预约演示
更新于:2026-05-30
JAK Inhibitor (Alcon)
JAK抑制剂(爱尔康制药)
更新于:2026-05-30
概要
基本信息
关联
100 项与 JAK抑制剂(爱尔康制药) 相关的临床结果
登录后查看更多信息
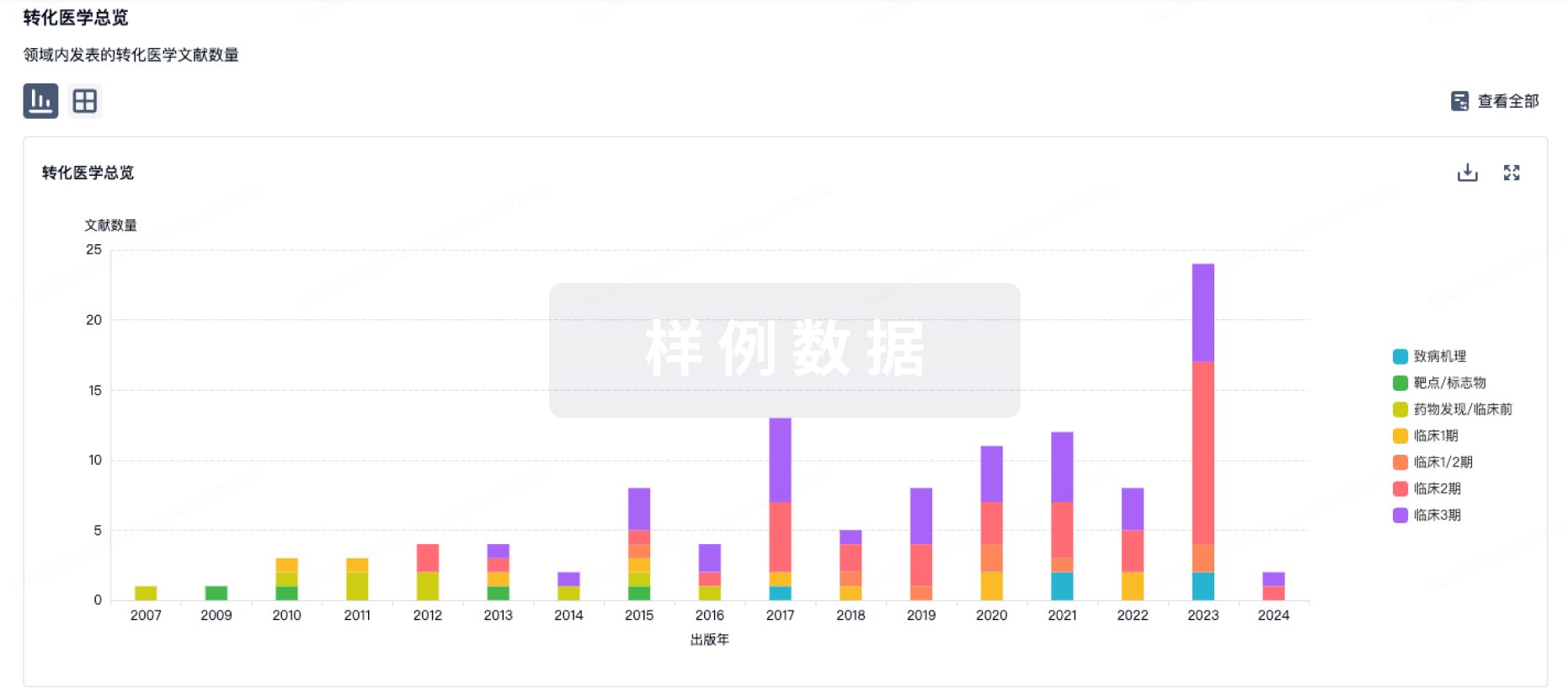
100 项与 JAK抑制剂(爱尔康制药) 相关的转化医学
登录后查看更多信息
100 项与 JAK抑制剂(爱尔康制药) 相关的专利(医药)
登录后查看更多信息
82
项与 JAK抑制剂(爱尔康制药) 相关的文献(医药)2026-04-01·JOURNAL OF CONTROLLED RELEASE
Formulation and administration timing of lipid derivatized JAK-inhibitor and corticosteroid modulate saRNA-LNP inflammation and expression
Article
作者: Tam, Yuen Yi C ; Li, Shyh-Dar ; Chen, Sam ; Casmil, Irafasha C ; Lai, Mei-Jung ; Liao, Suiyang ; Blakney, Anna K ; Maiti, Bappa ; Friesen, Josh J ; Liou, Jing-Ping ; Yuan, Endger ; Bathula, Nuthan Vikas
Self-amplifying RNA (saRNA)-lipid nanoparticle (LNP) therapeutics represent a transformative advance in nucleic acid medicine, enabling prolonged protein expression at significantly lower doses compared to traditional mRNA-LNP systems. However, their broader clinical translation is hindered by pronounced innate immune activation elicited by saRNA replication intermediates and LNP components. To address this challenge, we investigated lipid-derivatized prodrugs of peficitinib (a pan-JAK inhibitor) and dexamethasone (a corticosteroid) for their ability to modulate saRNA-LNP induced inflammation. Using both in vitro and in vivo models, we optimized the formulation strategy, including evaluating co-formulation within the same LNPs and independent formulation into separate LNPs, as well as varied timing of administration. Our findings demonstrate that co-formulation of peficitinib exacerbated the endosomal damage signaling and downstream defence pathways, abrogating saRNA replication and expression despite suppressing innate immune activation. By contrast, independent delivery delayed these responses by a few hours, preserving saRNA replication and expression while still mitigating inflammation. Collectively, these results emphasise that the formulation strategy, and timing - not drug identity alone, influence the trade-off between controlling reactogenicity and maintaining transgene expression, offering a refined pathway toward reducing reactogenicity while maximizing the therapeutic potential of saRNA-LNP therapeutics.
2026-02-01·Clinical Gastroenterology and Hepatology
Janus Kinase Inhibitor-Induced Acne in Inflammatory Bowel Disease: An International, Multicenter, Retrospective Cohort Study
Article
作者: Gututui, Madalina ; Lukáš, Milan ; Vieujean, Sophie ; Kuzhiyanjal, Anish John Kuriakose ; Fernandes, Rita ; Honap, Sailish ; Uzzan, Mathieu ; Digby-Bell, Jonathan ; Hart, Ailsa ; Shields, Natalie ; Pavlidis, Polychronis ; Sebastian, Shaji ; Neves, Joana Camões ; Kobayashi, Taku ; Badrulhisham, Fakhirah ; Spencer, Ashley ; Baillie, Samantha ; Peyrin-Biroulet, Laurent ; McBride, Jodie ; Nancey, Stephane ; Thompson, Ellen ; Temido, Maria José ; Jama, Amina ; Chai, Ningyu ; Shakweh, Eathar ; Simão, Inês ; Parkes, Gareth C ; D'Amico, Ferdinando ; Estevinho, Maria Manuela ; Limdi, Jimmy ; Bergereau, Emilie ; Magro, Fernando ; Wegener, Birte-Antina ; Mendes, João Martins ; Mehta, Sonia ; O'Neill, Catarina ; Fumery, Mathurin ; Din, Shahida ; Nogami, Akira
BACKGROUND & AIMS:
JAK inhibitor-associated acne is a common but poorly understood adverse event. This study aimed to investigate the epidemiology, clinical characteristics, and treatment outcomes of this condition in patients with inflammatory bowel disease (IBD).
METHODS:
This international, multicenter, retrospective cohort study consecutively enrolled JAK-inhibitor-treated patients with IBD who subsequently developed acne. The primary objective was to evaluate the clinical characteristics of acne. Secondary objectives included determining acne prevalence, impact on quality of life, and antiacne treatment effectiveness.
RESULTS:
Among 2183 JAK inhibitor-treated patients with IBD, 272 developed acne. The crude prevalence rates of acne were 15.9% for upadacitinib, 4.3% for tofacitinib, and 1.9% for filgotinib, with dose-dependent relationships observed for upadacitinib and tofacitinib. Acne predominantly affected patients aged 30-50 years; most cases were mild-moderate in severity. A prior history of acne vulgaris was associated with significantly increased odds of developing severe JAK inhibitor-associated acne (odds ratio, 4.88; 95% confidence interval, 2.88-31.7; P = .0003) and acne-related skin complications (odds ratio, 3.92; 95% confidence interval, 1.56-10.11; P = .004). One-third of patients reported a negative psychosocial impact, and 40% received pharmacologic intervention. Eighteen percent of patients who developed acne required JAK inhibitor dose reduction or discontinuation, although most did not have severe disease.
CONCLUSIONS:
This is the first study characterizing this adverse event in JAK inhibitor-treated patients with IBD and presents the largest cohort of JAK inhibitor-induced acne cases across all immune-mediated diseases. Acne is a common adverse effect resulting in significant psychological burden. Early identification, proactive counseling, and timely interventions, such as dose reduction or referral to dermatology, are crucial in managing this side effect.
2026-02-01·ALIMENTARY PHARMACOLOGY & THERAPEUTICS
Meta‐Analysis: Improvement of Bowel Urgency With Advanced Therapies for Inflammatory Bowel Disease
Review
作者: Narula, Neeraj ; Tandon, Parul ; Rai, Nitin Shiv ; Yuan, Yuhong ; Belesiotis, Peter ; Sasson, Alexa ; Ma, Christopher ; Jairath, Vipul ; Patel, Purab ; Cino, Maria
ABSTRACT:
Background:
Inflammatory bowel diseases (IBD) are chronic conditions that significantly affect quality of life. Bowel urgency, a particularly disruptive symptom of IBD, is often underreported in clinical trials.
Aims:
To examine the effects of IBD therapies on bowel urgency (BU), focusing on the degree and durability of improvement.
Methods:
We searched MEDLINE, Embase, and Cochrane databases in December 2024 for studies that reported a BU outcome for IBD therapies. We included only those studies that reported the absence of BU as a quantitative, binary outcome in the meta‐analysis. We also performed a subgroup analysis by IBD subtype. We report risk ratios (RR) with 95% confidence intervals (CI).
Results:
We included 29 randomised controlled trials (RCTs) and 15
post hoc
studies of RCTs representing eight therapeutic agents. There was significantly improved likelihood of BU remission across all induction (RR 1.77, CI 1.51–2.08) and maintenance (RR 2.40, CI 1.54–3.73) therapies compared to placebo, and no major differences between anti‐interleukin‐23 agents (risankizumab, mirikizumab, guselkumab) and a JAK‐inhibitor (upadacitinib).
Conclusions:
Advanced IBD therapies with different mechanisms of action produce rapid and sustained improvement in BU. The degree of BU improvement was similar among agents. Areas for future research include investigation of BU outcomes with other IBD therapies, exploration of underlying mechanisms of action, and greater standardisation for measuring BU through validated scores.
4,208
项与 JAK抑制剂(爱尔康制药) 相关的新闻(医药)2026-05-29
·雪球
楼主写得很详细,目前先声还亏10个点,不知道什么时候能反弹下@小刘鸭埃里克前言:不构成购买建议,我从来没买过先声的股票,这篇文章只是我研究创新药的研究框架,不构成投资建议,别在这文章底下问我“老师,XX药业帮我看下,多少钱能不能买?”,我不是你们丫的医疗许愿池最近我在全力梭哈押注能源危机,我的主仓是海油神火,只是这种票最近行情无聊得等,毕竟我是医疗从业人士,研究点医疗算是干点人事。本文第一稿写于2025年7月,这两天业余时间进行了一些更新,还是算烂尾了,但想想我写的叫做“速览”我心安理得的烂尾。我这篇文章也不保证对,里头个人观点比较多,我自己对先声的研究时间不超过10个小时,深度肯定也不够的。有错误欢迎指正下文中,关于事实会有正常字体,而我的观点将会用加粗字体正文开始:港股的BioPharma中,从市值看瑞、信达、百济神州这些千亿级市值的算第一梯队。先声药业属于第二梯队的老牌药企,且非常有特点——布局中枢神经(CNS)、自免、肿瘤三大赛道。CNS药物是除了肿瘤和自免外,市场容量最大的药物领域;先声是一家很聪明的公司,我很喜欢。关注我的朋友应该知道我是重点关注CNS这个学科,而不是肿瘤的。对于肿瘤这种赛道拥挤度太高的学科,我水平太二把刀了,还是找些有钱但赛道拥挤度不高的研究更好。这个学科有研究的友友咱们多多交流先声药业当前市值约257亿港元(2026年5月),市销率(TTM)约3.0x、市盈率(TTM)约17.3x、市净率约2.47x、股息率(TTM)约1.68%。2025年全年,公司实现营业收入77.31亿元,同比增长16.5%;创新药业务收入63.04亿元,占总收入比重达到81.5%,创历史新高;归母净利润13.44亿元,同比增长86.2%。创新药占比从2020年的约45%大幅提升至超过八成,这个“仿转创”的转型在传统化药企业里非常了不起。1995年,江苏先声药业成立,主要从事药品的商业化。2007年4月,先声药业登陆纽交所,成为首家在纽交所上市的中国化学生物药公司,上市时募资2.26亿美元,市值一度超过10亿美元。在美股上市阶段,公司收入达到13-20亿级别,2007年年收入就能够达到13亿,而恒瑞当年的收入也不到20亿。从历史来看先声在古典阶段能跟恒瑞掰手腕的。2013年,由创始人任晋生、弘毅投资、复星医药等组成的财团以总代价4.95亿美元收购外部流通股,完成私有化。实控人任晋生心中充满不甘,在后来的媒体报道中,他曾不止一次提到“公司被低估”。我相信任总现在也会觉着先声被低估,先声我看来是一家优秀的企业。2020年10月27日,先声药业港股IPO,IPO时市值约357亿港元。等到回港股上市的时候,公司收入规模已经接近50亿。任晋生1982年毕业于南京中医药大学中药专业,毕业后被分配到苏北启东盖天力制药厂,10年时间从一名车间普通技术员成长为经营副厂长,将“盖天力”品牌在全国打响。1992年,他毅然辞掉国企铁饭碗,和6位平均年龄只有20多岁的年轻人到南京创业。创业初期7人凑齐5万元承包了江苏省医药工业公司的新特药经营部,并在国内率先采取“总经销”“总代理”的经营模式。1999年进行二次改制,成为一家以民营资本为主导的企业。2001年,先声通过资本运作并购海南富海,从医药商业公司转型成为制药公司,这是先声历史上的第一笔资本运作。先声的产品线主要是三条,神经科学领域(CNS),肿瘤,自免。后续会按照这三条产品线对先声药业进行分析,但从2020年先声回归港股之后为时间点,先声的可以说是两家公司。我把2020年港股上市作为划分先声发展阶段的时间点,一方面是港股IPO这个特殊节点,另一方面则是医保改革在此时间点后愈演愈烈。这个时间点,也是公司“仿转创”的重要业务转折点。一、古典阶段的先声,医保改革前的阶段(2019及之前):在港股再次上市的时候,先声2019年的销售收入接近50亿元,依达拉奉+恩度+艾拉莫德三大重磅药加起来超过了收入的50%。可以说在这之前先声还是一家传统的化药仿制药企业CNS领域:2003年,先声首仿上市了依达拉奉(商品名必存),这是一款脑保护剂(自由基清除剂),在脑梗死发病24小时内使用可改善神经症状和功能障碍。2007年9月28日,先声斥资1.11亿元收购依达拉奉的二仿——吉林省博大制药51%的股权,将博大旗下的"易达生"收入囊中。必存与易达生相互补充,分别占领高端和中低端依达拉奉市场,变相垄断了这款产品的主要市场。在退出医保前,依达拉奉的主要市场玩家还是先声。本领域目前还有个有临床证据的重磅标杆药物是石药的丁苯酞。2019年7月,国家卫健委发布《第一批国家重点监控合理用药药品目录》,神经节苷脂、脑苷肌肽、奥拉西坦、依达拉奉等20个品种被纳入监控,随后这些品种系数被调出2019版国家医保目录,导致这个领域有大量品种直接消失在历史长河——包括神经节苷脂、脑苷肌肽、奥拉西坦、长春西汀等,曾经的大品种断崖式下滑。神经保护剂曾是神药集中营,充斥着各种10亿级重磅品种。但这个领域的基础研究一直不清楚,机制众说纷纭,你管那么多机制干啥,看临床数据有用不就完了。最起码依达拉奉被剔除之后还能回归,证明确实有用,而且我也跟临床老师聊过这个事儿,就有神内的老师跟我说依达拉奉患者用了好使啥的依达拉奉在这个政策事件后开始走下坡路,2017年销售额还有12.44亿元,2018年11.99亿元,2019年下滑到9.37亿元(占先声总营收的18.6%,占依达拉奉市场份额的36.8%)。2019年被纳入重点监控并调出医保后,2020年上半年依达拉奉营收同比暴跌68.92%,仅1.78亿元。自2022版国家医保目录调整开始,"非独家药品竞价"成为新亮点,依达拉奉注射液作为非独家产品通过该方式重新进入医保目录,但市场已不复当年。肿瘤领域:2006年5月28日,先声药业斥资2亿元打败60多家国内外竞争对手,收购烟台麦得津80%股份,将后者刚刚上市的世界第一个重组人血管内皮抑制素、抗肿瘤一类生物创新药——恩度(重组人血管内皮抑制素注射液,靶点VEGF)纳入麾下。在当年,非小细胞肺癌患者在化疗之后,在中国可选择的生物药有且仅有恩度。2020年港股上市时,恩度已经成为先声最核心的产品之一,销售额收入占比达到约四分之一,超过11亿元。这是20年前的生物靶向药,当年在中国花2亿跟现在也不可同日而语,先声当年出手并购恩度可谓是战略眼光超群。恩度作为VEGF靶点的生物药,近些年围绕这个靶点有很多创新药陆续获批,此靶点的仿制药都有几十个了,非小细胞肺癌这个适应症也是众多创新药神仙云集,竞争烈度在2019年后与之前不可同日而语。2007年11月26日,先声收购东捷药业85.71%股权,获得首入市场的新型铂类抗癌化疗药捷佰舒(注射用奈达铂)。2008年4月18日,先声收购芜湖中人药业70%的股权,拿下中人氟安(5-氟尿嘧啶植入剂),这是一款国内外独家、首批上市的缓释氟尿嘧啶植入剂,属于特殊剂型的术中化疗药。中人氟安自2003年底上市以来,截至2007年累计销售约26万支,2007年销售额约3300万元。被收购后先声希望第二年将其做成又一个亿元级产品。2019年,中人氟安占中国消化系统肿瘤术中化疗市场约6.6%的份额。近年该品种一直维持在1亿左右销售额,属于稳定贡献但天花板有限的小品种。又是一个成功的收购,先声这方面做的真不错。自免领域:2011年,先声与天津药物研究院合作研发的艾拉莫德(商品名艾得辛)获批上市,这是一款类风湿性关节炎的一类创新药,也是全球第一个上市的艾拉莫德制剂、全新结构类型的DMARDs(改善病情抗风湿药)。2019年销售额超过5亿。现在大热的自免领域当年并没有这么火,15年前先声就差异化布局了一类新药,避开了当时拥挤的肿瘤赛道。艾拉莫德的作用机制尚不完全清楚。体外研究显示,它可抑制核因子-κB(NF-κB)的活性,进而抑制炎性细胞因子(白介素-1、白介素-6、白介素-8、肿瘤坏死因子α)的生成;还可与小鼠和人的B细胞直接作用,抑制免疫球蛋白的生成;此外可抑制环氧酶-2(COX-2)的活性,但对环氧酶-1(COX-1)无影响。临床研究表明,服用该药最快4-6周即可起效,可明显改善类风湿关节炎患者的症状和体征,提高生活质量。与传统细胞毒药物相比,安全性较好。最为重要的是,艾拉莫德可以有效阻止骨质破坏,减少患者的致残率和致畸率。先声这个自免是古典时代的自免药物了,现在自免走的是另一条路,关于自免我在历史文章再鼎业绩Q4有写过自己的思考其他:瑞舒伐他汀(商品名舒夫坦)是一种HMG-CoA还原酶抑制剂,属于他汀类降脂药,用于高胆固醇血症及混合性血脂异常,通过降低低密度脂蛋白胆固醇(LDL-C,即"坏胆固醇")来预防动脉粥样硬化性心血管疾病。每日服用5-20mg可降低LDL-C约38%-48%。2019年,瑞舒伐他汀收入占比7%,为公司第四大品种,销售超过3.5亿元。2019年后进入国家集采时刻,先声选择了弃标。二、仿转创的先声:2020年上市后医保改革后的阶段先声在2020年回归港股的时候,只有恩度和艾拉莫德两款药算作创新药,而接下来的几年获批了多款创新药,现在创新药占比超过80%,属于很成功的“仿转创”。这对于传统化药企业非常了不起,君不见现在的龙头化药巨头都没有到达这个比例。(1)CNS:先必新系列与科唯可神经保护剂在医保监控目录以及退出医保政策下,大批量品种在临床终端消亡,包括先声的依达拉奉,也包括神经节苷脂、脑苷肌肽、奥拉西坦等等。与此同时,也腾出了巨大的市场需求,石药的丁苯酞作为为数不多做出临床证据的药,在这种背景下得到快速发展。2020年,先必新(依达拉奉右莰醇注射用浓溶液)获批上市,这是2015年以来国内卒中治疗领域唯一上市的创新药。2020年先必新刚上市这年,神经系统板块收入已经从高点的12亿下降到7亿;而到了2021年,也就是先必新进入医保目录后的第一个完整销售年度,神经系统板块收入15亿,同比增长120%。2025年,神经科学领域收入达到27.53亿元,同比增长26.6%,其中先必新注射液市场份额约31%,覆盖超6500家医疗机构。先必新舌下片于2024年12月获批上市,可与注射液序贯使用,显著延长治疗周期。先声预计先必新系列产品天花板可能奔着50亿级别增长。根据医保支付价,先必新注射剂日治疗费用(使用6支)2024年约为198元,2025年国谈续约后降至约177元/日。按平均住院时长7天计算,一个疗程总费用约1386元。先必新注射液已纳入乙类医保,假设报销30%则患者自付部分约415.8元。先必新舌下片作为住院期注射剂的延续治疗,目前尚未纳入国家医保目录,但符合新增医保目录申请条件,公司正在积极沟通争取纳入。舌下片在网上药房标价约980元/盒(14片,每片70元),按每日2片计算,14天费用约1960元。先必新是先声的基石药物,我在我们有个医疗群里,大家都是一二级的投资经理研究院及卖方分析师,医药自媒体,我看大家都研究肿瘤,CGT,我研究先必新,有时候觉着自己怪萨比的,都不好意思跟大家讨论达利雷生(商品名:科唯可):这是先声从瑞士Idorsia引进的改善日间功能的失眠药,已于2025年6月在中国获批上市。科唯可是目前唯一获美、欧、日批准的可改善日间功能的双食欲素受体拮抗剂(DORA)类失眠药,2025版中国失眠治疗路径已将其列为最高证据等级(A级)。其半衰期约8小时,无药物依赖与成瘾风险,且未被列入我国精神药品管制目录,可在医院、零售及电商渠道凭普通处方购买。公司预计其销售峰值可能超过40亿元。药物机制觉着不错啊,副作用从机制看比传统安眠药小得多,这有点消费医疗的属性,我对消费医疗一窍不通,这个药卖的好不好不懂,懂的友友可以来指点我(2)肿瘤:从恩维达到恩泽舒先声药业2020年8月从美国G1Therapeutics引进曲拉西利时,这款药在海外市场还未获批,属于"买在爆发前夜"的超前布局。交易总额1.7亿美元,包括1400万美元首付款和1.56亿美元里程碑付款,先声获得大中华区所有适应症的独家开发和商业化权益。2021年2月,曲拉西利获FDA批准,成为全球首个在化疗前给药、拥有全系骨髓保护作用的创新药物,曾获FDA突破性疗法认定和优先审评资格;2022年7月12日在中国获附条件上市批准;2023年10月转为常规上市;2023年8月,拓扑替康方案的新适应症NDA获受理;2024年底纳入国家医保目录。这个案例我看完是很震撼的,因为觉着先声太牛逼了。牛逼在哪?第一,桥接数据的精准运用。先声引进后没有从头做大规模III期,而是做了安全性导入和药代动力学(PK)桥接试验——2021年5月首例受试者入组,同年11月完成全部入组,分析结果显示中国患者与境外患者具有一致的药物代谢动力学特征和临床获益趋势。因为FDA已经快速获批,CDE认可了桥接数据,这让先声从BD到上市仅用了不到两年时间,2020年8月引进,2022年7月就批下来了。这也是我认知里最快上市的BD案例,第二,站在MNC的肩膀上。CDK4/6这个靶点被辉瑞(哌柏西利)、礼来(阿贝西利)、诺华(瑞波西利)以及国产恒瑞(达尔西利)等巨头在国外和国内科普了很久,医生和患者对这个靶点的认知已经被教育得非常充分。先声不需要再去教育市场,直接享受了整个靶点的认知红利。第三,摘了骨髓保护的差异化果子。所有MNC的CDK4/6抑制剂都在挤HR+/HER2-乳腺癌这个核心适应症,赛道拥挤得神仙打架。而G1的曲拉西利选择的是肺癌化疗后的骨髓抑制保护,作为骨髓保护剂来申报——这个适应症临床做起来比传统肿瘤治疗快得多(肿瘤生存期就决定了临床试验短不了),且因为FDA的快速获批,CDE直接让做桥接试验就给批了。先声仅付了1400万美元的首付款,就快速拿到了一个First-in-Class的特色产品。大靶点+小适应症,找小公司去扫货,先声这个"取巧"的BD战略优势在这个药物上体现得淋漓尽致。至于后期怎么围绕骨髓保护这个特色适应症在肿瘤科室做临床推广,相信先声的销售能力了。(2)恩立妥(西妥昔单抗β注射液):填补近20年国产EGFR抗体空白2005年,第一款进口EGFR抗体药物西妥昔单抗在中国获批治疗结直肠癌,该领域十余年来在中国未有同靶点国产产品上市,医生和患者在临床用药上选择有限。尽管进口西妥昔单抗治疗结直肠癌的疗效已有大量临床数据验证,但仍存在进口可及性无法保证、安全性有待改进等潜在问题——尤其是西妥昔单抗的糖基化修饰可能导致严重超敏反应。2023年8月,先声从迈博药业引进西妥昔单抗β注射液,获得中国内地市场权益。恩立妥是西妥昔单抗的2.4类改良型新药,通过优化分子结构有效避免了导致超敏反应的糖基化修饰问题。2024年6月,恩立妥获批上市,用于与FOLFIRI方案联合一线治疗RAS/BRAF基因野生型的转移性结直肠癌,填补了我国结直肠癌EGFR靶向抗体药物市场近20年来仅有进口药物、而无国产品种的空白。2024年12月,恩立妥纳入国家医保目录。EGFR靶向治疗获批适应症均为与生物标志物检测配合的特定人群使用,即RAS/BRAF基因未发生突变的野生型患者。中国结直肠癌患者中,RAS/BRAF野生型占比接近45%。据相关企业年报及全球数据库显示,2023年西妥昔单抗全球销售额超10亿欧元,中国销售额超20亿元人民币。恩立妥作为国产替代,在这个已有充分临床验证的成熟靶点上切入,逻辑清晰。(3)恩泽舒(注射用苏维西塔单抗):铂耐药卵巢癌的国产首个全人群靶向药恩泽舒的渊源可以追溯到2008年——先声药业从Epitomics公司收购了该药的专利权。随后Epitomics于2010年7月成立了Apexigen,并授权后者独家使用其抗体技术进行抗体疗法的开发和商业化,同时将与先声药业的许可及合作协议转让给Apexigen。后来Apexigen并入PyxisOncology,先声再明与PyxisOncology联合开发,先声再明基于自有技术平台完成了细胞株筛选、工艺开发以及临床样品生产,获批后由先声再明南京江北新区抗体工厂开展商业化生产。苏维西塔单抗是一种新一代重组人源化抗VEGF兔源单克隆抗体,通过差异化分子表位设计精准阻断VEGF与受体(VEGFR2)的结合,抑制肿瘤血管生成。临床前研究显示,在相同剂量下其抑瘤效果强于贝伐珠单抗,剂量仅为贝伐珠单抗的1/7。2024年1月,III期SCORES研究达到主要终点;2024年3月,NDA获NMPA受理;2025年6月30日,恩泽舒获批上市,联合紫杉醇、多柔比星脂质体或拓扑替康用于铂耐药后接受过不超过1种系统治疗的成人复发性卵巢癌、输卵管癌或原发性腹膜癌。这是中国首个获批用于铂耐药复发卵巢癌全人群的血管靶向治疗药物,打破了该领域既往治疗选择有限的困局。SCORES研究显示:中位无进展生存期(PFS)达5.49个月(对照组2.73个月),疾病进展风险降低54%(HR=0.46);总生存期(OS)死亡风险降低23%(HR=0.77),是首个在该人群中显示OS获益的血管靶向药。更难得的是,恩泽舒在获批当年即被纳入2025年国家医保目录,于2026年1月1日起执行。先声给出的该药物业绩指引是在2030年可实现14.2亿元销售额。此外,恩度(重组人血管内皮抑制素注射液)也于2025年成功转入医保常规药品目录(非协议期内谈判药品),进一步巩固了其在晚期非小细胞肺癌治疗中的基石地位。(3)自免:艾拉莫德与后续管线2025年,自身免疫领域收入18.92亿元,同比增长4.5%,增速放缓主要受部分品种省级集采影响。艾拉莫德(艾得辛)作为全球首个且国内唯一上市的艾拉莫德药物,也是近十年唯一上市的中国自主研发的小分子改善病情抗风湿药物(DMARDs),持续巩固市场领导地位,是先声自免板块的基石。LNK01001:这是先声从凌科药业(LynkPharmaceuticals)引进的临床III期高选择性JAK1抑制剂(通用名:Zemprocitinib)。2022年3月,先声与凌科达成商业化合作协议,获得该药在大中华区类风湿关节炎和强直性脊柱炎的独家商业化权益。凌科药业2026年1月港股IPO招股书显示,LNK01001正在开展多项III期临床试验,预计2026年上半年针对特应性皮炎、2026年下半年针对类风湿关节炎、2027年下半年针对强直性脊柱炎进入新药申请阶段。JAK抑制剂一直是口服自免的重要靶点,这个药的引进增加了先声自免产品线的厚度。乐德奇拜单抗(商品名:乐瑞平):这是靶向IL-4Rα的全人源单抗,先声2023年11月从康乃德生物医药引进,获得大中华区开发、生产和商业化的独家权利。2025年7月,乐德奇拜单抗治疗特应性皮炎的NDA首次获国家药监局受理。然而,2026年4月,该上市申请收到通知件(被拒)。2026年4月29日,先声重新提交的NDA再次获受理。三期临床数据显示,第16周EASI-75应答率达到74.2%,至第52周升至96.6%,显示出深度缓解优势。其哮喘适应症已进入III期临床。这个药也很有故事,先声属于“捡漏”型BD,目前付出了1.5亿元人民币的首付款。国内康诺亚的IL-4Rα单抗已经获批上市,2年后可能有一堆国产IL-4Rα集中上市,先声也在其中。自免这个学科,考虑到国内的支付环境和复杂临床,我始终在思考(4)抗感染:先诺欣与玛氘诺沙韦先声在抗感染领域其实没啥深厚的历史积淀,不像神经科学有依达拉奉、肿瘤有恩度、自免有艾拉莫德那样有十几年的根基。抗感染这块,主要讲新冠口服药先诺欣,一个是流感药玛氘诺沙韦(先林达)。先声汇报业绩时重点讲的是神经科学、抗肿瘤、自身免疫三大领域,抗感染基本被归入"其他"或者干脆不提,这说明这个板块战略重要性有限。先诺欣(先诺特韦片/利托那韦片组合包装)2023年初获批,是中国首款自主研发、具备自主知识产权的3CL靶点抗新冠病毒创新药。先声在疫情期决定快速开发这款药,2021年底引进了上海药物研究所和武汉病毒研究所的3CL口服新冠药,2023年初附条件上市,成为最先上市的4款国产口服新冠药之一。但问题是,这药生不逢时——批下来的时候疫情已经收尾了。2024年中报里,先声自己白纸黑字写的:"受新冠疫情变化影响,先诺欣®销售收入有所下降;其他领域收入较2023年同期下降约16.8%。"2024年7月虽然转为常规批准,但市场需求已经断崖式萎缩。所以不是先声不想提,是这个产品从当年的"王炸"变成了现在的"鸡肋",提多了反而暴露短板。不过这也侧面说明先声的市场嗅觉确实敏锐——能在疫情尾声快速布局并获批,这种反应速度不是所有药企都有的。玛氘诺沙韦(商品名:先林达)是先声与安帝康生物合作开发的抗流感创新药,为cap依赖型核酸内切酶抑制剂(注意:不是RNA聚合酶PA抑制剂,玛巴洛沙韦才是PA抑制剂)。其通过抑制流感病毒cap依赖型核酸内切酶,阻断病毒自身mRNA转录,从根源对病毒实施精准打击。玛氘诺沙韦全病程仅需口服"一粒",可在24小时内阻止流感病毒复制。2025年3月,片剂(成人及青少年)获批上市;2025年9月,儿童颗粒剂(2-11岁)的NDA获受理,是中国首个成功完成III期临床并申报上市的针对儿童患者的抗流感病毒创新药。此外,2岁及以上人群甲型乙型流感暴露后预防试验也已启动。2025年3月才获批,9月儿童适应症才申报,处于商业化极早期,2025年年报里根本没披露具体销售额。奥司他韦曾经摸到过50亿的销售额,2021年获批的罗氏玛巴洛沙韦是下一代流感药,2023年玛巴洛沙韦片国内销售额超过5亿元,预计2024年超过10亿元。类似玛巴洛沙韦的PA抑制剂,青峰医药已经获批上市,后面健康元、济川都有类似品种。国内差不多都是前后脚上市,先声自己给的峰值预期也就1亿元级别——在77亿总收入里连零头都算不上。现在奥司他韦已经集采了,未来流感PA抑制剂感觉也快集采,玛氘诺沙韦作为cap抑制剂虽然机制不同,但临床优势是否足够突出、能不能在红海市场里切出一块肉来,还得看儿童颗粒剂获批后能不能在儿科市场打出差异化。先声在业绩会上不提它,原因很简单:体量太小,讲多了浪费口舌。三、在研管线展望(烂尾部分,只有事实无个人点评,全是搬运的事实,因为没时间写了)SIM0270(口服SERD):这是不区分ESR1突变状态、覆盖HR+/HER2-全人群的口服选择性雌激素受体降解剂(SERD)。其差异化优势在于具有更高效的血脑屏障通透性,脑血比较同类化合物高4-10倍,有望解决乳腺癌脑转移未满足需求。目前正在开展一项覆盖二线HR+/HER2-全人群联合依维莫司的III期临床(SIMRISE),计划在中国约50个研究中心入组460名患者,预计有望于2026年第四季度读出topline数据,并有望成为国内第一递交上市申请的口服SERD。SIM0278(IL-2mu-Fc):这是先声利用自有蛋白质工程技术平台开发的Treg偏好型IL-2突变融合蛋白,通过引入突变降低与效应T细胞的亲和力,同时保留与Treg细胞的高亲和力,从而选择性激活Treg细胞,帮助恢复机体免疫平衡,而不影响效应T细胞或NK细胞。2022年9月,先声与西班牙Almirall公司达成海外授权协议(首付款1500万美元,潜在总额4.92亿美元),保留大中华区权益。2025年11月,SIM0278已正式启动中国II期临床研究,用于中重度特应性皮炎,并于杭州市第一人民医院完成首例患者给药。该药物在已完成的I期临床中显示出初步疗效信号、良好耐受性和合适的药代动力学特征,具备BIC(Best-in-Class)潜力。六、BD对外授权(烂尾部分,只有事实无个人点评,全是搬运的事实,因为没时间写了)先声药业明确提出“自研+BD”双轮驱动,近五年累计研发投入约90亿元。其对外授权已从早期的license-in为主,全面升级为license-out与license-in并重的全球化布局。对外授权集中在肿瘤(ADC/多抗)和自身免疫(双抗)两大领域,且多为临床前/早期项目,体现国际巨头对其技术平台的认可。截至2026年1月,先声已有5项自研早研项目实现海外授权,潜在交易总金额超46亿美元。2025年,公司合计收到对外许可首付款及里程碑付款1.54亿美元,其中约6350万美元已在当年确认收入。具体授权情况如下:2022年9月,SIM0278(IL-2mu-Fc)授权给西班牙Almirall公司,潜在总额4.92亿美元,先声保留大中华区权益。2025年1月,抗肿瘤三抗SIM0500与美国艾伯维达成海外权益许可选择权合作。2025年6月,SIM0505(CDH6ADC)及ADC平台授权给美国NextCure,潜在总额7.45亿美元,且NextCure可使用先声ADC平台开发新靶点药物,属于双向技术合作。2025年12月,SIM0613(LRRC15ADC)授权给法国益普生,潜在总额10.60亿美元。2026年1月,SIM0709(TL1A/IL-23p19双抗)授权给德国勃林格殷格翰,潜在总额10.58亿欧元,先声保留大中华区权益并收取4200万欧元首付款。这种全球共建、区域分治的模式,标志着先声的议价能力显著提升,不再是以早期全盘卖青苗的被动姿态。这段瞎几把写的,随便看吧,写不动了七、整体结论从管线布局来看,先声的战略风格20年来一直是在药品领域做差异化竞争,不与强大的对手正面硬刚。自免和肿瘤药的布局别看现在大火,当年也是差异化竞争。近几年公司围绕着大适应症或者大靶点+小适应症做了很多捡漏性BD——流感药抑制剂、自免IL-4Rα、失眠药DORA、CDK4/6骨髓保护都是如此。说回先必新,先声的整体风格可以说是聪明,不硬碰硬,四两拨千斤。别听那些人扯淡说什么国内的药企只会卖药,能卖药的人一定是情商最高的,你换新的biotech药都不知道咋卖。能把先必新做到神经保护剂的龙头,绝对是会卖货的。先必新目前在缺血性脑卒中AIS适应症上作为唯一纳入指南Ⅱa类推荐的神经保护剂,加之全年国内超20亿元销售,配合后续的舌下片剂型覆盖更多临床场景,在国内AIS适应症任何新品想要上市,都需要考虑与先必新的竞争关系。(还有丁苯酞,两者算是脑卒中领域的大小王了)公司2025年业绩已经创出新高,净利润增长86%,创新药占比超八成,10款创新药形成“5款基石+5款放量新品”的产品梯队,加上对外授权成为新的增长引擎,基本面是在持续改善的。先声的股东回报在创新药里可以了,别拿着跟中海油啥的比。我现在已经是熊市思维了,我只买超过5%股息率的股票,做好防守。所以除了做动量暂时不考虑医疗板块尤其创新药这种行业风险大的行业先声药业在港股市场不太受待见,港股投资者觉着先声取巧,管理层给出的销售峰值指引也常被质疑。其实管线太多了,我只是挑挑拣拣地分析,算是烂尾了,但是我累了就这样吧,毕竟这个系列叫做“速览”。港股反而喜欢做头对头的企业,也可能香港的分析师只看得懂头对头(更新:我现在不这么看了,我不该这么吐槽。索罗斯说价值是主观的,价格才是客观的。尤其是创新药这个行业门槛太高,对于散户是100尺栏,判断价值这个事情太主观,头对头或者BD的金额更客观,很多创新药的市值看叙事吧。按确定性顺序:股息,现金流,利润,营收,订单,技术导入验证,技术储备和市场容量,在港股这个市场,股息才是能确定的事情,别的都是流动性带来的叙事)如果先声在A股上市,最牛的神经保护剂先必新、新冠口服药、创新药占比超80%、BD出海这些都可以是炒作题材,我认为先声这样一家优秀的企业绝对不止现在200多亿港币的市值。做大事要有天时地利人和,港股这个泥坑离岸市场天时不行,这资本市场跟咱大A比不了啊(又到了我日常黑港股的环节)。主要参考资料:先声药业2025年度业绩公告、2025年中期业绩报告;国金证券、中金公司、交银国际研报;美国临床肿瘤学会(ASCO)年会摘要;公司官方新闻稿及港交所公告。$先声药业(02096)$@超级泥头车@Wankm5@徐大宝李二狗@管我财@范俊青@先声药业你们公司粉丝咋还没我多
2026-05-29
·雪球
哥们儿终于不再HR提离职——不干人事了@小刘鸭埃里克前言:不构成购买建议,我从来没买过先声的股票,这篇文章只是我研究创新药的研究框架,不构成投资建议,别在这文章底下问我“老师,XX药业帮我看下,多少钱能不能买?”,我不是你们丫的医疗许愿池最近我在全力梭哈押注能源危机,我的主仓是海油神火,只是这种票最近行情无聊得等,毕竟我是医疗从业人士,研究点医疗算是干点人事。本文第一稿写于2025年7月,这两天业余时间进行了一些更新,还是算烂尾了,但想想我写的叫做“速览”我心安理得的烂尾。我这篇文章也不保证对,里头个人观点比较多,我自己对先声的研究时间不超过10个小时,深度肯定也不够的。有错误欢迎指正下文中,关于事实会有正常字体,而我的观点将会用加粗字体正文开始:港股的BioPharma中,从市值看瑞、信达、百济神州这些千亿级市值的算第一梯队。先声药业属于第二梯队的老牌药企,且非常有特点——布局中枢神经(CNS)、自免、肿瘤三大赛道。CNS药物是除了肿瘤和自免外,市场容量最大的药物领域;先声是一家很聪明的公司,我很喜欢。关注我的朋友应该知道我是重点关注CNS这个学科,而不是肿瘤的。对于肿瘤这种赛道拥挤度太高的学科,我水平太二把刀了,还是找些有钱但赛道拥挤度不高的研究更好。这个学科有研究的友友咱们多多交流先声药业当前市值约257亿港元(2026年5月),市销率(TTM)约3.0x、市盈率(TTM)约17.3x、市净率约2.47x、股息率(TTM)约1.68%。2025年全年,公司实现营业收入77.31亿元,同比增长16.5%;创新药业务收入63.04亿元,占总收入比重达到81.5%,创历史新高;归母净利润13.44亿元,同比增长86.2%。创新药占比从2020年的约45%大幅提升至超过八成,这个“仿转创”的转型在传统化药企业里非常了不起。1995年,江苏先声药业成立,主要从事药品的商业化。2007年4月,先声药业登陆纽交所,成为首家在纽交所上市的中国化学生物药公司,上市时募资2.26亿美元,市值一度超过10亿美元。在美股上市阶段,公司收入达到13-20亿级别,2007年年收入就能够达到13亿,而恒瑞当年的收入也不到20亿。从历史来看先声在古典阶段能跟恒瑞掰手腕的。2013年,由创始人任晋生、弘毅投资、复星医药等组成的财团以总代价4.95亿美元收购外部流通股,完成私有化。实控人任晋生心中充满不甘,在后来的媒体报道中,他曾不止一次提到“公司被低估”。我相信任总现在也会觉着先声被低估,先声我看来是一家优秀的企业。2020年10月27日,先声药业港股IPO,IPO时市值约357亿港元。等到回港股上市的时候,公司收入规模已经接近50亿。任晋生1982年毕业于南京中医药大学中药专业,毕业后被分配到苏北启东盖天力制药厂,10年时间从一名车间普通技术员成长为经营副厂长,将“盖天力”品牌在全国打响。1992年,他毅然辞掉国企铁饭碗,和6位平均年龄只有20多岁的年轻人到南京创业。创业初期7人凑齐5万元承包了江苏省医药工业公司的新特药经营部,并在国内率先采取“总经销”“总代理”的经营模式。1999年进行二次改制,成为一家以民营资本为主导的企业。2001年,先声通过资本运作并购海南富海,从医药商业公司转型成为制药公司,这是先声历史上的第一笔资本运作。先声的产品线主要是三条,神经科学领域(CNS),肿瘤,自免。后续会按照这三条产品线对先声药业进行分析,但从2020年先声回归港股之后为时间点,先声的可以说是两家公司。我把2020年港股上市作为划分先声发展阶段的时间点,一方面是港股IPO这个特殊节点,另一方面则是医保改革在此时间点后愈演愈烈。这个时间点,也是公司“仿转创”的重要业务转折点。一、古典阶段的先声,医保改革前的阶段(2019及之前):在港股再次上市的时候,先声2019年的销售收入接近50亿元,依达拉奉+恩度+艾拉莫德三大重磅药加起来超过了收入的50%。可以说在这之前先声还是一家传统的化药仿制药企业CNS领域:2003年,先声首仿上市了依达拉奉(商品名必存),这是一款脑保护剂(自由基清除剂),在脑梗死发病24小时内使用可改善神经症状和功能障碍。2007年9月28日,先声斥资1.11亿元收购依达拉奉的二仿——吉林省博大制药51%的股权,将博大旗下的"易达生"收入囊中。必存与易达生相互补充,分别占领高端和中低端依达拉奉市场,变相垄断了这款产品的主要市场。在退出医保前,依达拉奉的主要市场玩家还是先声。本领域目前还有个有临床证据的重磅标杆药物是石药的丁苯酞。2019年7月,国家卫健委发布《第一批国家重点监控合理用药药品目录》,神经节苷脂、脑苷肌肽、奥拉西坦、依达拉奉等20个品种被纳入监控,随后这些品种系数被调出2019版国家医保目录,导致这个领域有大量品种直接消失在历史长河——包括神经节苷脂、脑苷肌肽、奥拉西坦、长春西汀等,曾经的大品种断崖式下滑。神经保护剂曾是神药集中营,充斥着各种10亿级重磅品种。但这个领域的基础研究一直不清楚,机制众说纷纭,你管那么多机制干啥,看临床数据有用不就完了。最起码依达拉奉被剔除之后还能回归,证明确实有用,而且我也跟临床老师聊过这个事儿,就有神内的老师跟我说依达拉奉患者用了好使啥的依达拉奉在这个政策事件后开始走下坡路,2017年销售额还有12.44亿元,2018年11.99亿元,2019年下滑到9.37亿元(占先声总营收的18.6%,占依达拉奉市场份额的36.8%)。2019年被纳入重点监控并调出医保后,2020年上半年依达拉奉营收同比暴跌68.92%,仅1.78亿元。自2022版国家医保目录调整开始,"非独家药品竞价"成为新亮点,依达拉奉注射液作为非独家产品通过该方式重新进入医保目录,但市场已不复当年。肿瘤领域:2006年5月28日,先声药业斥资2亿元打败60多家国内外竞争对手,收购烟台麦得津80%股份,将后者刚刚上市的世界第一个重组人血管内皮抑制素、抗肿瘤一类生物创新药——恩度(重组人血管内皮抑制素注射液,靶点VEGF)纳入麾下。在当年,非小细胞肺癌患者在化疗之后,在中国可选择的生物药有且仅有恩度。2020年港股上市时,恩度已经成为先声最核心的产品之一,销售额收入占比达到约四分之一,超过11亿元。这是20年前的生物靶向药,当年在中国花2亿跟现在也不可同日而语,先声当年出手并购恩度可谓是战略眼光超群。恩度作为VEGF靶点的生物药,近些年围绕这个靶点有很多创新药陆续获批,此靶点的仿制药都有几十个了,非小细胞肺癌这个适应症也是众多创新药神仙云集,竞争烈度在2019年后与之前不可同日而语。2007年11月26日,先声收购东捷药业85.71%股权,获得首入市场的新型铂类抗癌化疗药捷佰舒(注射用奈达铂)。2008年4月18日,先声收购芜湖中人药业70%的股权,拿下中人氟安(5-氟尿嘧啶植入剂),这是一款国内外独家、首批上市的缓释氟尿嘧啶植入剂,属于特殊剂型的术中化疗药。中人氟安自2003年底上市以来,截至2007年累计销售约26万支,2007年销售额约3300万元。被收购后先声希望第二年将其做成又一个亿元级产品。2019年,中人氟安占中国消化系统肿瘤术中化疗市场约6.6%的份额。近年该品种一直维持在1亿左右销售额,属于稳定贡献但天花板有限的小品种。又是一个成功的收购,先声这方面做的真不错。自免领域:2011年,先声与天津药物研究院合作研发的艾拉莫德(商品名艾得辛)获批上市,这是一款类风湿性关节炎的一类创新药,也是全球第一个上市的艾拉莫德制剂、全新结构类型的DMARDs(改善病情抗风湿药)。2019年销售额超过5亿。现在大热的自免领域当年并没有这么火,15年前先声就差异化布局了一类新药,避开了当时拥挤的肿瘤赛道。艾拉莫德的作用机制尚不完全清楚。体外研究显示,它可抑制核因子-κB(NF-κB)的活性,进而抑制炎性细胞因子(白介素-1、白介素-6、白介素-8、肿瘤坏死因子α)的生成;还可与小鼠和人的B细胞直接作用,抑制免疫球蛋白的生成;此外可抑制环氧酶-2(COX-2)的活性,但对环氧酶-1(COX-1)无影响。临床研究表明,服用该药最快4-6周即可起效,可明显改善类风湿关节炎患者的症状和体征,提高生活质量。与传统细胞毒药物相比,安全性较好。最为重要的是,艾拉莫德可以有效阻止骨质破坏,减少患者的致残率和致畸率。先声这个自免是古典时代的自免药物了,现在自免走的是另一条路,关于自免我在历史文章再鼎业绩Q4有写过自己的思考其他:瑞舒伐他汀(商品名舒夫坦)是一种HMG-CoA还原酶抑制剂,属于他汀类降脂药,用于高胆固醇血症及混合性血脂异常,通过降低低密度脂蛋白胆固醇(LDL-C,即"坏胆固醇")来预防动脉粥样硬化性心血管疾病。每日服用5-20mg可降低LDL-C约38%-48%。2019年,瑞舒伐他汀收入占比7%,为公司第四大品种,销售超过3.5亿元。2019年后进入国家集采时刻,先声选择了弃标。二、仿转创的先声:2020年上市后医保改革后的阶段先声在2020年回归港股的时候,只有恩度和艾拉莫德两款药算作创新药,而接下来的几年获批了多款创新药,现在创新药占比超过80%,属于很成功的“仿转创”。这对于传统化药企业非常了不起,君不见现在的龙头化药巨头都没有到达这个比例。(1)CNS:先必新系列与科唯可神经保护剂在医保监控目录以及退出医保政策下,大批量品种在临床终端消亡,包括先声的依达拉奉,也包括神经节苷脂、脑苷肌肽、奥拉西坦等等。与此同时,也腾出了巨大的市场需求,石药的丁苯酞作为为数不多做出临床证据的药,在这种背景下得到快速发展。2020年,先必新(依达拉奉右莰醇注射用浓溶液)获批上市,这是2015年以来国内卒中治疗领域唯一上市的创新药。2020年先必新刚上市这年,神经系统板块收入已经从高点的12亿下降到7亿;而到了2021年,也就是先必新进入医保目录后的第一个完整销售年度,神经系统板块收入15亿,同比增长120%。2025年,神经科学领域收入达到27.53亿元,同比增长26.6%,其中先必新注射液市场份额约31%,覆盖超6500家医疗机构。先必新舌下片于2024年12月获批上市,可与注射液序贯使用,显著延长治疗周期。先声预计先必新系列产品天花板可能奔着50亿级别增长。根据医保支付价,先必新注射剂日治疗费用(使用6支)2024年约为198元,2025年国谈续约后降至约177元/日。按平均住院时长7天计算,一个疗程总费用约1386元。先必新注射液已纳入乙类医保,假设报销30%则患者自付部分约415.8元。先必新舌下片作为住院期注射剂的延续治疗,目前尚未纳入国家医保目录,但符合新增医保目录申请条件,公司正在积极沟通争取纳入。舌下片在网上药房标价约980元/盒(14片,每片70元),按每日2片计算,14天费用约1960元。先必新是先声的基石药物,我在我们有个医疗群里,大家都是一二级的投资经理研究院及卖方分析师,医药自媒体,我看大家都研究肿瘤,CGT,我研究先必新,有时候觉着自己怪萨比的,都不好意思跟大家讨论达利雷生(商品名:科唯可):这是先声从瑞士Idorsia引进的改善日间功能的失眠药,已于2025年6月在中国获批上市。科唯可是目前唯一获美、欧、日批准的可改善日间功能的双食欲素受体拮抗剂(DORA)类失眠药,2025版中国失眠治疗路径已将其列为最高证据等级(A级)。其半衰期约8小时,无药物依赖与成瘾风险,且未被列入我国精神药品管制目录,可在医院、零售及电商渠道凭普通处方购买。公司预计其销售峰值可能超过40亿元。药物机制觉着不错啊,副作用从机制看比传统安眠药小得多,这有点消费医疗的属性,我对消费医疗一窍不通,这个药卖的好不好不懂,懂的友友可以来指点我(2)肿瘤:从恩维达到恩泽舒先声药业2020年8月从美国G1Therapeutics引进曲拉西利时,这款药在海外市场还未获批,属于"买在爆发前夜"的超前布局。交易总额1.7亿美元,包括1400万美元首付款和1.56亿美元里程碑付款,先声获得大中华区所有适应症的独家开发和商业化权益。2021年2月,曲拉西利获FDA批准,成为全球首个在化疗前给药、拥有全系骨髓保护作用的创新药物,曾获FDA突破性疗法认定和优先审评资格;2022年7月12日在中国获附条件上市批准;2023年10月转为常规上市;2023年8月,拓扑替康方案的新适应症NDA获受理;2024年底纳入国家医保目录。这个案例我看完是很震撼的,因为觉着先声太牛逼了。牛逼在哪?第一,桥接数据的精准运用。先声引进后没有从头做大规模III期,而是做了安全性导入和药代动力学(PK)桥接试验——2021年5月首例受试者入组,同年11月完成全部入组,分析结果显示中国患者与境外患者具有一致的药物代谢动力学特征和临床获益趋势。因为FDA已经快速获批,CDE认可了桥接数据,这让先声从BD到上市仅用了不到两年时间,2020年8月引进,2022年7月就批下来了。这也是我认知里最快上市的BD案例,第二,站在MNC的肩膀上。CDK4/6这个靶点被辉瑞(哌柏西利)、礼来(阿贝西利)、诺华(瑞波西利)以及国产恒瑞(达尔西利)等巨头在国外和国内科普了很久,医生和患者对这个靶点的认知已经被教育得非常充分。先声不需要再去教育市场,直接享受了整个靶点的认知红利。第三,摘了骨髓保护的差异化果子。所有MNC的CDK4/6抑制剂都在挤HR+/HER2-乳腺癌这个核心适应症,赛道拥挤得神仙打架。而G1的曲拉西利选择的是肺癌化疗后的骨髓抑制保护,作为骨髓保护剂来申报——这个适应症临床做起来比传统肿瘤治疗快得多(肿瘤生存期就决定了临床试验短不了),且因为FDA的快速获批,CDE直接让做桥接试验就给批了。先声仅付了1400万美元的首付款,就快速拿到了一个First-in-Class的特色产品。大靶点+小适应症,找小公司去扫货,先声这个"取巧"的BD战略优势在这个药物上体现得淋漓尽致。至于后期怎么围绕骨髓保护这个特色适应症在肿瘤科室做临床推广,相信先声的销售能力了。(2)恩立妥(西妥昔单抗β注射液):填补近20年国产EGFR抗体空白2005年,第一款进口EGFR抗体药物西妥昔单抗在中国获批治疗结直肠癌,该领域十余年来在中国未有同靶点国产产品上市,医生和患者在临床用药上选择有限。尽管进口西妥昔单抗治疗结直肠癌的疗效已有大量临床数据验证,但仍存在进口可及性无法保证、安全性有待改进等潜在问题——尤其是西妥昔单抗的糖基化修饰可能导致严重超敏反应。2023年8月,先声从迈博药业引进西妥昔单抗β注射液,获得中国内地市场权益。恩立妥是西妥昔单抗的2.4类改良型新药,通过优化分子结构有效避免了导致超敏反应的糖基化修饰问题。2024年6月,恩立妥获批上市,用于与FOLFIRI方案联合一线治疗RAS/BRAF基因野生型的转移性结直肠癌,填补了我国结直肠癌EGFR靶向抗体药物市场近20年来仅有进口药物、而无国产品种的空白。2024年12月,恩立妥纳入国家医保目录。EGFR靶向治疗获批适应症均为与生物标志物检测配合的特定人群使用,即RAS/BRAF基因未发生突变的野生型患者。中国结直肠癌患者中,RAS/BRAF野生型占比接近45%。据相关企业年报及全球数据库显示,2023年西妥昔单抗全球销售额超10亿欧元,中国销售额超20亿元人民币。恩立妥作为国产替代,在这个已有充分临床验证的成熟靶点上切入,逻辑清晰。(3)恩泽舒(注射用苏维西塔单抗):铂耐药卵巢癌的国产首个全人群靶向药恩泽舒的渊源可以追溯到2008年——先声药业从Epitomics公司收购了该药的专利权。随后Epitomics于2010年7月成立了Apexigen,并授权后者独家使用其抗体技术进行抗体疗法的开发和商业化,同时将与先声药业的许可及合作协议转让给Apexigen。后来Apexigen并入PyxisOncology,先声再明与PyxisOncology联合开发,先声再明基于自有技术平台完成了细胞株筛选、工艺开发以及临床样品生产,获批后由先声再明南京江北新区抗体工厂开展商业化生产。苏维西塔单抗是一种新一代重组人源化抗VEGF兔源单克隆抗体,通过差异化分子表位设计精准阻断VEGF与受体(VEGFR2)的结合,抑制肿瘤血管生成。临床前研究显示,在相同剂量下其抑瘤效果强于贝伐珠单抗,剂量仅为贝伐珠单抗的1/7。2024年1月,III期SCORES研究达到主要终点;2024年3月,NDA获NMPA受理;2025年6月30日,恩泽舒获批上市,联合紫杉醇、多柔比星脂质体或拓扑替康用于铂耐药后接受过不超过1种系统治疗的成人复发性卵巢癌、输卵管癌或原发性腹膜癌。这是中国首个获批用于铂耐药复发卵巢癌全人群的血管靶向治疗药物,打破了该领域既往治疗选择有限的困局。SCORES研究显示:中位无进展生存期(PFS)达5.49个月(对照组2.73个月),疾病进展风险降低54%(HR=0.46);总生存期(OS)死亡风险降低23%(HR=0.77),是首个在该人群中显示OS获益的血管靶向药。更难得的是,恩泽舒在获批当年即被纳入2025年国家医保目录,于2026年1月1日起执行。先声给出的该药物业绩指引是在2030年可实现14.2亿元销售额。此外,恩度(重组人血管内皮抑制素注射液)也于2025年成功转入医保常规药品目录(非协议期内谈判药品),进一步巩固了其在晚期非小细胞肺癌治疗中的基石地位。(3)自免:艾拉莫德与后续管线2025年,自身免疫领域收入18.92亿元,同比增长4.5%,增速放缓主要受部分品种省级集采影响。艾拉莫德(艾得辛)作为全球首个且国内唯一上市的艾拉莫德药物,也是近十年唯一上市的中国自主研发的小分子改善病情抗风湿药物(DMARDs),持续巩固市场领导地位,是先声自免板块的基石。LNK01001:这是先声从凌科药业(LynkPharmaceuticals)引进的临床III期高选择性JAK1抑制剂(通用名:Zemprocitinib)。2022年3月,先声与凌科达成商业化合作协议,获得该药在大中华区类风湿关节炎和强直性脊柱炎的独家商业化权益。凌科药业2026年1月港股IPO招股书显示,LNK01001正在开展多项III期临床试验,预计2026年上半年针对特应性皮炎、2026年下半年针对类风湿关节炎、2027年下半年针对强直性脊柱炎进入新药申请阶段。JAK抑制剂一直是口服自免的重要靶点,这个药的引进增加了先声自免产品线的厚度。乐德奇拜单抗(商品名:乐瑞平):这是靶向IL-4Rα的全人源单抗,先声2023年11月从康乃德生物医药引进,获得大中华区开发、生产和商业化的独家权利。2025年7月,乐德奇拜单抗治疗特应性皮炎的NDA首次获国家药监局受理。然而,2026年4月,该上市申请收到通知件(被拒)。2026年4月29日,先声重新提交的NDA再次获受理。三期临床数据显示,第16周EASI-75应答率达到74.2%,至第52周升至96.6%,显示出深度缓解优势。其哮喘适应症已进入III期临床。这个药也很有故事,先声属于“捡漏”型BD,目前付出了1.5亿元人民币的首付款。国内康诺亚的IL-4Rα单抗已经获批上市,2年后可能有一堆国产IL-4Rα集中上市,先声也在其中。自免这个学科,考虑到国内的支付环境和复杂临床,我始终在思考(4)抗感染:先诺欣与玛氘诺沙韦先声在抗感染领域其实没啥深厚的历史积淀,不像神经科学有依达拉奉、肿瘤有恩度、自免有艾拉莫德那样有十几年的根基。抗感染这块,主要讲新冠口服药先诺欣,一个是流感药玛氘诺沙韦(先林达)。先声汇报业绩时重点讲的是神经科学、抗肿瘤、自身免疫三大领域,抗感染基本被归入"其他"或者干脆不提,这说明这个板块战略重要性有限。先诺欣(先诺特韦片/利托那韦片组合包装)2023年初获批,是中国首款自主研发、具备自主知识产权的3CL靶点抗新冠病毒创新药。先声在疫情期决定快速开发这款药,2021年底引进了上海药物研究所和武汉病毒研究所的3CL口服新冠药,2023年初附条件上市,成为最先上市的4款国产口服新冠药之一。但问题是,这药生不逢时——批下来的时候疫情已经收尾了。2024年中报里,先声自己白纸黑字写的:"受新冠疫情变化影响,先诺欣®销售收入有所下降;其他领域收入较2023年同期下降约16.8%。"2024年7月虽然转为常规批准,但市场需求已经断崖式萎缩。所以不是先声不想提,是这个产品从当年的"王炸"变成了现在的"鸡肋",提多了反而暴露短板。不过这也侧面说明先声的市场嗅觉确实敏锐——能在疫情尾声快速布局并获批,这种反应速度不是所有药企都有的。玛氘诺沙韦(商品名:先林达)是先声与安帝康生物合作开发的抗流感创新药,为cap依赖型核酸内切酶抑制剂(注意:不是RNA聚合酶PA抑制剂,玛巴洛沙韦才是PA抑制剂)。其通过抑制流感病毒cap依赖型核酸内切酶,阻断病毒自身mRNA转录,从根源对病毒实施精准打击。玛氘诺沙韦全病程仅需口服"一粒",可在24小时内阻止流感病毒复制。2025年3月,片剂(成人及青少年)获批上市;2025年9月,儿童颗粒剂(2-11岁)的NDA获受理,是中国首个成功完成III期临床并申报上市的针对儿童患者的抗流感病毒创新药。此外,2岁及以上人群甲型乙型流感暴露后预防试验也已启动。2025年3月才获批,9月儿童适应症才申报,处于商业化极早期,2025年年报里根本没披露具体销售额。奥司他韦曾经摸到过50亿的销售额,2021年获批的罗氏玛巴洛沙韦是下一代流感药,2023年玛巴洛沙韦片国内销售额超过5亿元,预计2024年超过10亿元。类似玛巴洛沙韦的PA抑制剂,青峰医药已经获批上市,后面健康元、济川都有类似品种。国内差不多都是前后脚上市,先声自己给的峰值预期也就1亿元级别——在77亿总收入里连零头都算不上。现在奥司他韦已经集采了,未来流感PA抑制剂感觉也快集采,玛氘诺沙韦作为cap抑制剂虽然机制不同,但临床优势是否足够突出、能不能在红海市场里切出一块肉来,还得看儿童颗粒剂获批后能不能在儿科市场打出差异化。先声在业绩会上不提它,原因很简单:体量太小,讲多了浪费口舌。三、在研管线展望(烂尾部分,只有事实无个人点评,全是搬运的事实,因为没时间写了)SIM0270(口服SERD):这是不区分ESR1突变状态、覆盖HR+/HER2-全人群的口服选择性雌激素受体降解剂(SERD)。其差异化优势在于具有更高效的血脑屏障通透性,脑血比较同类化合物高4-10倍,有望解决乳腺癌脑转移未满足需求。目前正在开展一项覆盖二线HR+/HER2-全人群联合依维莫司的III期临床(SIMRISE),计划在中国约50个研究中心入组460名患者,预计有望于2026年第四季度读出topline数据,并有望成为国内第一递交上市申请的口服SERD。SIM0278(IL-2mu-Fc):这是先声利用自有蛋白质工程技术平台开发的Treg偏好型IL-2突变融合蛋白,通过引入突变降低与效应T细胞的亲和力,同时保留与Treg细胞的高亲和力,从而选择性激活Treg细胞,帮助恢复机体免疫平衡,而不影响效应T细胞或NK细胞。2022年9月,先声与西班牙Almirall公司达成海外授权协议(首付款1500万美元,潜在总额4.92亿美元),保留大中华区权益。2025年11月,SIM0278已正式启动中国II期临床研究,用于中重度特应性皮炎,并于杭州市第一人民医院完成首例患者给药。该药物在已完成的I期临床中显示出初步疗效信号、良好耐受性和合适的药代动力学特征,具备BIC(Best-in-Class)潜力。六、BD对外授权(烂尾部分,只有事实无个人点评,全是搬运的事实,因为没时间写了)先声药业明确提出“自研+BD”双轮驱动,近五年累计研发投入约90亿元。其对外授权已从早期的license-in为主,全面升级为license-out与license-in并重的全球化布局。对外授权集中在肿瘤(ADC/多抗)和自身免疫(双抗)两大领域,且多为临床前/早期项目,体现国际巨头对其技术平台的认可。截至2026年1月,先声已有5项自研早研项目实现海外授权,潜在交易总金额超46亿美元。2025年,公司合计收到对外许可首付款及里程碑付款1.54亿美元,其中约6350万美元已在当年确认收入。具体授权情况如下:2022年9月,SIM0278(IL-2mu-Fc)授权给西班牙Almirall公司,潜在总额4.92亿美元,先声保留大中华区权益。2025年1月,抗肿瘤三抗SIM0500与美国艾伯维达成海外权益许可选择权合作。2025年6月,SIM0505(CDH6ADC)及ADC平台授权给美国NextCure,潜在总额7.45亿美元,且NextCure可使用先声ADC平台开发新靶点药物,属于双向技术合作。2025年12月,SIM0613(LRRC15ADC)授权给法国益普生,潜在总额10.60亿美元。2026年1月,SIM0709(TL1A/IL-23p19双抗)授权给德国勃林格殷格翰,潜在总额10.58亿欧元,先声保留大中华区权益并收取4200万欧元首付款。这种全球共建、区域分治的模式,标志着先声的议价能力显著提升,不再是以早期全盘卖青苗的被动姿态。这段瞎几把写的,随便看吧,写不动了七、整体结论从管线布局来看,先声的战略风格20年来一直是在药品领域做差异化竞争,不与强大的对手正面硬刚。自免和肿瘤药的布局别看现在大火,当年也是差异化竞争。近几年公司围绕着大适应症或者大靶点+小适应症做了很多捡漏性BD——流感药抑制剂、自免IL-4Rα、失眠药DORA、CDK4/6骨髓保护都是如此。说回先必新,先声的整体风格可以说是聪明,不硬碰硬,四两拨千斤。别听那些人扯淡说什么国内的药企只会卖药,能卖药的人一定是情商最高的,你换新的biotech药都不知道咋卖。能把先必新做到神经保护剂的龙头,绝对是会卖货的。先必新目前在缺血性脑卒中AIS适应症上作为唯一纳入指南Ⅱa类推荐的神经保护剂,加之全年国内超20亿元销售,配合后续的舌下片剂型覆盖更多临床场景,在国内AIS适应症任何新品想要上市,都需要考虑与先必新的竞争关系。(还有丁苯酞,两者算是脑卒中领域的大小王了)公司2025年业绩已经创出新高,净利润增长86%,创新药占比超八成,10款创新药形成“5款基石+5款放量新品”的产品梯队,加上对外授权成为新的增长引擎,基本面是在持续改善的。先声的股东回报在创新药里可以了,别拿着跟中海油啥的比。我现在已经是熊市思维了,我只买超过5%股息率的股票,做好防守。所以除了做动量暂时不考虑医疗板块尤其创新药这种行业风险大的行业先声药业在港股市场不太受待见,港股投资者觉着先声取巧,管理层给出的销售峰值指引也常被质疑。其实管线太多了,我只是挑挑拣拣地分析,算是烂尾了,但是我累了就这样吧,毕竟这个系列叫做“速览”。港股反而喜欢做头对头的企业,也可能香港的分析师只看得懂头对头(更新:我现在不这么看了,我不该这么吐槽。索罗斯说价值是主观的,价格才是客观的。尤其是创新药这个行业门槛太高,对于散户是100尺栏,判断价值这个事情太主观,头对头或者BD的金额更客观,很多创新药的市值看叙事吧。按确定性顺序:股息,现金流,利润,营收,订单,技术导入验证,技术储备和市场容量,在港股这个市场,股息才是能确定的事情,别的都是流动性带来的叙事)如果先声在A股上市,最牛的神经保护剂先必新、新冠口服药、创新药占比超80%、BD出海这些都可以是炒作题材,我认为先声这样一家优秀的企业绝对不止现在200多亿港币的市值。做大事要有天时地利人和,港股这个泥坑离岸市场天时不行,这资本市场跟咱大A比不了啊(又到了我日常黑港股的环节)。主要参考资料:先声药业2025年度业绩公告、2025年中期业绩报告;国金证券、中金公司、交银国际研报;美国临床肿瘤学会(ASCO)年会摘要;公司官方新闻稿及港交所公告。$先声药业(02096)$@超级泥头车@Wankm5@徐大宝李二狗@管我财@范俊青@先声药业你们公司粉丝咋还没我多
2026-05-29
·科学战银
【伊顿健康导读】
如果银屑病患者同时存在超重或肥胖的情况,体重管理就不仅是改善外观的问题。大量的临床研究证实,体重超标是影响银屑病发生、发展和治疗效果的一个明确的、可干预的风险因素。
前几日小编写了一篇关于银屑病患者可以银屑病+减重同时治疗的文章,有许多体重可能超标的银屑病患者对其中的减重方案感兴趣,所以今天这篇文章的内容集中针对体重超标的银屑病患者给出了一些科学的减重方案。
减重改善银屑病
这是所有减重治疗的基本方案,也就是通过控制热量摄入与增加规律的身体活动来实现体重下降。
研究数据显示,对于肥胖的银屑病患者,通过饮食和运动实现体重下降5%-10%,其银屑病皮损的严重程度通常能得到有临床意义的改善。
尽管这种方法需要较强的个人依从性且起效相对较慢,但重要性却不可替代,是后续药物干预的基础。
手术减重方案后银屑病的改善
回顾性研究显示,胃旁路术在减重之外,对银屑病有独特的改善作用。胃旁路术后,银屑病总体发病率下降约48%,重度银屑病风险下降56%,银屑病关节炎风险下降71%。
胃束带手术未见显著获益。这种差异提示GLP-1介导的代谢效应可能独立于减重本身。
GLP-1受体激动剂药物干预
减重又抗炎
当效果不佳或体重指数(BMI)达到一定标准时,可以考虑在医生指导下使用药物。其中,GLP-1受体激动剂是近年来应用较多的一类。这类药物通过中枢性抑制食欲、延缓胃排空来减轻体重。另外有研究显示,这类药物可能对改善全身代谢性炎症也有一定作用。
利拉鲁肽:一项针对合并2型糖尿病的银屑病患者的随机对照试验显示,使用利拉鲁肽治疗12周后,PASI评分和DLQI评分均显著优于对照组,且皮损组织中的IL-17、IL-23、TNF-α等炎症因子表达明显下降。这表明它在减重降糖之外,可能直接抑制了银屑病的关键炎症通路。它也是较早获批的减重药物。
司美格鲁肽:2025年的一项随机研究专门观察了肥胖合并2型糖尿病的银屑病患者。结果显示,司美格鲁肽治疗12周后,PASI评分中位数从21降至10,血清CRP和IL-6水平也显著下降,这证实了其系统性的抗炎作用。
替尔泊肽:是GIP/GLP-1双受体激动剂。在TOGETHER-PsO的研究中显示,替尔泊肽联合依奇珠单抗相比单用依奇珠单抗效果更优。联合组达到PASI 100+体重下降≥10%的比例为27.1%,单药组仅5.8%。联合组达到PASI 100的比例为40.6% ,而单药组为29.0%。这说明替尔泊肽联合银屑病生物制剂可能带来皮损与体重的协同改善。
关于GLP-1受体激动剂的副作用
最常见的的副作用是胃肠道反应,包括恶心、呕吐、腹泻、便秘、腹痛等,尤其在用药初期或增加剂量时,这可能影响用药的依从性。但多数患者的反应为轻至中度。
系统化的评估与管理流程
第一步:银屑病患者应常规测量BMI,并评估是否存在高血压、糖尿病、血脂异常等代谢并发症。
分层干预:
BMI≥25伴有合并症:应转至营养科,专业指导下进行。
BMI≥27伴有合并症,或 BMI ≥ 30:可考虑药物减重。GLP-1受体激动剂作为首选,因为它兼具减重与潜在抗炎。
BMI≥35伴有合并症,或 BMI ≥ 40:可考虑减重手术。
三类患者在治疗中应尤其关注体重管理:
高风险进展为银屑病关节炎的银屑病患者;
早期银屑病关节炎患者,此阶段是关键的干预窗口期;
对常规治疗反应不佳的难治性/治疗抵抗性银屑病关节炎患者。
伊顿健康结语
合并超重或肥胖的银屑病患者,综合性的体重管理是整体治疗方案中重要组成部分。应将体重变化与银屑病活动度、关节症状和代谢指标一起,作为定期随访的核心监测指标。
减重和治皮肤病一样,都是长期的事。效果要维持,副作用也要管,需要患者有足够的耐心和依从性。
肥胖银屑病患者应长期监测在皮肤科、风湿科、营养科及内分泌科医生的共同协作下制定个体化策略,可能有助于更好地控制病情。
临床前沿资讯:
如今银屑病领域创新药研发飞速发展,包括IL-17A抑制剂,IL-23 抑制剂、TYK2 抑制剂、JAK 抑制剂等多个靶点,生物制剂与口服靶向药均有大量临床研究持续推进。如需咨询前沿临床项目与新药动态,可在本公众号内发关键词:临床
感谢阅读,希望内容能对你有所帮助!
参考文献:
1.Shi Y, et al. Roles of glucagon-like peptide 1 receptor agonists in immune cell biology and autoimmune/autoinflammatory diseases. Cell Biosci.
2.Nicolau J, et al. Liraglutide improves psoriasis and psoriatic arthritis in obese patients: a prospective open-label cohort study. J Dermatolog Treat.
3.Petković-Dabić J, et al. Effects of Semaglutide Treatment on Psoriatic Lesions in Obese Patients with Type 2 Diabetes Mellitus: An Open-Label, Randomized Clinical Trial. J Clin Med.
4.Sontam A, et al. Glucagon-like peptide-1 receptor agonists in psoriasis and psoriatic arthritis: emerging evidence and future research opportunities. Expert Rev Clin Immunol.
5.Nature Reviews Rheumatology. Obesity and psoriasis: the role of GLP-1 receptor agonists. Nat Rev Rheumatol.
6.Buus NH, et al. Roux-en-Y gastric bypass surgery and risk of incident psoriasis and psoriatic arthritis: a nationwide cohort study. JAMA Dermatol.
7.American Diabetes Association. Standards of Care in Diabetes—2026. Diabetes Care.
8.National Psoriasis Foundation. Clinical guidance on the use of GLP-1 receptor agonists in patients with psoriasis and psoriatic arthritis. J Psoriasis Psoriatic Arthritis.
本文为伊顿健康服务的真实患者故事,仅做分享,不构成对任何药物或诊疗方案的推荐、推广或宣传,也不可替代专业医疗建议。如有问题,请咨询医疗卫生专业人士。材料图片等源自网络,侵删。
END
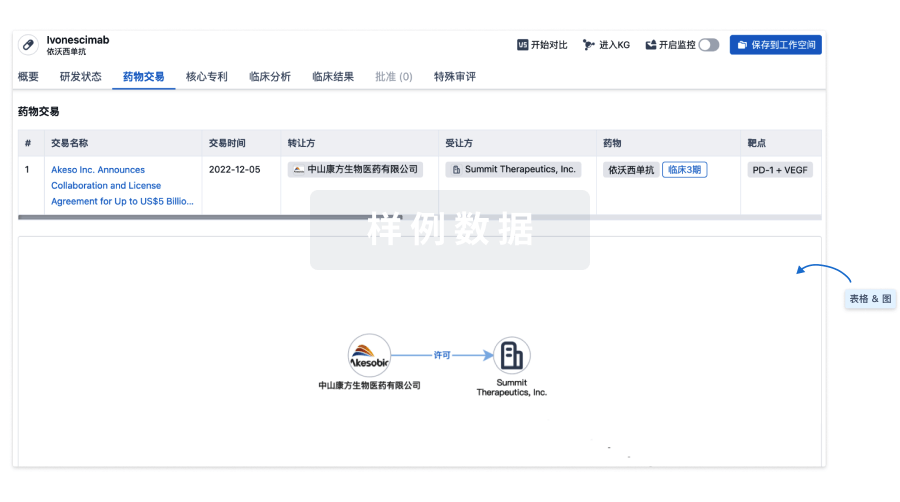
100 项与 JAK抑制剂(爱尔康制药) 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 干眼症 | 临床前 | 瑞士 | 2023-06-14 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
| 研究 | 分期 | 人群特征 | 评价人数 | 分组 | 结果 | 评价 | 发布日期 |
|---|
No Data | |||||||
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
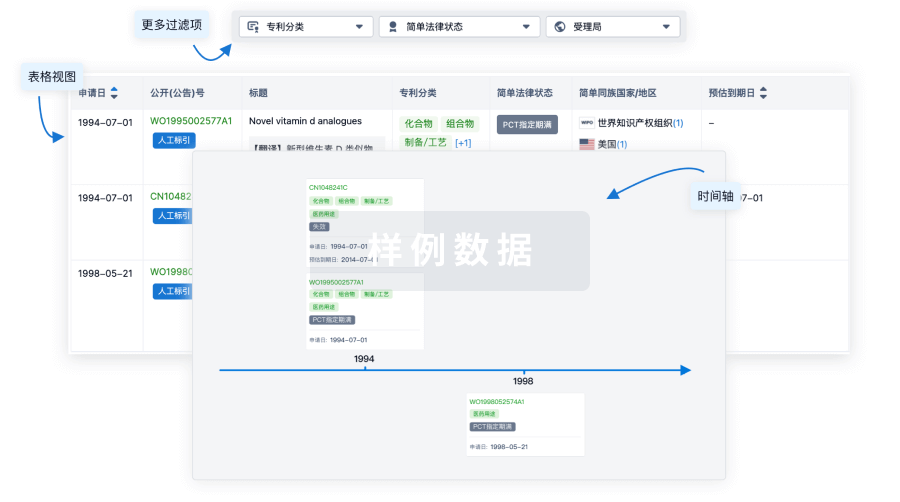
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
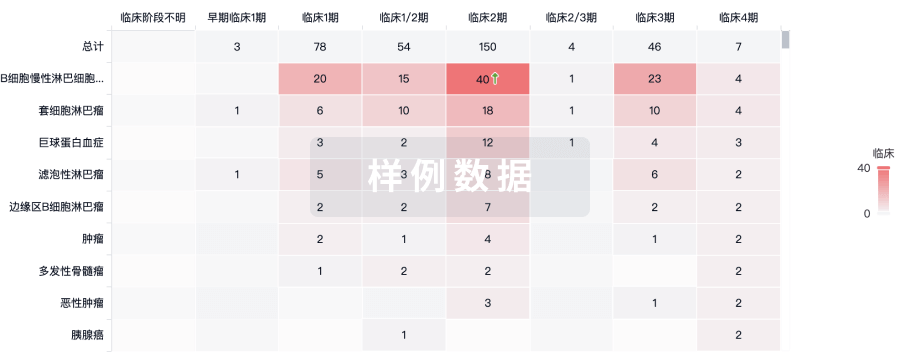
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用