预约演示
更新于:2026-03-25
Fresenius Medical Care AG
更新于:2026-03-25
概览
疾病领域得分
一眼洞穿机构专注的疾病领域

暂无数据
技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
暂无数据
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
NCT07428395
Feasibility of Intradialytic Hematocrit and Oxygen Saturation Monitoring During Continuous Kidney Replacement Therapy
NCT07004907
Efficacy and Tolerability of the APD Treatment of Toddlers and Newborns With the Silencia PD Cycler
NCT06341452
Comparison of Individualized Sodium Management Versus Standard Treatment in Hemodialysis
100 项与 Fresenius Medical Care AG 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2026-03-01AMERICAN JOURNAL OF KIDNEY DISEASES
Optimizing Comprehensive Medication Management in CKD: An Opportunity to Integrate Pharmacists in the Kidney Care Team
Review
作者: Condon Martinez, Amanda J ; St Peter, Wendy L ; Maxson, Rebecca ; Meaney, Calvin J ; Hudson, Joanna Q ; Chang, Alex R
Comprehensive medication management (CMM) is the standard of care that ensures that medications are individually assessed to determine that each medication is appropriate, effective for the medical condition, safe given the patient's comorbidities and other medications, and able to be taken by the patient as intended. CMM helps improve all aspects of health care quality and is essential for individuals with chronic kidney disease. It specifically addresses the complexity of medication regimens in patients with multiple comorbid conditions that often lead to medication therapy problems. The provision of CMM is best optimized with a multidisciplinary team that includes a pharmacist. The importance of interprofessional and multidisciplinary practice in the care of individuals with kidney disease has been emphasized by nephrology organizations and within chronic kidney disease-related guidelines. The shift toward pay for performance and value-based care models within nephrology has created more opportunities for pharmacist integration into care teams. Other health care providers should view the inclusion of pharmacists in the kidney care team as a valuable opportunity to enhance patient support, reduce work-related stress, and improve outcomes through collaborative teamwork. The Advancing Kidney Health through Optimal Medication Management initiative supports the involvement of pharmacists across practices and health care systems to ensure the successful implementation of CMM for individuals with kidney disease.
2026-01-01Clinical Journal of the American Society of Nephrology
Characteristics of Populations Included in Randomized Controlled Trials of Hemodiafiltration and Registry Real-Life Populations
Article
作者: Hegbrant, Jörgen ; Barth, Claudia ; Canaud, Bernard ; Yuen, Tom ; Pham, Ngoc ; Bots, Michiel L. ; Davenport, Andrew ; Rose, Matthias ; Cromm, Krister ; Blankestijn, Peter J. ; Strippoli, Giovanni F.M. ; Woodward, Mark ; Jaha, Hanna ; Saglimbene, Valeria
Key Points:
Coverage of patient characteristics in existing trials of hemodiafiltration versus hemodialysis seems to be broad but incomplete.Randomized trials of hemodiafiltration versus hemodialysis have been primarily limited to Europe.Inconsistencies between trials and registries support further studies using real-world data to explore applicability of existing evidence.
Background:
Selection criteria in randomized trials (randomized controlled trials [RCTs]) can lead to differences in key characteristics between trial participants and real-life populations. We evaluated reporting of population characteristics in existing RCTs of hemodiafiltration (HDF) and in real-life populations included in kidney registries to descriptively identify key differences.
Methods:
We used systematic review methodology to identify existing RCTs of HDF versus hemodialysis (1966 to May 2024). We also searched the Fresenius Quantitative Market Analysis team registry database (2024 update) for existing registries from Europe, the Asia-Pacific region, and America including populations on HDF. Patient characteristics from RCTs and registries were extracted, summarized, and compared descriptively.
Results:
Eleven RCTs (
N
=5108) and eight registries (
N
=1,147,167) were identified. There were no RCTs in the United States and only two small RCTs from Australia (
N
=124) and Brazil (
N
=195). Most trials were from Europe. Key characteristics consistently reported in both RCTs and registries were only age, sex, diabetes, cardiovascular disease, vascular access type, and dialysis vintage. There was moderate to high heterogeneity for these patient characteristics in RCTs, indicating enrollment of a broad array of people. The proportion of people with diabetes was 26% in RCTs and 43% in registries. The prevalence of arteriovenous fistulas/graft was 90% in RCTs and 70% in registries.
Conclusions:
There was a broad but incomplete array of patient characteristics in existing RCTs and real-world registries of HDF versus hemodialysis. Data were primarily limited to Europe and only a core set of demographic and clinical variables. Apart for age, sex, diabetes, cardiovascular disease, vascular access type, and dialysis vintage, other patient and treatment relevant characteristics were erratically or not at all reported in RCTs as well as in real-world registries. With potential differences in patient populations, we support the need for studies examining HDF in real-world settings,
e.g
., with target emulation trials.
2025-11-26NEPHROLOGY DIALYSIS TRANSPLANTATION
Effect of haemodialysis on the brain and heart assessed using multiparametric MRI
Article
作者: Nicholas, Rosemary ; Buchanan, Charlotte E ; Taal, Maarten W ; Francis, Susan T ; Selby, Nicholas M ; Gullapudi, Venkata Rukmini Latha ; Cox, Eleanor F ; Canaud, Bernard ; White, Kelly
ABSTRACT:
Background and hypothesis:
Haemodialysis (HD) patients often develop cognitive impairment, negatively impacting health-related quality of life. We use brain magnetic resonance imaging (MRI) measures to study the acute changes in cerebral water content during HD, alongside chronic changes in HD patients compared with healthy volunteers (HVs) to assess whether the brain changes associated with ageing develop more rapidly in HD patients (‘accelerated brain ageing’). We also study associated cardiac MRI measures.
Methods:
3T MRI scans were performed during HD in 12 patients to characterize the acute effect of HD on cerebral water content (T1 mapping), alongside previously reported results from the HD-REMODEL (HaemoDialysis interventions to REduce MultiOrgan Dysfunction and Effect on quality of Life assessed by MRI scanning) trial. MRI changes in brain structure [volumes and T1 of white (WM) and grey matter (GM), WM diffusion fractional anisotropy (FA) and mean diffusivity (MD)], perfusion, blood flow, and cardiac measures were compared between HD patients pre-dialysis and HVs (age and gender matched).
Results:
WM T1 increased during HD (3.8 ± 1.7%, P = .0005). GM and WM volume [total intracranial volume (TIV)-corrected] were lower in HD compared with HVs [GM volume/TIV: 0.37 (0.34–0.41) vs 0.42 (0.42–0.44), WM volume/TIV: 0.34 ± 0.03 vs 0.37 ± 0.01, P = .009]. In HD, FA was lower and MD higher than HVs (FA: 0.32 ± 0.02 vs 0.35 ± 0.01, MD: 0.59 ± 0.03 vs 0.53 ± 0.01, P < .0001). Higher MD and lower FA was seen in older participants, with steeper slopes in HD (MD: 0.003 vs 0.0006 × 10−3 mm2/s/year P = .003, FA: –0.001 vs –0.0003 units/year P < .0001), suggestive of accelerated ageing. There were no differences between groups in age-related heart changes.
Conclusions:
An acute increase in WM T1 during HD has been shown for the first time, reflecting a rise in brain water content. This is potentially caused by the development of an osmotic gradient across the blood–brain barrier due to slower diffusion of urea, and may contribute to acute symptoms and chronic pathological changes contributing to accelerated brain ageing in HD patients.
2026-03-18
·医药健闻
2026-03-18
财报临床1期

100 项与 Fresenius Medical Care AG 相关的药物交易
登录后查看更多信息
100 项与 Fresenius Medical Care AG 相关的转化医学
登录后查看更多信息
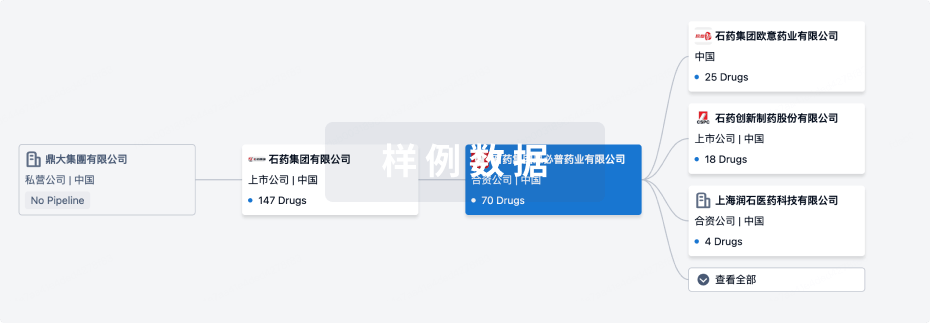
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月08日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
批准上市
1
3
其他
登录后查看更多信息
当前项目
登录后查看更多信息
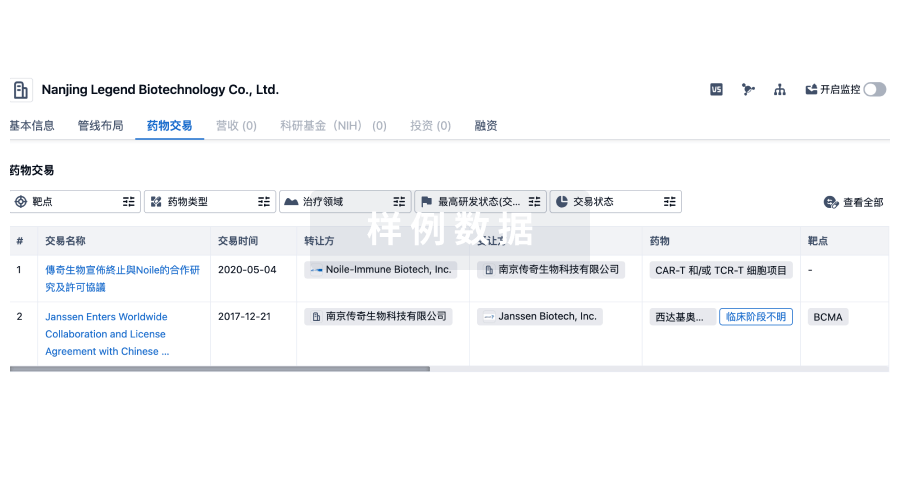
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
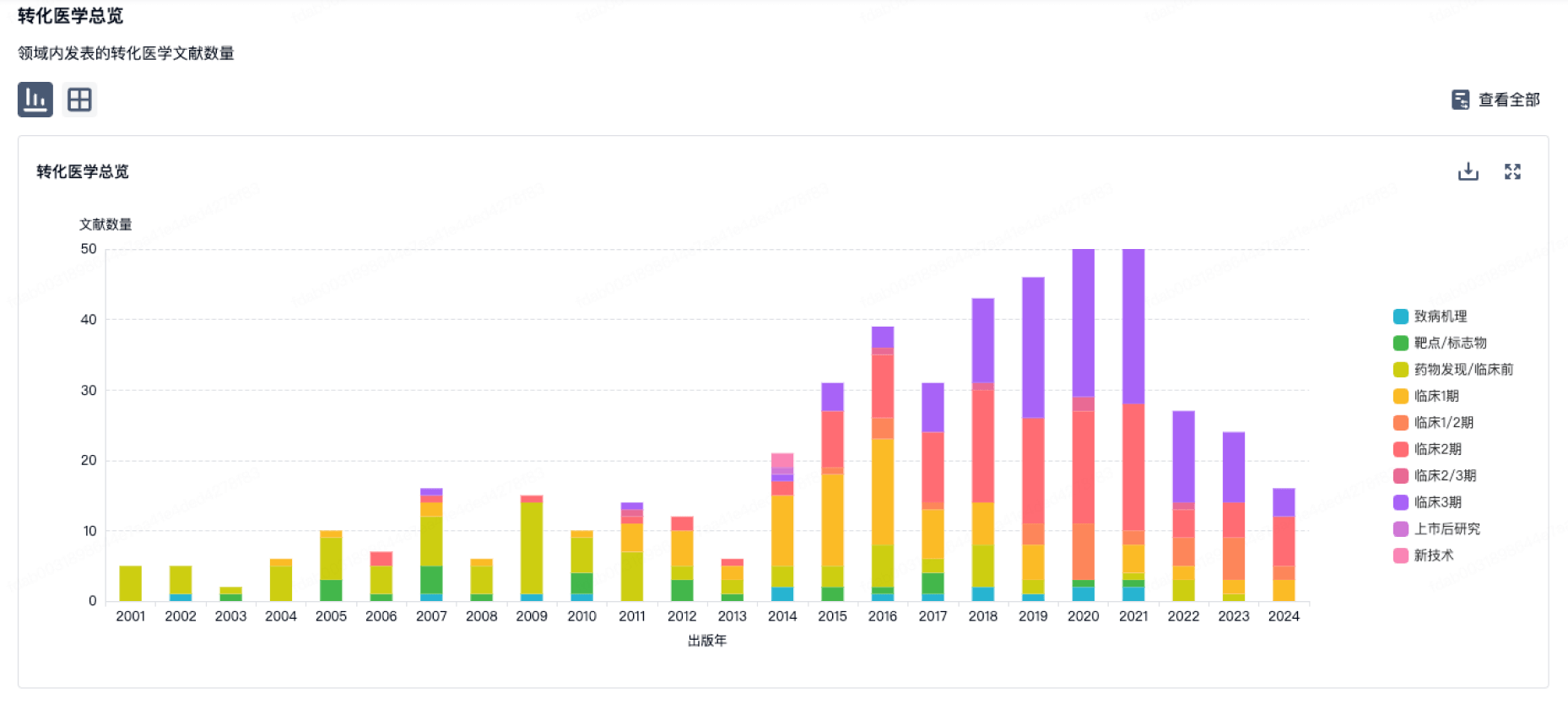
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
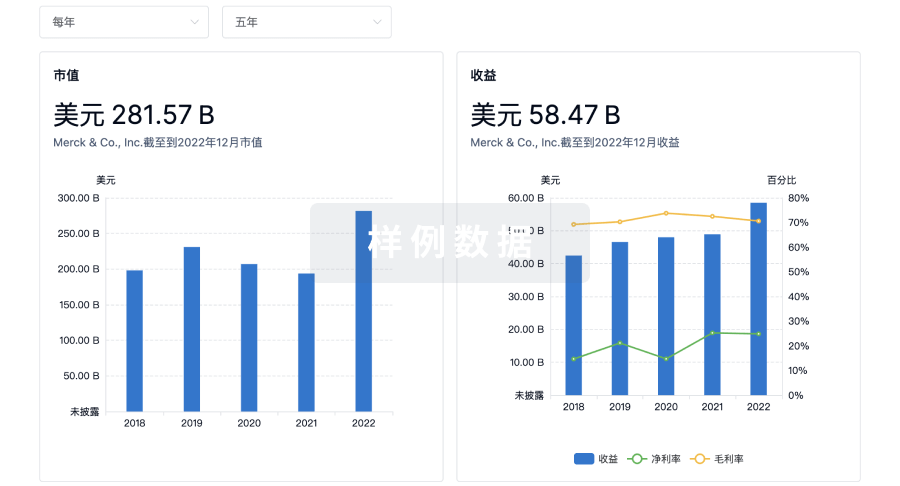
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用