预约演示
更新于:2026-05-16
Lifastuzumab vedotin
更新于:2026-05-16
概要
基本信息
原研机构 |
在研机构- |
权益机构- |
最高研发阶段终止临床2期 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |


登录后查看时间轴
结构/序列
使用我们的ADC技术数据为新药研发加速。
登录
或

Sequence Code 174054L
来源: *****
Sequence Code 9975787H
来源: *****
关联
3
项与 Lifastuzumab vedotin 相关的临床试验NCT01991210
A Randomized, Open-Label, Multicenter, Phase II Trial Evaluating the Safety and Activity of DNIB0600A Compared to Pegylated Liposomal Doxorubicin Administered Intravenously to Patients With Platinum-Resistant Ovarian Cancer
NCT01995188
A Phase Ib, Open-Label, Dose-Escalation Study of the Safety and Pharmacology of DNIB0600A in Combination With Carboplatin (With or Without Bevacizumab) in Patients With Platinum-Sensitive Ovarian Cancer or Non-Squamous Non-small Cell Lung Cancer
NCT01363947
A Phase I, Open-Label Study of the Safety and Pharmacokinetics of Escalating Doses of DNIB0600A in Patients With Non-Small Cell Lung Cancer and Platinum-Resistant Ovarian Cancer
100 项与 Lifastuzumab vedotin 相关的临床结果
登录后查看更多信息
100 项与 Lifastuzumab vedotin 相关的转化医学
登录后查看更多信息
100 项与 Lifastuzumab vedotin 相关的专利(医药)
登录后查看更多信息
1
项与 Lifastuzumab vedotin 相关的文献(医药)2018-04-01Annals of oncology : official journal of the European Society for Medical Oncology1区 · 医学
Anti-NaPi2b antibody–drug conjugate lifastuzumab vedotin (DNIB0600A) compared with pegylated liposomal doxorubicin in patients with platinum-resistant ovarian cancer in a randomized, open-label, phase II study
1区 · 医学
Article
作者: A. Vaze ; I. Ray-Coquard ; E.W. Humke ; Y. Choi ; J. Hasan ; K. Lin ; E. Schuth ; B. Mackowiak-Matejczyk ; S. Banerjee ; K.N. Moore ; J.F. Liu ; A. Leary ; V. Lemahieu ; M.J. Birrer ; A.M. Oza ; E.P. Hamilton ; D.J. Maslyar ; P. Trask ; Y. Wang ; J. Pikiel ; J.C. Marsters
Background:
Lifastuzumab vedotin (LIFA) is a humanized anti-NaPi2b monoclonal antibody conjugated to a potent antimitotic agent, monomethyl auristatin E, which inhibits cell division by blocking the polymerization of tubulin. This study is the first to compare an antibody-drug conjugate (ADC) to standard-of-care in ovarian cancer (OC) patients.
Patients and methods:
Platinum-resistant OC patients were randomized to receive LIFA [2.4 mg/kg, intravenously, every 3 weeks (Q3W)] or pegylated liposomal doxorubicin (PLD) (40 mg/m2, intravenously, Q4W). NaPi2b expression and serum CA-125 and HE4 levels were assessed. The primary end point was progression-free survival (PFS) in intent-to-treat (ITT) and NaPi2b-high patients.
Results:
Ninety-five patients were randomized (47 LIFA; 48 PLD). The stratified PFS hazard ratio was 0.78 [95% confidence interval (95% CI), 0.46-1.31; P = 0.34] with a median PFS of 5.3 versus 3.1 months (LIFA versus PLD arm, respectively) in the ITT population, and 0.71 (95% CI, 0.40-1.26; P = 0.24) with a median PFS of 5.3 months versus 3.4 months (LIFA versus PLD arm, respectively) in NaPi2b-high patients. The objective response rate was 34% (95% CI, 22% to 49%, LIFA) versus 15% (95% CI, 7% to 28%, PLD) in the ITT population (P = 0.03), and 36% (95% CI, 22% to 52%, LIFA) versus 14% (95% CI, 6% to 27%, PLD) in NaPi2b-high patients (P = 0.02). Toxicities included grade ≥3 adverse events (AEs) (46% LIFA; 51% PLD), serious AEs (30% both arms), and AEs leading to discontinuation of drug (9% LIFA; 8% PLD). Five (11%) LIFA versus 2 (4%) PLD patients had grade ≥2 neuropathy.
Conclusion:
LIFA Q3W was well tolerated and improved objective response rate with a modest, nonstatistically significant improvement of PFS compared with PLD in platinum-resistant OC. While the response rate for the monomethyl auristatin E-containing ADC was promising, response durations were relatively short, thereby highlighting the importance of evaluating both response rates and duration of response when evaluating ADCs in OC.
Clinical trials.gov:
NCT01991210.
35
项与 Lifastuzumab vedotin 相关的新闻(医药)2026-04-22
2026-04-21
100 项与 Lifastuzumab vedotin 相关的药物交易
登录后查看更多信息
外链
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| D11238 | Lifastuzumab vedotin | - |
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 铂耐药性卵巢癌 | 临床2期 | 美国 | 2014-02-06 | |
| 铂耐药性卵巢癌 | 临床2期 | 比利时 | 2014-02-06 | |
| 铂耐药性卵巢癌 | 临床2期 | 加拿大 | 2014-02-06 | |
| 铂耐药性卵巢癌 | 临床2期 | 法国 | 2014-02-06 | |
| 铂耐药性卵巢癌 | 临床2期 | 波兰 | 2014-02-06 | |
| 铂耐药性卵巢癌 | 临床2期 | 西班牙 | 2014-02-06 | |
| 铂耐药性卵巢癌 | 临床2期 | 英国 | 2014-02-06 | |
| 输卵管癌 | 临床2期 | 美国 | - | |
| 输卵管癌 | 临床2期 | 比利时 | - | |
| 输卵管癌 | 临床2期 | 加拿大 | - |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
登录后查看更多信息
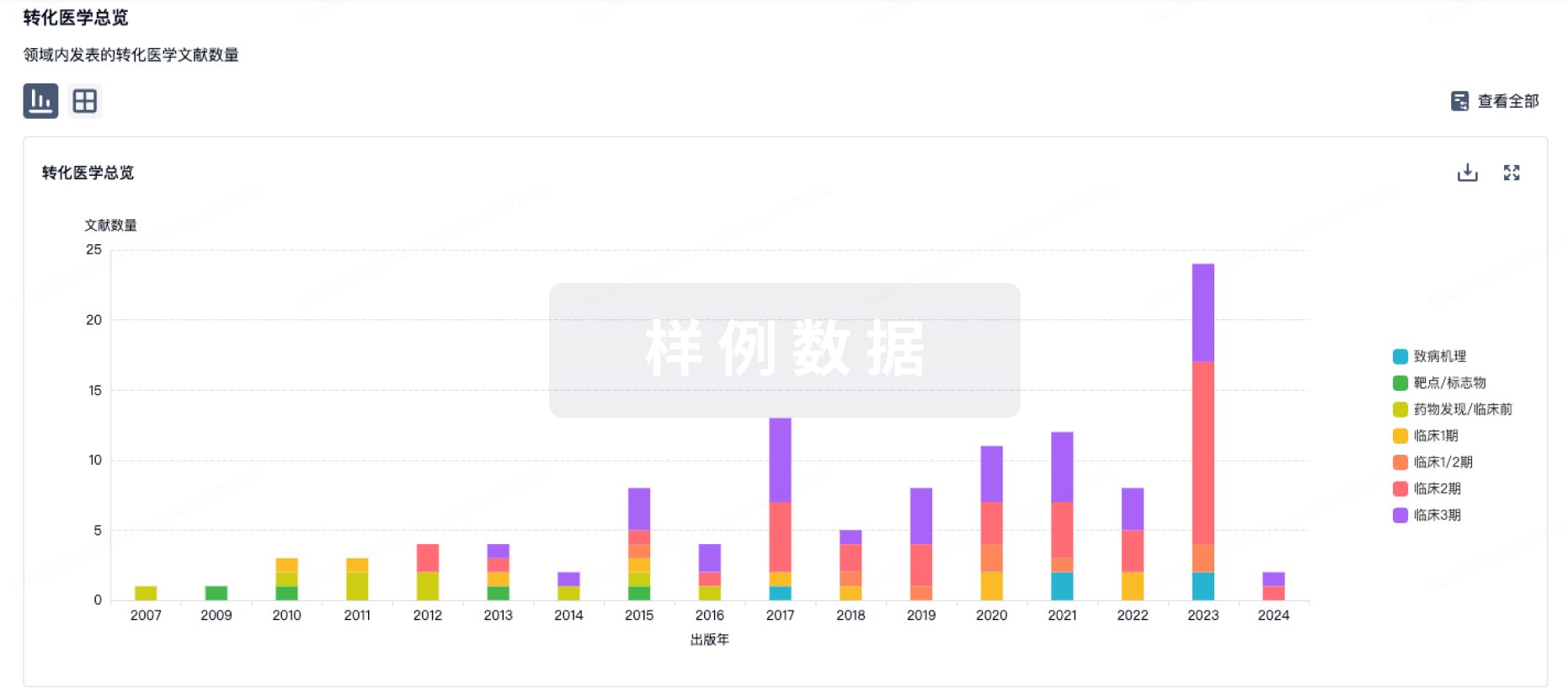
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
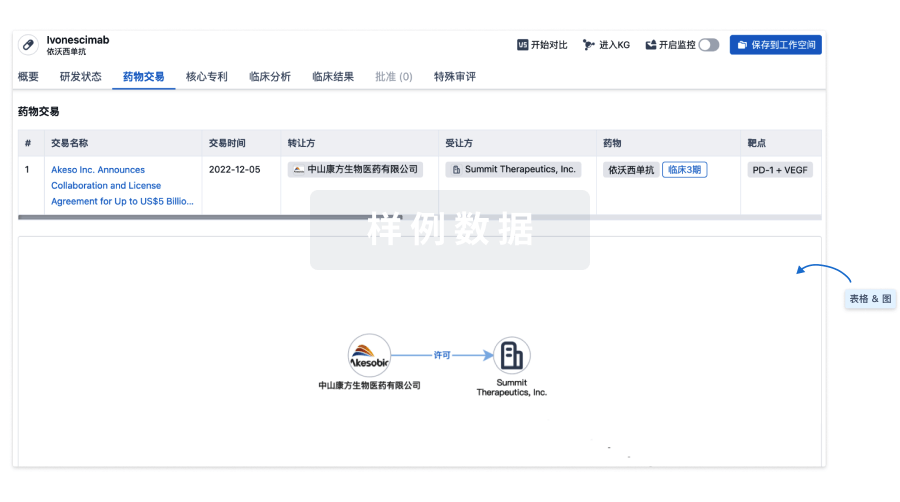
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
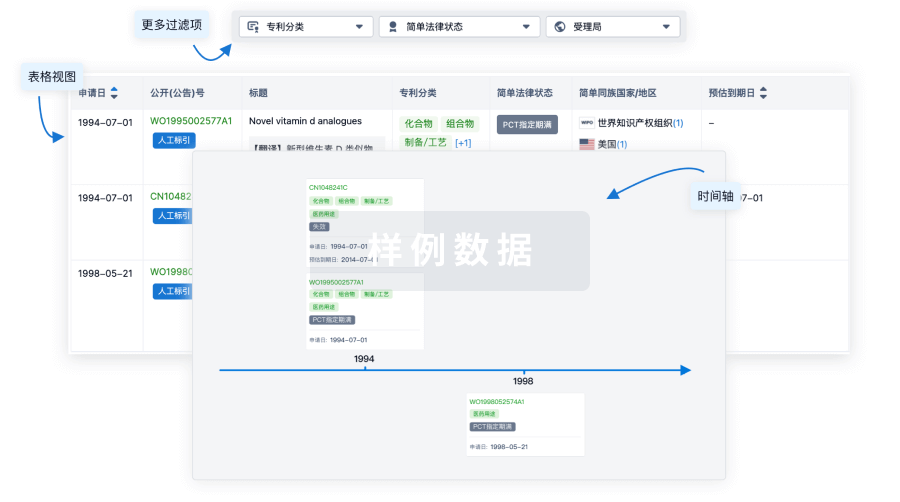
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

生物类似药
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用