优先审批临床研究
100 项与 江苏鹍远生物科技股份有限公司 相关的药物交易
登录后查看更多信息
100 项与 江苏鹍远生物科技股份有限公司 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年05月29日管线快照
无数据报导
登录后保持更新
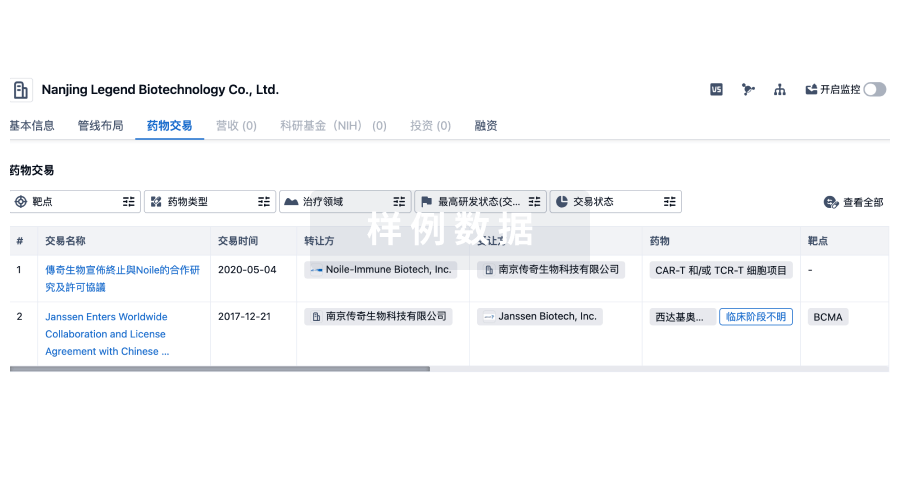
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
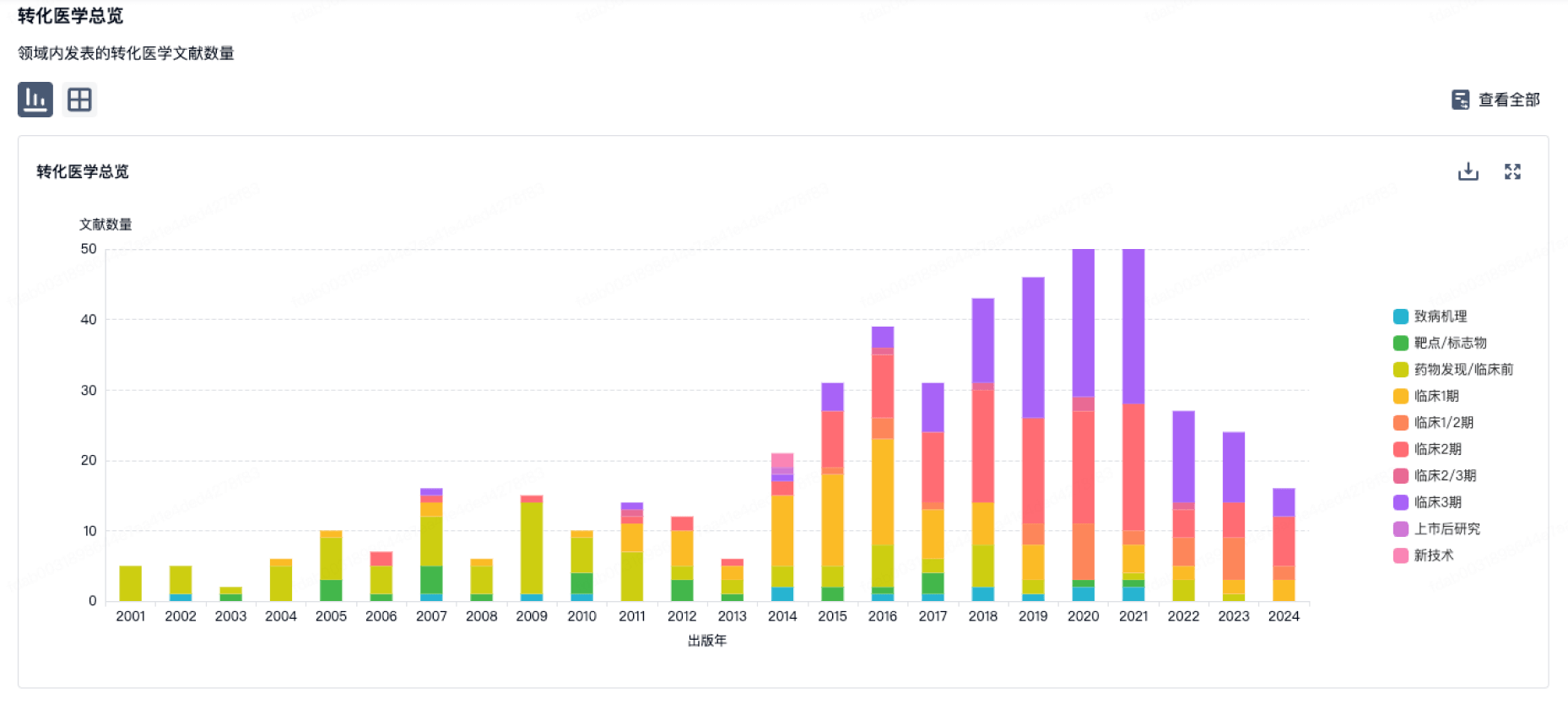
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
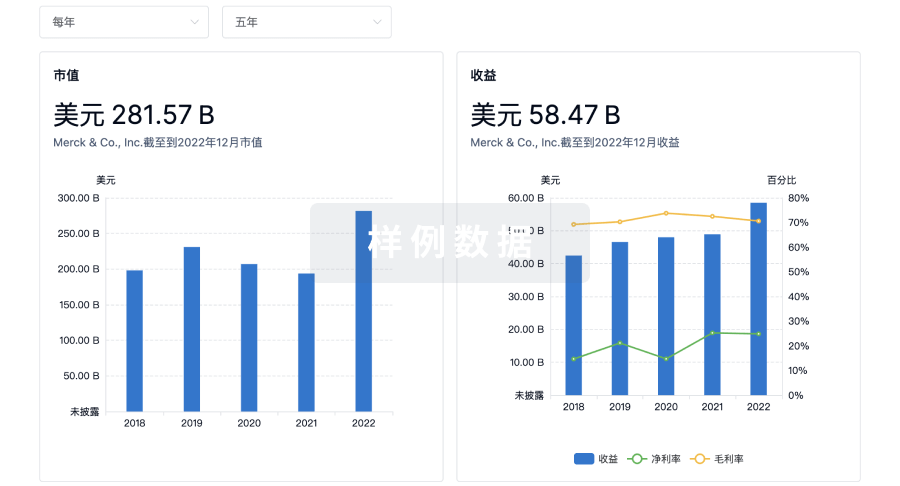
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用