预约演示
更新于:2026-03-15
Virbac SA
更新于:2026-03-15
概览
关联
100 项与 Virbac SA 相关的临床结果
登录后查看更多信息
0 项与 Virbac SA 相关的专利(医药)
登录后查看更多信息
59
项与 Virbac SA 相关的文献(医药)2025-07-01·JOURNAL OF VETERINARY PHARMACOLOGY AND THERAPEUTICS
Pharmacokinetic–Pharmacodynamic Cutoff Values for Doxycycline in Pigs to Support the Establishment of Clinical Breakpoints for Antimicrobial Susceptibility Testing
Article
作者: Ferran, Aude A. ; del Castillo, Jérôme R. E. ; Lees, Peter ; Toutain, Pierre‐Louis ; Pelligand, Ludovic ; Croubels, Siska ; Roques, Béatrice B. ; Bousquet, Eric ; Bousquet‐Melou, Alain
ABSTRACT:
This meta‐analysis provides a population model of doxycycline (DOXY) disposition in pigs for computation of PK/PD cutoff values corresponding to differing modalities of DOXY administration orally in pigs. This analysis enables establishment of specific clinical breakpoints for the development of antimicrobial susceptibility testing of DOXY in pigs. The meta‐analysis of 380 data sets, totaling 3295 plasma concentrations obtained from 300 pigs weighing 8.5–101 kg, was performed using a non‐linear mixed effect model. The plasma clearance for a typical 50 kg BW pig was estimated to be 0.259 L/kg/h with a corresponding plasma half‐life of 7.33 h. The bioavailability of DOXY administered in feed under field conditions was estimated to be 50%, with a large between‐subject variability of 84.8%. The bioavailability of DOXY in solution in drinking water was significantly lower (30.7%) but much less variable, with a between‐subject variability of 34.3%. Several dosing schedules (5 to 20 mg/kg per day) for two administration modalities (drinking water vs. food) were simulated to calculate the corresponding PK/PD cutoffs. The highest PK/PD cutoff of 0.50 mg/L was obtained for DOXY administered in feed at 20 mg/kg BW.
2025-03-04·NEW ZEALAND VETERINARY JOURNAL
Effect of a pre-calving injectable trace mineral supplement on white blood cell function in seasonally calving pastoral dairy cows
Article
作者: Bates, AJ ; Fitzpatrick, C ; Wells, M ; Laven, RA
AIMS:
To investigate the effect of injection of trace mineral supplement (TMS) 14-28 days before calving on white blood cell count (WBCC) and function, serum antioxidant capacity (SAC) and reactive oxygen species (ROS) in pasture-fed cattle after calving.
METHODS:
On each of two South Island, seasonally calving, pastoral dairy farms,1 month before dry-off, a random sample of 150 multiparous cows predicted to calve within 7 days of the herd's planned start of calving (PSC) were stratified on individual somatic cell count, age, breed and expected calving date. On each farm, 14-24 days before PSC, 60 selected cows were randomly assigned for TMS (Zn, Mn, Se, Cu) injection, and 60 were controls. All 240 cows were contemporaneously injected with hydroxocobalamin, and controls with Se. Blood samples were collected pre-injection and 3, 12 and 40 days after calving. Phagocytic activity, count and proportion of neutrophils, lymphocytes and monocytes, WBCC, ROS, SAC were measured. Plasma concentrations of Se, Cu and glutathione peroxidase (GPx) were monitored from a random subset of animals. Differences attributable to TMS were estimated using mixed-multivariable Bayesian analysis, expressed as mean and highest density interval (HDI).
RESULTS:
Three and 40 days after calving, TMS-treated cows had 0.36 (90% HDI = 0.00-0.77) x 109 and 0.25 (90% HDI = 0.00-0.55) x 109 fewer neutrophils/L. Neutrophils comprised 6 (90% HDI = 0-11)% and 4 (90% HDI = 0-8)% less of the WBCC, and the neutrophil count was 14 (90% HDI = 0-27)% and 9 (90% HDI = 0-18)% less than controls. However, 3 days after calving, there were 7 (95% HDI = 2-12)% more cells phagocytosing and 2,900 (95% HDI = 2,600-3,200) more bacteria ingested/cell. Twelve and 40 days after calving, TMS-treated cows had 0.65 (95% HDI = 0.17-1.17) x 109 and 0.28 (95% HDI = 0.00-0.59) x 109 more lymphocytes/L. Lymphocytes comprised 10 (95% HDI = 3-18)% and 5 (95% HDI = 0-9)% more of the WBCC, and the lymphocyte count was 30 (95% HDI = 11-51)% and 9 (95% HDI = 0-9)% more than controls. There were no meaningful differences in ROS, SAC, ROS/SAC, other white blood cells, or WBCC. Plasma Cu, Se and GPx concentrations were above recommended thresholds.
CONCLUSIONS:
Pre-calving TMS injection was associated with differences in white blood cell population and function that may reduce the risk of disease.
ABBREVIATIONS:
BHOB: Beta-hydroxybutyrate; GPx: Glutathione peroxidase; HDI: Highest density interval; MESF: Molecules of equivalent soluble fluorophore; OSi: Oxidative stress index; PSC: Planned start of calving; ROPE: Region of probable equivalence; ROS: Reactive oxygen species; SAC: Serum antioxidant capacity; THI: Temperature humidity index; TMS: Trace mineral supplement; WAIC: Widely applicable information criterion; WBCC: White blood cell count.
2025-02-01·CELL STRESS & CHAPERONES
Molecular response of canine testis to GnRH agonist: Insights into AR, HIF-1α, and HSPs expression during arrest and recovery of spermatogenesis
Article
作者: Packeiser, Eva-Maria ; Ay, Serhan ; Goericke-Pesch, Sandra ; Findik, Murat ; Speiser-Fontaine, Christelle ; Körber, Hanna ; Selçuk, Murat ; Vasetska, Anastasiia ; Aslan, Selim ; Binli, Firdevs
Slow-release gonadotropin-releasing hormone (GnRH) agonist implants are frequently used for contraception in male dogs. Although the effects are fully reversible, there is still concern about the safety of the implant's mode of action. Addressing this, we investigated cellular stress and androgen receptor (AR) signaling during downregulation and recovery. Testicular tissues were sampled from dogs castrated at different time points after GnRH implant removal and compared with untreated controls. AR, hypoxia-inducible factor 1 (HIF1A), heat shock proteins heat shock protein 72 (HSP72), heat shock protein 73 (heat shock cognate, HSPA8) (HSP73), heat shock protein A2 (HSPA2), heat shock protein 90 alpha (inducible isoform) (HSP90AA1), and heat shock protein 90 beta (constitutive isoform) (HSP90AB1) were investigated by quantitative real-time polymerase chain reaction and AR, HSP72, HSP73, and HSP90 immunohistochemically. While AR, HIF1A, and HSP70 were upregulated at gene expression level, HSPA8, HSPA2, and HSP90AA1 expression were downregulated during spermatogenic arrest; HSP90AB1 expression did not change. Immunohistochemistry verified AR-expression in Sertoli, peritubular, and Leydig cells, occasionally also in spermatogonia. Stress-inducible HSP72 was occasionally detected, while constitutive HSP73 and HSP90 were abundantly expressed by germ cells. Our results were similar to studies on seasonal breeders such as pine voles, geese, fish, and soft-shelled turtles. Accordingly, GnRH implants did not impose additional cellular stress on testicular cells when compared with natural recrudescence. Since comparative data on HIF1α are scarce, we cannot draw conclusions about hypoxic conditions.
43
项与 Virbac SA 相关的新闻(医药)2026-02-25
—TOP10企业、增长逻辑、中国布局与老龄化下的新赛道一、全球宠物医药市场:规模、增速与结构性机遇
根据QYResearch、Grand View Research及格隆汇等机构综合数据:2025年全球宠物医药市场规模达200亿美元(约合1450亿元人民币),同比增长8.5%;未来五年(2026–2030)复合年增长率(CAGR)预计为8.7%–9.2%,2030年有望突破300亿美元;区域分布:北美:占比35%(美国为主,人均宠药支出超$120/年);欧洲:占比28%(德国、法国、英国领先);亚太:占比22%,增速最快(CAGR 12%),中国为核心引擎。
驱动因素:“宠物伴侣化”趋势深化;老龄宠物慢性病管理需求上升;单克隆抗体、口服驱虫等创新药加速商业化;宠物保险渗透率提升(美国达25%,中国不足1%但快速起步)。二、2025年全球宠物医药营收TOP10企业榜单排名公司名称2025年宠物药营收(亿美元)总部核心市场1Zoetis(硕腾)52.3美国全球2Boehringer Ingelheim(勃林格殷格翰动保)28.7德国欧美+中国3Merck Animal Health(默沙东动保)24.1美国北美、拉美4Elanco(礼蓝动保)18.9美国全球5Virbac(维克)12.6法国欧洲、东南亚6Ceva Santé Animale(诗华)10.8法国拉美、非洲7Dechra Pharmaceuticals9.5英国欧美专科药8Vetoquinol(威隆)6.2法国欧洲9Norbrook(诺贝罗)4.8北爱尔兰英联邦国家10Kindred Biosciences(被硕腾收购)—美国创新生物药
注:部分企业未单独披露宠物药收入,数据为估算值(基于动保总营收中宠物占比推算)。三、头部企业核心产品与竞争优势差异化企业代表产品/品牌技术平台核心优势ZoetisApoquel(犬特应性皮炎)、Librela(犬骨关节炎单抗)、Simparica Trio(三合一驱虫)单抗、JAK抑制剂、寄生虫靶向药全球最大宠物药企,研发管线最深,数字化工具(VetConnect)绑定兽医勃林格殷格翰NexGard(口服驱虫)、Vetmedin(犬心衰药)、Caninsulin(犬猫胰岛素)心血管、内分泌、寄生虫领域深厚积累欧洲本土信任度高,疫苗+治疗药协同默沙东动保Bravecto(长效驱虫,12周)、Nobivac(犬猫疫苗)长效制剂技术、疫苗平台驱虫药全球市占率前三,渠道覆盖广礼蓝动保Credelio(驱虫)、Entyce(食欲刺激剂)小分子创新药从礼来拆分后聚焦高毛利专科药VirbacDentaflex(口腔护理)、Allerderm(皮肤屏障修复)专科护理、外用制剂在皮肤、口腔等慢病管理细分领先DechraOsphos(马骨代谢药)、Torigen(肿瘤免疫疗法)专科药、肿瘤免疫专注高价值小众市场,毛利率超65%
竞争本质差异:美国企业:重“重磅炸弹”创新药,高定价、强专利壁垒;欧洲企业:重“全生命周期管理”,覆盖预防-治疗-护理;中小企:靠细分专科(如肿瘤、牙科、行为药)突围。四、跨国集团在中国宠物医药市场的份额与产能布局1. 市场份额(2025年)外资合计占据中国宠物药品约70%的销售额,其中:硕腾:约35%(驱虫、皮肤病绝对领先);勃林格殷格翰:约15%(心衰、驱虫);默沙东:约12%(Bravecto为主);礼蓝、Virbac等:合计约8%。
国产企业(如瑞普、海正动保、宠爱国际自研品牌)主要集中在中低端驱虫、消炎药,高端处方药仍严重依赖进口。2. 在华产能与战略投资硕腾:苏州工厂已投产Simparica系列口服片,供应中国及亚太;与京东健康、新瑞鹏共建“处方药直供”闭环。勃林格殷格翰:上海张江设立宠物药CDMO平台,支持本地注册;2025年推出“中国定制版”NexGard Mini(针对小型犬)。默沙东:浙江建德基地生产Bravecto咀嚼片,实现本地灌装,缩短供货周期至2周内。礼蓝:通过收购南京天邦切入宠物疫苗,并与农科院合作开发猫三联国产化。Virbac:与中牧股份合资成立“维克中牧”,主打口腔与皮肤护理产品本地化生产。
战略共性:“本地注册 + 本地生产 + 本地渠道”三位一体,应对中国日益严格的进口药品监管。五、中国宠物医药法规环境:机遇与挑战并存
2024–2025年,多项关键政策重塑市场:
《宠物用兽药注册管理办法(试行)》出台(2024年12月)首次将宠物药与食品动物药分类管理;设立“优先审评通道”,创新药审评时限压缩至12个月;影响:为国产宠物药打开政策窗口,瑞普、海正等加速申报。
处方药线上销售“白名单”制度试点(2025年)允许持证平台(如京东健康、阿里健康)在兽医远程问诊后销售处方药;影响:打破传统渠道垄断,推动DTC(直面消费者)模式。
新版GMP对宠物药企强制实施(2025年底)要求独立生产线、质量追溯系统;影响:淘汰中小作坊式企业,行业集中度提升。
宠物疫苗强制免疫目录未纳入,市场化程度高猫三联、犬四联等完全由市场决定,利好创新疫苗企业。六、人口结构变迁下的中国宠物医药新赛道
面对出生率持续走低(2025年总和生育率约1.0)与老龄化加速(60岁以上人口超3亿),宠物成为情感替代与陪伴刚需。以下细分赛道值得重点布局:1. 老年宠物慢病管理需求:犬猫糖尿病、关节炎、肾衰、心脏病高发;机会产品:口服降糖药(如Glipizide仿制);关节保健品(含UC-II、Omega-3);心衰用药(如匹莫苯丹国产化)。2. 心理健康与行为调节背景:独居老人/年轻人增多,分离焦虑、攻击行为频发;机会产品:行为调节营养补充剂(含L-茶氨酸、α-乳清蛋白);天然镇静喷雾(信息素类产品,如Adaptil仿制)。3. 口腔与皮肤专科护理数据:80%以上老年犬有牙周病,60%猫有慢性皮肤病;机会产品:家用牙科洁牙凝胶;屏障修复乳液(含神经酰胺、燕麦提取物)。4. 居家诊断与慢病监测趋势:结合智能项圈、尿检试纸、血糖仪;机会方向:宠物家用POCT(即时检测)试剂盒;与SaaS平台联动的健康管理服务。5. 平价替代与普惠处方药痛点:进口药价格高昂(如Apoquel 300元/片);机会:高质量仿制药(如奥拉替尼);中药复方制剂(如清热解毒口服液用于猫鼻支)。七、结语:从“进口依赖”走向“中国创新”
2025年,中国宠物医药市场正处于历史性拐点:一方面,跨国巨头凭借产品力与品牌牢牢把控高端市场;另一方面,政策松绑、资本涌入、临床需求爆发,为本土企业创造前所未有的突围窗口。
未来五年,谁能抓住“老龄化宠物+孤独经济”的结构性红利,谁能打通“研发-注册-渠道-服务”闭环,谁就将在这片千亿蓝海中赢得属于中国品牌的席位。
数据来源:农业农村部、中国兽药协会、QYResearch《2025全球宠物医药报告》、京东《2023中国宠物行业白皮书》、上市公司公告、行业访谈(截至2026年1月)免责声明:本文不构成任何投资或医疗建议,市场有风险,决策需谨慎。
2025-12-24
·医药健闻
全球医疗行业每日重点资讯
文 | 苏丁
企业动态
强生公司(Johnson & Johnson)周一遭遇重大法律挫折,巴尔的摩陪审团判决该公司向因使用婴儿爽身粉罹患癌症的女性支付超过15亿美元赔偿。这一裁决标志着该公司持续发酵的滑石粉诉讼危机中创下的最高单笔赔偿纪录。一名女性原告胜诉的原因为陪审团认定强生及其子公司未就滑石粉产品中的石棉成分向消费者发出警示。她在持续多年每日使用婴儿爽身粉后,于2024年1月被诊断出腹膜间皮瘤。
全球动保巨头维克集团(Virbac)宣布,以约1亿英镑(折合人民币约9.51亿元)完成对诺布鲁克实验室(Norbrook Laboratories)旗下猫甲亢治疗药物——甲巯咪唑口服溶液(商品名:Thyronorm/Felanorm-美国市场)的收购,交易涵盖该产品的全球生产、研发及商业化相关全部权益。该产品是针对猫甲状腺功能亢进症(甲亢)的专属治疗药物,而猫甲亢是老年猫咪最常见的内分泌疾病。诺布鲁克实验室将继续作为Virbac的合作伙伴,担任该产品的合同生产方(CMO)。
罗欣药业下属子公司山东罗欣拟将其持有的罗欣安若维他药业(成都)有限公司20%股权以512.5万美元转让给Helix Healthcare B.V.。本次股权转让前,山东罗欣持有罗安公司70%股权,本次股权转让完成后,山东罗欣持有罗安公司50%股权,罗安公司将不再纳入公司合并报表范围。
诺纳生物与CDMO企业博腾正式达成深度战略合作。双方将聚焦双抗、多抗等复杂抗体类新型治疗方式的全生命周期研发生产,通过“创新技术平台+产业化落地能力”的精准协同,破解新型抗体药物工艺开发难、合规要求高、成本挑战大、转化周期长的行业痛点,加速创新疗法从实验室走向临床及市场,为全球患者提供更具可及性的突破性治疗方案。双方将共同组建联合开发管理团队,针对诺纳相关项目推进一体化开发与全程管理,并在项目管理、质量体系等关键职能上实现深度协同。双方将重点围绕复杂抗体(包括双抗、多抗及非对称抗体等)项目的全生命周期开展合作。
诺纳生物宣布,拓展其一体化药物发现与开发框架,以支持早期临床开发及研究者发起的临床试验(IITs)。此次拓展将诺纳生物在药物发现及新药临床试验(IND)申报支持等方面的能力,进一步延伸至CMC开发、毒理学研究及GMP生产等领域,全面增强了公司在这些关键环节的专业实力。通过战略合作、平台并购以及内部能力建设,诺纳生物助力全球生物制药企业加速启动临床试验。
金赛药业与Partex AI达成药物开发战略合作。双方将结合金赛多年重大疾病领域创新药物的开发经验与Partex AI人工智能技术赋能药物全生命周期的前沿技术积累,共同加速创新药研发与商业化。根据合作协议,金赛药业与Partex AI将共同应用Partex自研的Foundation Model与尖端AI驱动平台,加速药物从早期发现到商业化开发全流程,如应用AI筛选并优化候选药物、新靶点识别,推动金赛核心业务领域的业务拓展与海外商业化。
产业动态
雅培宣布其Volt脉冲场消融(PFA)系统已获得美国食品药品监督管理局(FDA)批准,用于治疗房颤患者。这一获批标志着雅培正式进军美国PFA市场,将与美敦力、波士顿科学、强生医疗科技和Kardium等公司展开激烈竞争。雅培介绍,Volt采用单导管PFA方法,旨在优化工作流程并提高手术灵活性。它巧妙地将球囊篮式导管与EnSite X EP心脏标测系统相结合。
荃信生物与Windward BioGroup AG的附属公司LE2025 Therapeutics AG订立许可及合作协议。该协议授予LE2025在全球范围(不包括中国内地、中国台湾、中国香港及中国澳门)内开发及商业化QX027N的独家权利。作为回报,集团将有权收取总额高达7亿美元的付款,包括首付款、Windward Bio的股权、开发及商业里程碑付款,以及根据QX027N在许可地区的销售净额收取分级特许权使用费。
远大医药与祐儿医药达成产品合作协议。远大医药将获得全球首款用于紧急治疗I型过敏反应(包括严重过敏反应)的肾上腺素鼻喷雾剂Neffy(优敏速)在中国大陆合作渠道内的独家商业化权益以及在中国香港的非独家商业化权益。此次合作覆盖2mg以及1mg两种规格,分别适用于成人和30kg以上儿童患者、15—30kg儿童患者。
三力制药近期与海南大学达成技术转让协议,以总额2亿元受让阿尔茨海默病(AD)候选药物HXW2324化合物及相关专利申请权。HXW2324化合物是用于开发阿尔茨海默病(AD)新型治疗药物的临床前候选化合物。本次合同约定的发明专利权或专利申请权的转让价款总额2亿元,分为0.2亿元里程碑款(含税)与1.8亿元销售提成(含税)两部分,均按阶段分期支付。
GSK 宣布,NMPA已批准美泊利珠单抗注射液用于未充分控制的以血嗜酸性粒细胞升高为特征的慢性阻塞性肺疾病(COPD)成人患者的维持治疗。这也是中国首个且唯一获批的每月给药一次,用于治疗血嗜酸性粒细胞计数(BEC)≥150细胞/μL 的广泛 COPD 患者的生物制剂。
参天公司旗下环孢素滴眼液(Ⅲ)维卡思(Verkazia)在中国正式上市,用于治疗4岁及以上儿童和青少年的严重性春季角结膜炎,填补了免疫抑制剂在儿童适应症方面的空白。维卡思是严重性春季角结膜炎治疗领域中国首个获批的针对儿童及青少年的创新型无防腐剂免疫抑制剂,也是目前已发布的三批《临床急需境外新药名单》中唯一儿童眼科用药。
迈威生物宣布,其自主研发的抗ST2单抗创新药的临床试验申请正式获得美国食品药品监督管理局(FDA)的许可,可针对中重度慢性阻塞性肺疾病(COPD)开展 IIa 期临床研究。
罗氏(Roche)宣布,美国FDA已加速批准CD20 x CD3靶向双特异性抗体Lunsumio Velo(mosunetuzumab)皮下(SC)制剂,用于治疗接受过两线或以上系统治疗的复发或难治性(R/R)滤泡性淋巴瘤(FL)成人患者。勃林格殷格翰(Boehringer Ingelheim)宣布,其所开发的小分子片剂Jascayd(nerandomilast)已获得美国FDA批准用于治疗成人进行性肺纤维化(PPF)。
Abcam宣布,20μl/μg小包装规格一抗产品数量再次新增,目前可提供超过4500种小包装一抗。产品广泛覆盖肿瘤、免疫、神经科学、代谢、表观遗传学、信号通路及细胞生物学等多个研究领域靶点,旨在更好地满足科研工作者多样化的实验需求。
联系美通社
+86-10-5953 9500
info@prnasia.com
2025-11-14
Bringing medical advances from the lab to the clinic.
(点击👆,免费获取美国NIH基金资助项目大数据分析)
慢性疼痛(Chronic Pain) 指疼痛持续超过3个月以上,已超出正常组织损伤修复时间范围,是一种独立的慢性疾病状态,而非仅仅是其他疾病的附属症状。其病理机制复杂,涉及外周痛觉调节紊乱、中枢敏化、情绪认知参与、炎症免疫通路异常等多因素互动,是美国最典型的大规模公共卫生问题之一。
最新研究进展
中枢敏化机制研究更深入:脑网络、脑区功能连接与疼痛记忆的长期可塑性成为新的解释框架,为表型分层与预后判断提供思路。
新型靶点药物开发推进:从传统阿片类管理转向非阿片机制,包括Nav1.7、TRPV1、CGPR通路、小胶质细胞抑制剂、炎性介质阻断等方向均在临床试验中推进。
神经调控和介入治疗发展迅速:脊髓刺激、外周神经调控、TMS/tDCS 等非侵入电调控逐渐进入标准路径探索。
AI、穿戴设备用于客观测量与实时管理:连续监测痛感、睡眠、活动量与心理压力成为患者长期管理的有力工具,有助于个体化治疗匹配。
跨学科综合管理概念强化:疼痛管理已经逐渐从“药物中心”走向“疼痛+心理+睡眠+运动”的多轴综合管理模式。目前仍待解决的核心临床痛点
缺乏稳定、客观、可广泛使用的生物标志物,临床仍以主观评分为主。
对复杂中枢敏化人群缺乏精准亚型分类与治疗匹配。
非阿片类创新药物在“真实临床结局改善”方面仍需更强证据。
高合并症(抑郁、焦虑、睡眠障碍)患者管理路径仍不够系统化。
可及性与长期管理不足,特别是基层医疗系统对慢性疼痛处置能力有限。
慢性疼痛的未来突破方向不再是寻找“一个更强的新止痛药”,而是建立基于生物学分层、神经网络调节、心理行为整合与长期数字化管理的综合机制治疗模式。
我们仅对美国国立卫生研究院(NIH)资助的在研相关项目进行梳理,希望给同仁们的选题思路提供一点启发。
2025年,以 "Chronic Pain"为检索词、在题目中进行检索,美国NIH针对慢性疼痛的在研有186项。
一,谁获得了这些研究?
1. 在研基金最多的PI:
ADAMS, MEREDITH C. B.,维克森林大学健康科学(WAKE FOREST UNIVERSITY HEALTH SCIENCES)
KAWI, JENNIFER,德克萨斯大学休斯顿健康科学中心(UNIVERSITY OF TEXAS HLTH SCI CTR HOUSTON)
VRANCEANU, ANA-MARIA,麻省总医院(MASSACHUSETTS GENERAL HOSPITAL)
2,基金最多的研究机构
WAKE FOREST UNIVERSITY HEALTH SCIENCES 维克森林大学健康科学中心
UNIVERSITY OF PENNSYLVANIA 宾夕法尼亚大学
UNIVERSITY OF TEXAS HEALTH SCIENCE CENTER AT HOUSTON 德克萨斯大学休斯顿健康科学中心
UNIVERSITY OF WASHINGTON 华盛顿大学(西雅图)
MASSACHUSETTS GENERAL HOSPITAL 麻省总医院
二,研究热点
研究领域总览(根据关键词)
研究热点包括:神经病理性疼痛(Neuropathic Pain)、老年人(Older Adults)、大脑(Brain)、慢性疼痛治疗(Chronic Pain Treatment)、生活质量(Quality of Life)、阿片类药物使用障碍(Opioid Use Disorder)等。
三,借鉴与突破
我们也分享在美国该领域的几项课题摘要,希望对同仁们有所启发。
A,The Penn Human Precision Pain Center (HPPC): Discovery and Functional Evaluation of Human Primary Somatosensory Neuron Types at Normal and Chronic Pain Conditions
Migraine, one of the most common primary headache disorders, affects 1 in 4 US households. This complex neurologic disorder is mediated in part by alterations in trigeminal somatosensation, which manifests as head/fa- cial pain and/or trigeminal allodynia. Effective treatments for migraine are still limited, and our knowledge about human trigeminal system at baseline and migraine conditions are sparse. In response to RFA-NS-22-018, HEAL Initiative: Discovery and Functional Evaluation of Human Pain-associated Genes & Cells, we propose to form the Penn Human Precision Pain Center (Penn HPPC) to elucidate molecular, cellular, epigenetic, and physiological profiles of human trigeminal ganglion (TG) sensory neurons at baseline and migraine conditions. The Penn HPPC will be composed of Penn and international investigators with multidisciplinary expertise. The PI, two MPIs, and two co-Is are currently collaborating on a single-soma deep RNA-seq of human dorsal root ganglion (DRG) neuron project, which form a strong foundation for this application. Specifically, the Penn HPPC will contain three cores and perform three projects. The administrative core will serve as a sole organizational and administrative entity for the Penn HPPC. The human tissue core will function as the sole entity for procuring and storing human tissues and distributing human tissues among research projects. The data core will be the sole entity for storage, processing, and distribution of all data from the HPPC projects. In project 1, we will employ three complementary approaches, a laser capture microdissection based single-neuron-soma deep RNA-seq (a novel method developed by the PI’s lab, which has been successfully used with human DRG neu- rons), 10 x Visium (a commercially available spatial transcriptomics platform), and MERSCOPE (another com- mercially available spatial transcriptomics platform) to conduct single-soma RNA-seq of neurons and non-neu- ronal cells of TGs from control donors and those with migraine. In project 2, we will perform two types of single- nucleus multi-omics sequencing with TGs from control donors and those with migraine: chromatin accessibility (ATAC plus RNA, 10x Genomics multiome assay) and DNA methylation (methylation plus RNA, snmCAT-seq). In project 3, we will recruit migraine patients and control human subjects to conduct pain questionnaires, soma- tosensory tests, blink reflex, and in vivo microneurography recordings of trigeminal and spinal sensory afferents. Together, our proposed Penn HPPC will produce comprehensive and multi-dimensional datasets of human TGs at baseline and migraine conditions, which will generate unprecedent molecular, cellular, and functional atlas to understand normal trigeminal sensations and abnormal sensations associated with migraine. Our results may also lead to discovery of new biomarkers for migraine diagnosis and/or identification of novel potential drug targets for migraine treatment.
B, Personalized Auricular Point Acupressure for Chronic Pain Self-Management in Rural Populations
Despite a range of therapeutic approaches, chronic musculoskeletal pain (CMP) persists at a high rate, creating a public health burden. Our long-term goal is to increase access and scalability of evidence-based interventions while addressing pain care disparities for rural individuals with limited resources and/or endure long distances to specialty pain care. We will conduct a hybrid implementation-effectiveness trial, guided by the Reach, Effectiveness, Adoption, Implementation, and Maintenance framework in diverse healthcare systems and communities across the United States in Texas and South Carolina focusing on rural health populations. Specifically, in our UG3 phase, we aim to plan and evaluate our Auricular Point Acupressure Self-Management (APA-SM) program integrated into rural health care and communities. Our team has accumulated extensive evidence supporting the use of APA-SM in decreasing pain intensity, reducing pain interference, and improving physical function. To maximize self-management of pain, we successfully developed and tested a smartphone APA app, an integral component of our APA-SM program, so patients can learn to self-administer APA. We also used ecological momentary assessment integrated into our app to measure real-world outcomes with participants able to self-monitor their progress using this as an innovative behavior change strategy. Our APA-SM program is theory-based according to Bandura’s self-efficacy model, toward successful initiation and maintenance of participants’ behavior change. In the UG3 phase, we will work with the NIH Pragmatic Trials Collaboratory Coordinating Center and collaborate extensively with our stakeholders to plan, implement, evaluate, and sustain our intervention. In the UH3 phase, using a pragmatic, randomized clinical trial, we will evaluate the clinical effectiveness of our 4-week APA-SM program. We will compare 3 groups: self-guided APA-SM, APA-SM + in-person training, and education control. The primary outcomes are pain intensity, pain interference, and function; the secondary outcomes are based on the HEAL Clinical Pain Core common data elements, and analgesic use, up to a 6-month follow-up. We will also evaluate implementation outcomes, cost-effectiveness, and predictive factors for APA-SM treatment response. A two-phase design in our UH3 will include an initiation (support for buy-in) and maintenance (no support provided) phase.
天下科研,唯快不破。
看了上述检索结果,对您有什么启发?赶快行动吧。
如果您需要HS提供类似的选题大数据分析,可阅读下面的推文:
应用这个“外挂”,张医生的选题思路源源不断、文章不断发表!
关键词: #美国基金解析;#Hanson临床科研;#Healsan医路成长
作者:Amber Wang,助理:ChatGPT
美国Healsan(恒祥医学),专长于Healsan™医学大数据分析、基于大数据的HansonCR™临床科研支持,以及MedEditing™的医学编辑服务。主要为医院科研处、生物制药公司和医生科学家提供数据分析和SCI报告,成为诸多机构的“临床科研外挂”。
网址:https://healsan.com/
点击👆;From Bench to Bedside, Healsan Paves the Path.
▼ 支持基金申请和SCI论文发表,推动临床科研的创新与发展。
基于Healsan™文献计量大数据的系列推文,全年安排如下;目前是研究热门靶点系列。
▲ 每年1-2月
▲ 每年3-4月
▲ 每年5-6月
▲ 每年7-8月
▲ 每年9-10月
▲ 每年11-12月
(点击👆图片,进入自己感兴趣的专辑)
▼ 临床科研技巧及文献更新
(点击👆图片,进入自己感兴趣的专辑。或点击“资源”,浏览本公众号所有资源)
更多高质量的医学生物科研、职业发展、及赴美访学留学推文,点击左下角“阅读原文”可见;电子邮箱注册后,可以每天免费收到高质量科研推送。
100 项与 Virbac SA 相关的药物交易
登录后查看更多信息
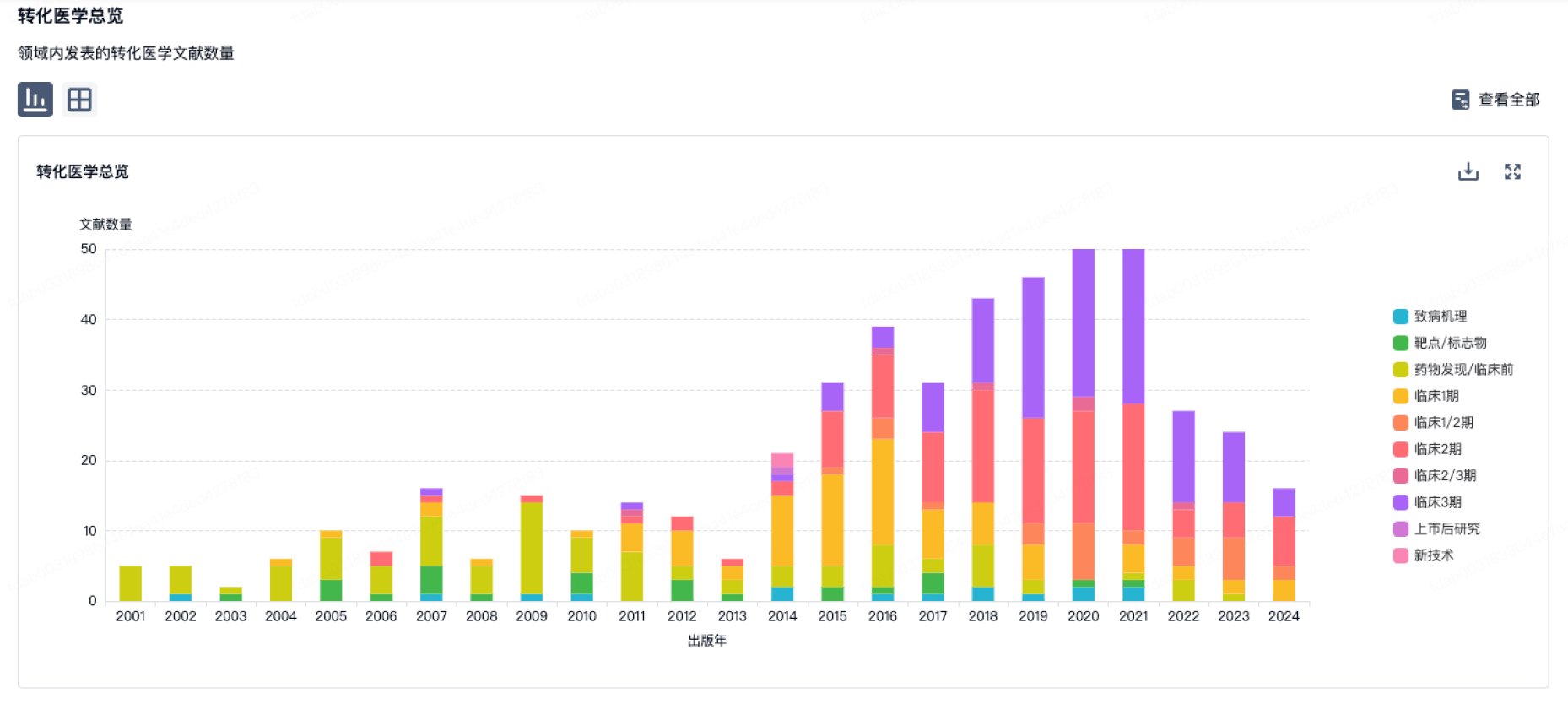
100 项与 Virbac SA 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月11日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
其他
3
登录后查看更多信息
当前项目
| 药物(靶点) | 适应症 | 全球最高研发状态 |
|---|---|---|
Vaneprim ( TGM2 ) | 细菌感染 更多 | 终止 |
Triptosine ( 5-HT receptor ) | 酗酒 更多 | 无进展 |
克伐他汀 ( HMGCR ) | 高脂血症 更多 | 无进展 |
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
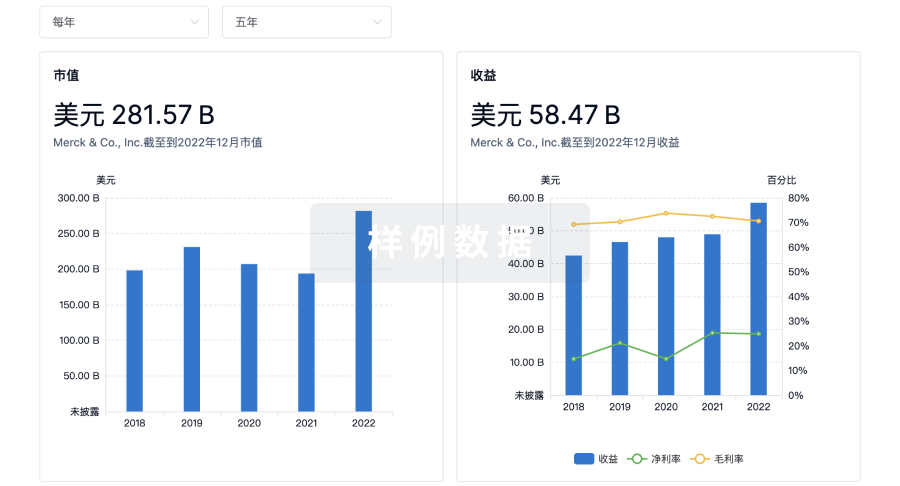
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用