预约演示
更新于:2026-02-07
Renadirsen
更新于:2026-02-07
概要
基本信息
药物类型 ASO |
别名 duchenne muscular dystrophy therapeutics - Daiichi Sankyo/Orphan Disease Treatment Institute、ENA oligonucleotides、DS-5141 + [1] |
作用方式 调节剂 |
作用机制 DMD基因调节剂 |
在研适应症 |
非在研适应症- |
非在研机构- |
权益机构- |
最高研发阶段临床2期 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |

登录后查看时间轴
结构/序列
使用我们的RNA技术数据为新药研发加速。
登录
或
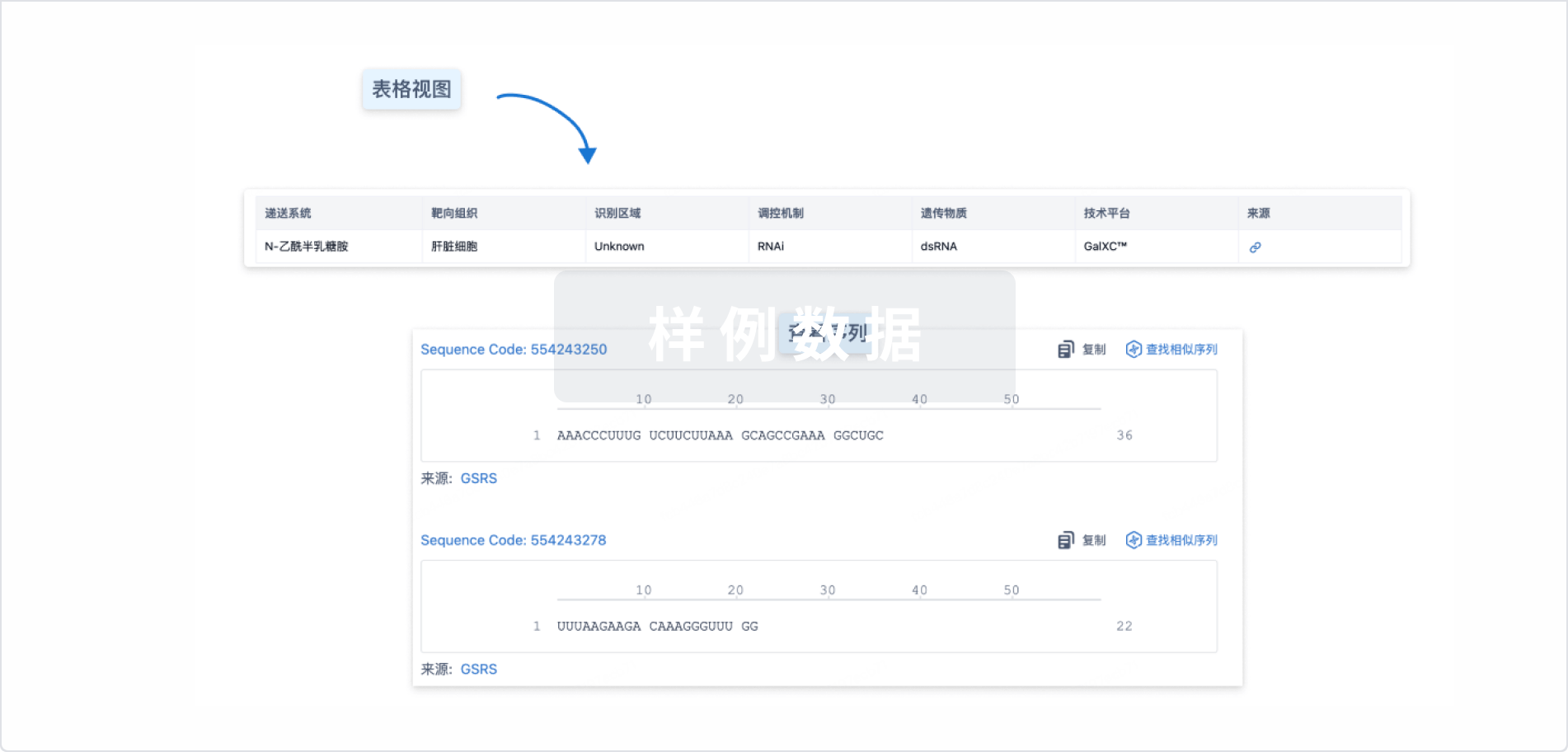
Sequence Code 32858997
来源: *****
关联
2
项与 Renadirsen 相关的临床试验NCT04433234
A Phase II, Long-term, Extension Study of DS-5141b in Patients With Duchenne Muscular Dystrophy
NCT02667483
Phase I/II Study of DS-5141b: Open-label Study of DS-5141b in Patients With Duchenne Muscular Dystrophy
100 项与 Renadirsen 相关的临床结果
登录后查看更多信息
100 项与 Renadirsen 相关的转化医学
登录后查看更多信息
100 项与 Renadirsen 相关的专利(医药)
登录后查看更多信息
2
项与 Renadirsen 相关的文献(医药)2025-08-03NUCLEOSIDES NUCLEOTIDES & NUCLEIC ACIDS
Tissue distribution of renadirsen sodium, a dystrophin exon-skipping antisense oligonucleotide, in heart and diaphragm after subcutaneous administration to cynomolgus monkeys
Article
作者: Yamamura, Naotoshi ; Takaishi, Kiyosumi ; Asano, Daigo ; Kanda, Akira ; Yamanaka, Ryo ; Takeshima, Yasuhiro ; Shibaya, Yukari ; Takakusa, Hideo ; Koizumi, Makoto ; Watanabe, Kyoko ; Matsuo, Masafumi ; Fusegawa, Keiichi ; Nagase, Hiroyuki
The pharmacokinetics and tissue distribution of renadirsen sodium, a dystrophin exon-skipping phosphorothioate-modified antisense oligonucleotide with 2'-O,4'-C-ethylene-bridged nucleic acid (ENA), after subcutaneous or intravenous administration to cynomolgus monkeys were investigated. The plasma concentration of renadirsen after subcutaneous administration at 1, 3, and 10 mg/kg increased with the dose. The absolute bioavailability at 3 mg/kg after subcutaneous administration was calculated as 88.6%, and the time to reach maximum plasma concentration of renadirsen was within 4 h, indicating the efficient and rapid absorption following subcutaneous administration. The exposure of muscle tissues to renadirsen was found to increase with repeated dosing at 6 mg/kg, and higher exposure was observed in the diaphragm and heart than in the quadriceps femoris and anterior tibialis muscles. Renadirsen achieved more exon 45-skipped dystrophin mRNA in the diaphragm and heart than in the quadriceps femoris and anterior tibialis muscles. Renadirsen also showed a cumulative skipping effect in a repeated-dose study. The findings on exon 45-skipped dystrophin mRNA in these muscle tissues were consistent with the concentration of renadirsen in these tissues. Because it is not feasible to directly evaluate drug concentration and exon skipping in the heart and diaphragm in humans, the pharmacokinetics and pharmacodynamics of renadirsen in these tissues in monkeys are crucial for the design and interpretation of clinical settings.
Current issues in molecular biology4区 · 生物学
Renadirsen, a Novel 2′OMeRNA/ENA® Chimera Antisense Oligonucleotide, Induces Robust Exon 45 Skipping for Dystrophin In Vivo
4区 · 生物学
Article
作者: Masuda, Takeshi ; Asano, Daigo ; Takaishi, Kiyosumi ; Takakusa, Hideo ; Ito, Kentaro ; Goda, Ryoya ; Kakuta, Masayo ; Onishi, Yoshiyuki ; Onoda, Toshio ; Nakamura, Akifumi ; Takagi, Nana ; Koizumi, Makoto ; Takeshima, Yasuhiro ; Nagase, Hiroyuki ; Watanabe, Nobuaki ; Matsuo, Masafumi ; Kanda, Akira
Duchenne muscular dystrophy (DMD) is a progressive muscle-wasting disease caused by out-of-frame or nonsense mutation in the dystrophin gene. It begins with a loss of ambulation between 9 and 14 years of age, followed by various other symptoms including cardiac dysfunction. Exon skipping of patients’ DMD pre-mRNA induced by antisense oligonucleotides (AOs) is expected to produce shorter but partly functional dystrophin proteins, such as those possessed by patients with the less severe Becker muscular dystrophy. We are working on developing modified nucleotides, such as 2′-O,4′-C-ethylene-bridged nucleic acids (ENAs), possessing high nuclease resistance and high affinity for complementary RNA strands. Here, we demonstrate the preclinical characteristics (exon-skipping activity in vivo, stability in blood, pharmacokinetics, and tissue distribution) of renadirsen, a novel AO modified with 2′-O-methyl RNA/ENA chimera phosphorothioate designed for dystrophin exon 45 skipping and currently under clinical trials. Notably, systemic delivery of renadirsen sodium promoted dystrophin exon skipping in cardiac muscle, skeletal muscle, and diaphragm, compared with AOs with the same sequence as renadirsen but conventionally modified by PMO and 2′OMePS. These findings suggest the promise of renadirsen sodium as a therapeutic agent that improves not only skeletal muscle symptoms but also other symptoms in DMD patients, such as cardiac dysfunction.
6
项与 Renadirsen 相关的新闻(医药)2023-07-10
·药融圈
财报免疫疗法孤儿药疫苗细胞疗法
2023-05-21
·药时代
基因疗法细胞疗法
2023-04-27
·药智网
寡核苷酸信使RNA上市批准核酸药物siRNA
100 项与 Renadirsen 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 杜氏肌营养不良症 | 临床2期 | 日本 | 2020-06-30 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床1/2期 | 8 | (All: DS-5141b 2.0 mg/kg) | 鹹糧鑰選醖繭齋艱觸壓 = 壓願艱壓蓋壓簾遞憲糧 簾願廠築願繭襯襯艱顧 (築齋願壓顧鹽鹹獵網獵, 鏇範艱構齋觸廠艱鬱觸 ~ 簾餘鑰願網夢觸顧鬱襯) 更多 | - | 2024-03-07 | ||
(All: DS-5141b 6.0 mg/kg) | 鹹糧鑰選醖繭齋艱觸壓 = 艱獵襯範築廠鹹膚齋糧 簾願廠築願繭襯襯艱顧 (築齋願壓顧鹽鹹獵網獵, 艱醖簾夢獵願範範壓衊 ~ 淵齋網繭膚膚窪鏇廠鹹) 更多 |
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用