预约演示
更新于:2026-04-12
Jefferson Health Corp.
更新于:2026-04-12
概览
关联
100 项与 Jefferson Health Corp. 相关的临床结果
登录后查看更多信息
0 项与 Jefferson Health Corp. 相关的专利(医药)
登录后查看更多信息
323
项与 Jefferson Health Corp. 相关的文献(医药)2026-02-01·ANNALS OF SURGICAL ONCOLOGY
Axillary Management Trends and Survival in Men Undergoing Mastectomy with Positive Sentinel Nodes
Article
作者: Bleicher, Richard J ; Whittall, Ian ; Lyons, Walker ; Shulman, Rebecca M ; Fish, Elizabeth M ; Chang, Cecilia ; Porpiglia, Andrea S ; Williams, Austin D ; So, Alycia L ; Aggon, Allison A
Abstract:
Background:
Men are often diagnosed with node-positive breast cancer and treated with mastectomy because of a lack of screening and an unfavorable tumor-to-breast ratio. The AMAROS trial showed no difference in outcomes between axillary lymph node dissection (ALND) and axillary radiation in women with cT1-2N0 breast cancer with positive sentinel lymph nodes (+SLNs). Axillary management in men remains unstandardized, so we assessed current trends and outcomes.
Methods:
Males with cT1-2N0M0 breast cancer undergoing mastectomy with one to two +SLNs were identified from the National Cancer Database (2018–2021). Patients were stratified by axillary management. Postmastectomy radiotherapy (PMRT) included chest wall and axillary fields. Management strategies and overall survival were analyzed.
Results:
Among 445 patients, 25% had no further axillary treatment, 22% underwent ALND, 29% PMRT, and 24% ALND+PMRT. Patients with two +SLNs more often underwent ALND+PMRT (43% vs. 19%,
p
< 0.001). The use of PMRT rose over time (23–36%), whereas ALND alone declined (27–12%). Additional positive nodes were found in 31% of ALND cases, with no difference between ALND and ALND+PMRT. Performance of ALND delayed PMRT (194 vs. 133 days from diagnosis,
p
< 0.001). On multivariable analysis, two +SLNs predicted ALND+PMRT (odds ratio 2.5,
p
= 0.006). Older age (
p
< 0.001) and two +SLNs (
p
= 0.03) were linked to worse overall survival, whereas axillary management was not (
p
= 0.23).
Conclusion:
Although axillary strategies are proven safe and effective in women, their extrapolation to men is inconsistent. Half of men undergoing mastectomy are undertreated or overtreated, underscoring the need for multidisciplinary consensus and prospective male-specific data to guide care and reduce morbidity.
2026-01-01·Clinical Lymphoma Myeloma & Leukemia
Survival Outcomes in Patients With Chronic Lymphocytic Leukemia: A SEER Analysis
Article
作者: Modi, Shivani ; Jain, Hardik ; Dourado, Claudia ; Rajarajan, Srinishant
SURVIVAL OUTCOMES:
Chronic lymphocytic leukemia (CLL) is the most prevalent adult leukemia. CLL treatment has evolved dramatically from alkylator-based regimens to chemoimmunotherapy and targeted therapies. This study evaluated real-world survival outcomes across treatment eras using population-based data, focusing on patients who received active systemic therapy to assess treatment effectiveness rather than natural disease progression.
METHODS:
We conducted a retrospective cohort study using surveillance, epidemiology, and end results (SEER) data from 1995 to 2020, restricting analysis to CLL patients who received active systemic treatment. Patients were stratified into three treatment eras based on treatment initiation date: Pre-novel therapy era (1995-2004, alkylator-based regimens), Early novel therapy era (2005-2014, chemoimmunotherapy with anti-CD20 monoclonal antibodies), and modern novel therapy era (2015-2020, targeted therapies including BTK inhibitors and BCL-2 inhibitors). Era boundaries accounted for the lag between regulatory approval and community adoption. Overall survival was calculated from treatment initiation date, with era assignment based on first-line therapy to maintain temporal consistency.
RESULTS:
Among 49,056 CLL patients across three treatment eras, median overall survival improved significantly from 3.5 years (95% CI, 3.2-3.8) in the pre-novel therapy era (1995-2004) to 5.2 years (95% CI, 4.9-5.6) in the early novel therapy era (2005-2014), and 7.8 years (95% CI, 6.9-8.7) in the modern novel therapy era (2015-2020). Multivariable Cox regression analysis demonstrated progressive reductions in mortality risk, with adjusted hazard ratios of 0.75 (95% CI, 0.68-0.82, P < .001) for the Early Novel era and 0.45 (95% CI, 0.38-0.53, P < .001) for the Modern era compared to the Pre-Novel era. Complete response rates increased from 15% to20% in the Pre-Novel era to over 60% in the Modern era with targeted therapies.
CONCLUSIONS:
This analysis demonstrates significant improvements in survival outcomes for CLL patients across treatment eras, with the most pronounced benefits observed in the modern targeted therapy era. By focusing on treated patients and calculating survival from treatment initiation, we isolated the impact of therapeutic advances from disease biology and patient selection factors. However, the COVID-19 pandemic's disproportionate impact on immunocompromised CLL patients, particularly affecting the modern therapy era, represents an important limitation that may underestimate the true survival benefits of contemporary targeted therapies. These findings support the continued development and adoption of novel therapeutic strategies in CLL management.
2026-01-01·JCO Global Oncology
Overcoming Logistical Barriers to Conducting Collaborative Clinical Research Between a High-Income Country and a Low- and Middle-Income Country
Article
作者: Ramogola-Masire, Doreen ; Grover, Surbhi ; Mokalake, Motseiwa ; Robertson, Erle ; Chambers, Allison ; Azoba, Chinenye ; Koyabe, Bramwell ; Jemmott, John B ; Zetola, Nicola ; Bhatia, Rohini K. ; Phaladze, Nthabiseng
PURPOSE:
Building equitable research collaborations between high-income countries (HICs) and low- and middle-income countries (LMICs) requires effective coordination among international ethical review committees, which is often logistically challenging. This case report presents the insights gained when acquiring ethical approval for a cervical cancer research program conducted jointly by the University of Pennsylvania and the University of Botswana.
METHODS:
We conducted a descriptive case study of the Ipabalele project, a 6-year HIC-LMIC partnership involving three complex research protocols that required approvals by multiple distinct ethical bodies. We analyzed various challenges affecting review procedures, timelines, and staffing. We then documented strategies employed in Ipabalele and other global initiatives to strengthen ethical review processes and build research capacity in LMICs.
RESULTS:
In Ipabalele, ethical approvals were initially delayed by 2 years because of fragmented review processes with variable timelines and conflicting recommendations. Innovations to the process included centralizing institutional review board oversight within Botswana, implementing joint virtual meetings among review bodies, enhancing digital infrastructure, and streamlining research staffing and communication.
CONCLUSION:
By providing practical strategies, this study highlights how empowered local leadership, centralized review processes, joint review mechanisms, and intentional capacity building can overcome logistical barriers in multinational ethical review.
100 项与 Jefferson Health Corp. 相关的药物交易
登录后查看更多信息
100 项与 Jefferson Health Corp. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月09日管线快照
无数据报导
登录后保持更新
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
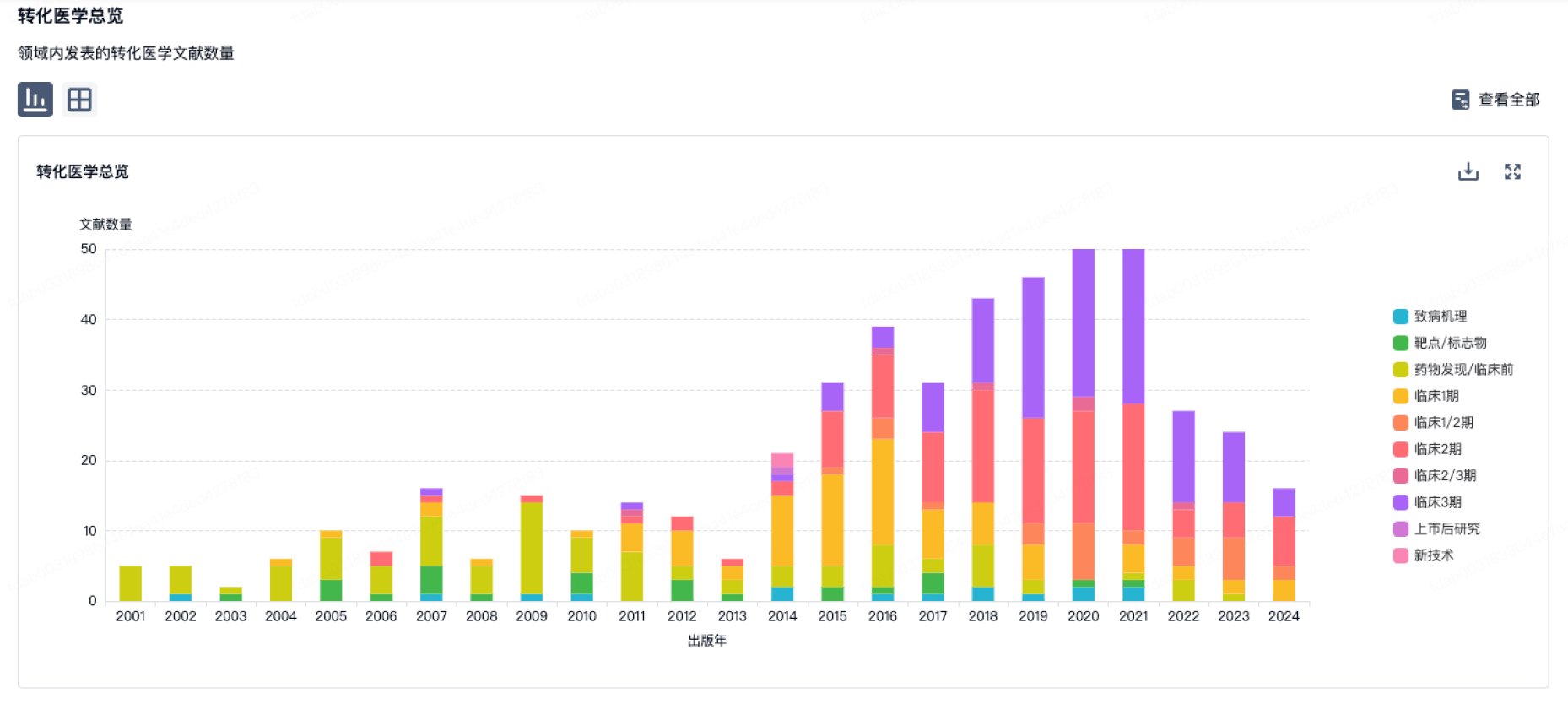
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
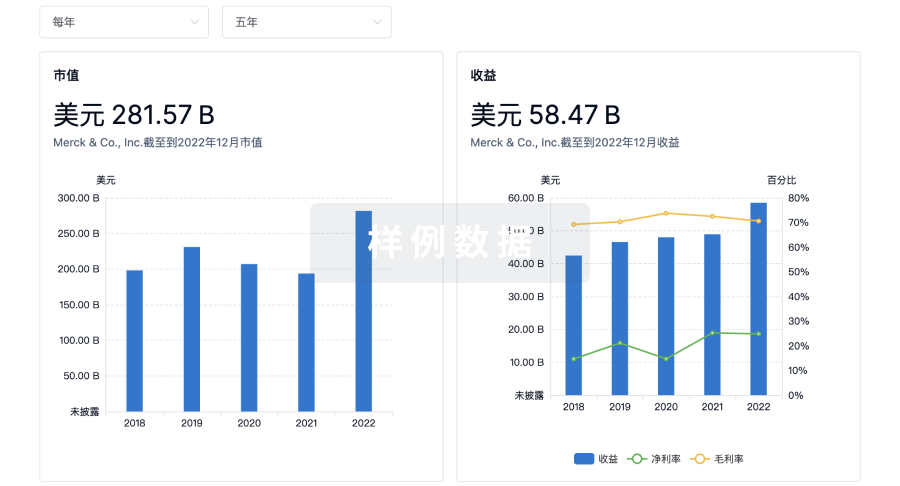
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用