预约演示
更新于:2026-06-16

Corcept Therapeutics, Inc.
更新于:2026-06-16
概览
标签
肿瘤
泌尿生殖系统疾病
内分泌与代谢疾病
小分子化药
化学药
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
NCT07553663
A Phase 1b, Open-Label Study Evaluating the Pharmacokinetics and Safety of Miricorilant in Adult Patients With Presumed Metabolic Dysfunction-Associated Steatohepatitis (MASH)
NCT07259317
A Phase 2, Single-Arm Trial of Relacorilant in Combination With Nab-Paclitaxel and Gemcitabine in Patients With Previously Untreated Metastatic Pancreatic Adenocarcinoma (TRIDENT)
NCT07276373
A Phase 1b/2, Open-Label, Dose-Finding and Proof of Concept Study of Nenocorilant in Combination With Anti-Programmed Cell Death/(Ligand) 1 in Patients With Advanced Solid Malignancies
100 项与 Corcept Therapeutics, Inc. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2024-11-04ONCOLOGIST
Relacorilant plus nab-paclitaxel for the treatment of metastatic pancreatic ductal adenocarcinoma: results from the open-label RELIANT study
Article
作者: Leal, Alexis D ; Skeel, Roland T ; Pashova, Hristina ; Fountzilas, Christos ; Mann, Grace ; Alese, Olatunji B ; Oberstein, Paul E ; Huyck, Timothy K ; Kio, Ebenezer A ; Noonan, Anne M ; Chiorean, Elena Gabriela ; Bahary, Nathan ; Lee, Valerie ; Borazanci, Erkut H ; Chung, Vincent ; Philip, Philip A ; Hanna, Wahid T ; Wainberg, Zev A ; Cardin, Dana B
Abstract:
Background:
Modulation of glucocorticoid receptor (GR) activity in tumor cells enhances chemotherapy efficacy. We evaluated the selective GR modulator relacorilant plus nab-paclitaxel in patients with metastatic pancreatic ductal adenocarcinoma (mPDAC) who had received at least 2 prior therapy lines.
Patients and Methods:
In this open-label, single-arm, phase III study, patients received once-daily oral relacorilant (100 mg, titrated to 150 mg in 25 mg increments/cycle) and nab-paclitaxel (80 mg/m2) on days 1, 8, and 15 of 28-day cycles. The primary efficacy endpoint was objective response rate (ORR) by blinded independent central review. Progression-free survival (PFS), overall survival (OS), target gene modulation, and safety were also assessed.
Results:
Of 43 patients enrolled, 31 were evaluable for ORR (12 did not reach first postbaseline radiographic assessment). An interim analysis to assess whether ORR was ≥10% showed no confirmed responses and the study was discontinued. Two (6.5%) patients attained unconfirmed partial responses and 15 (48.4%) had stable disease. Fourteen of 31 (45.2%) patients had reductions in target lesion size, despite prior nab-paclitaxel exposure in 12 of the 14. Median PFS and OS were 2.4 months (95% CI, 1.4-4.2) and 3.9 months (95% CI, 2.8-4.9), respectively. The most common adverse events were fatigue and nausea. RNA analysis confirmed that relacorilant plus nab-paclitaxel suppressed 8 cortisol target genes of interest.
Conclusion:
Relacorilant plus nab-paclitaxel showed modest antitumor activity in heavily pretreated patients with mPDAC, with no new safety signals. Studies of this combination in other indications with a high unmet medical need are ongoing.
2024-07-01BMJ Open
Study protocol for a prospective, multicentre study of hypercortisolism in patients with difficult-to-control type 2 diabetes (CATALYST): prevalence and treatment with mifepristone
Article
作者: Findling, James W ; Blonde, Lawrence ; Auchus, Richard J ; DeFronzo, Ralph A ; Frias, Juan P ; Buse, John B ; Fonseca, Vivian A ; Einhorn, Daniel ; Bancos, Irina ; Busch, Robert S ; Handelsman, Yehuda ; Rosenstock, Julio ; Tudor, Iulia Cristina ; Hamidi, Oksana ; Moraitis, Andreas G ; Pratley, Richard E
Introduction:
Even with recent treatment advances, type 2 diabetes (T2D) remains poorly controlled for many patients, despite the best efforts to adhere to therapies and lifestyle modifications. Although estimates vary, studies indicate that in >10% of individuals with difficult-to-control T2D, hypercortisolism may be an underlying contributing cause. To better understand the prevalence of hypercortisolism and the impact of its treatment on T2D and associated comorbidities, we describe the two-part Hyper
c
ortisolism in P
at
ients with Difficult to Control Type 2 Di
a
betes Despite Receiving Standard-of-Care Therapies: Preva
l
ence and Treatment with Korl
y
m
®
(Mifepri
st
one) (CATALYST) trial.
Methods and analysis:
In part 1, approximately 1000 participants with difficult-to-control T2D (haemoglobin A1c (HbA1c) 7.5%–11.5% despite multiple therapies) are screened with a 1 mg dexamethasone suppression test (DST). Those with post-DST cortisol >1.8 µg/dL and dexamethasone level ≥140 ng/dL are identified to have hypercortisolism (part 1 primary endpoint), have morning adrenocorticotropic hormone (ACTH) and dehydroepiandrosterone sulfate (DHEAS) measured and undergo a non-contrast adrenal CT scan. Those requiring evaluation for elevated ACTH are referred for care outside the study; those with ACTH and DHEAS in the range may advance to part 2, a randomised, double-blind, placebo-controlled trial to evaluate the impact of treating hypercortisolism with the competitive glucocorticoid receptor antagonist mifepristone (Korlym
®
). Participants are randomised 2:1 to mifepristone or placebo for 24 weeks, stratified by the presence/absence of an abnormal adrenal CT scan. Mifepristone is dosed at 300 mg once daily for 4 weeks, then 600 mg daily based on tolerability and clinical improvement, with an option to increase to 900 mg. The primary endpoint of part 2 assesses changes in HbA1c in participants with hypercortisolism with or without abnormal adrenal CT scan. Secondary endpoints include changes in antidiabetes medications, cortisol-related comorbidities and quality of life.
Ethics and dissemination:
The study has been approved by Cleveland Clinic IRB (Cleveland, Ohio, USA) and Advarra IRB (Columbia, Maryland, USA). Findings will be presented at scientific meetings and published in peer-reviewed journals.
Trial registration number:
NCT05772169
.
2024-01-01Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists
Relacorilant, a Selective Glucocorticoid Receptor Modulator in Development for the Treatment of Patients With Cushing Syndrome, Does Not Cause Prolongation of the Cardiac QT Interval
Article
作者: Custodio, Joseph M ; Kearney, Tara ; Donaldson, Kirsteen ; Pivonello, Rosario ; Feelders, Richard A ; Stigliano, Antonio ; Giordano, Roberta ; Darpo, Borje ; Lardo, Pina ; Ghigo, Ezio ; Mariash, Cary N ; Xue, Hongqi ; Mezősi, Emese ; Donegan, Diane M ; Hand, Austin L ; Moraitis, Andreas G
OBJECTIVE:
To assess the effect of relacorilant, a selective glucocorticoid receptor modulator under investigation for the treatment of patients with endogenous hypercortisolism (Cushing syndrome [CS]), on the heart rate-corrected QT interval (QTc).
METHODS:
Three clinical studies of relacorilant were included: (1) a first-in-human, randomized, placebo-controlled, ascending-dose (up to 500 mg of relacorilant) study in healthy volunteers; (2) a phase 1 placebo- and positive-controlled thorough QTc (TQT) study of 400 and 800 mg of relacorilant in healthy volunteers; and (3) a phase 2, open-label study of up to 400 mg of relacorilant administered daily for up to 16 weeks in patients with CS. Electrocardiogram recordings were taken, and QTc change from baseline (ΔQTc) was calculated. The association of plasma relacorilant concentration with the effect on QTc in healthy volunteers was assessed using linear mixed-effects modeling.
RESULTS:
Across all studies, no notable changes in the electrocardiogram parameters were observed. At all time points and with all doses of relacorilant, including supratherapeutic doses, ΔQTc was small, generally negative, and, in the placebo-controlled studies, similar to placebo. In the TQT study, placebo-corrected ΔQTc with relacorilant was small and negative, whereas placebo-corrected ΔQTc with moxifloxacin positive control showed rapid QTc prolongation. These results constituted a negative TQT study. The model-estimated slopes of the concentration-QTc relationship were slightly negative, excluding an association of relacorilant with prolonged QTc.
CONCLUSION:
At all doses studied, relacorilant consistently demonstrated a lack of QTc prolongation in healthy volunteers and patients with CS, including in the TQT study. Ongoing phase 3 studies will help further establish the overall benefit-risk profile of relacorilant.
2026-06-15
2026-06-06
100 项与 Corcept Therapeutics, Inc. 相关的药物交易
登录后查看更多信息
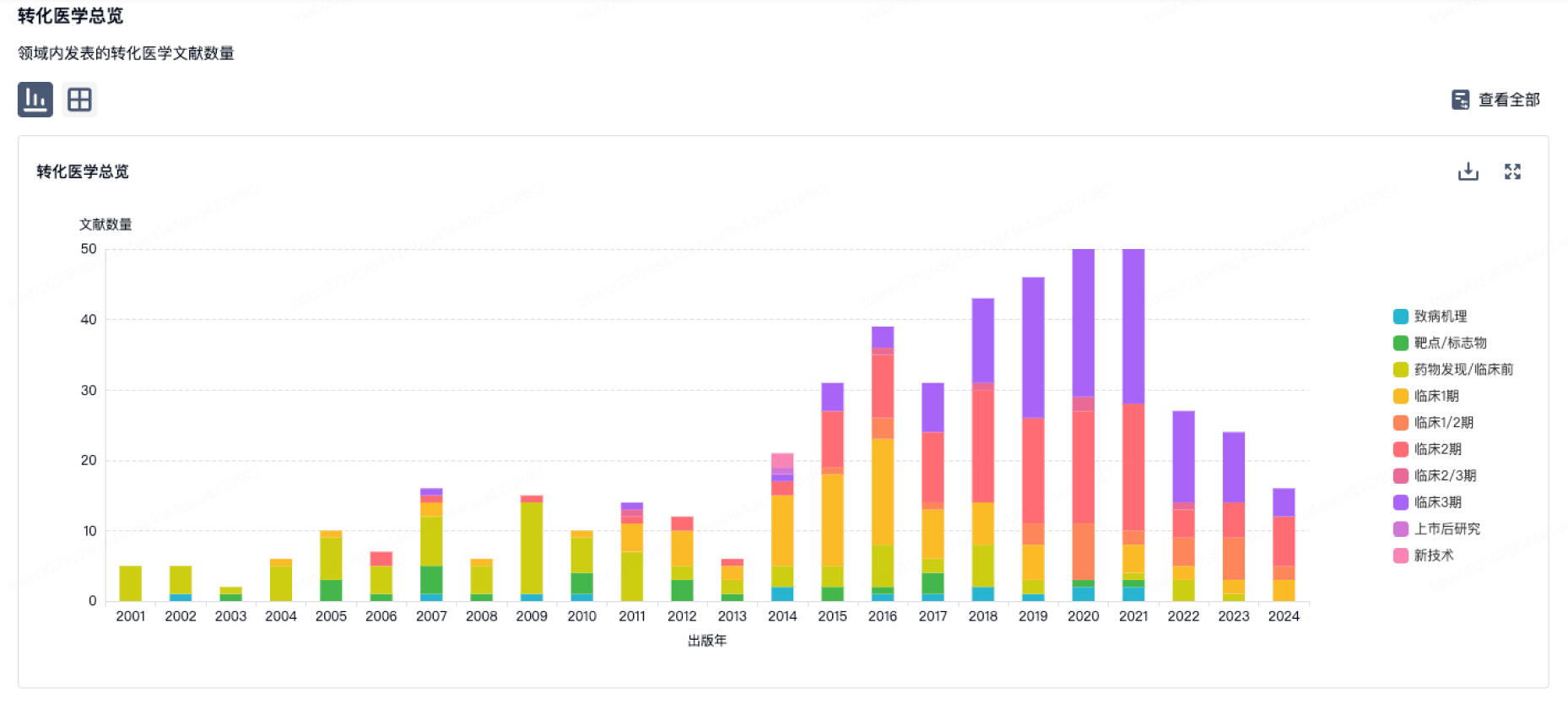
100 项与 Corcept Therapeutics, Inc. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月19日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
药物发现
1
1
临床1期
临床2期
3
2
批准上市
其他
5
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
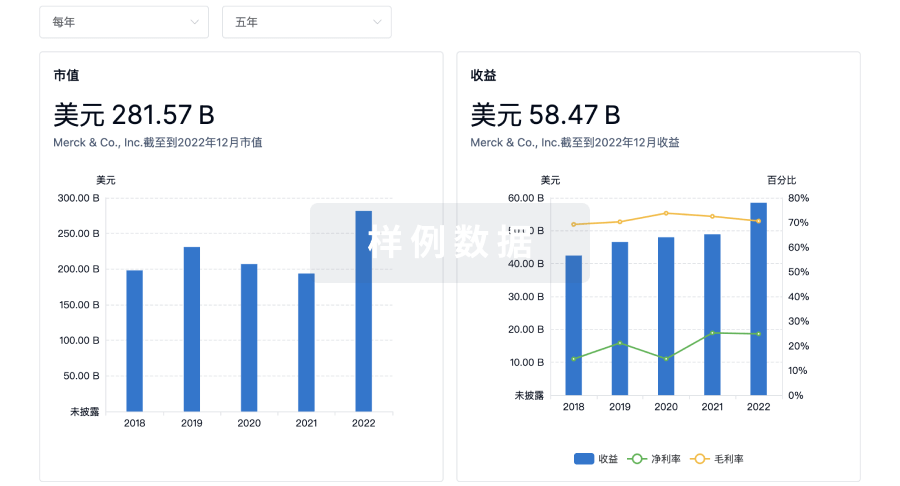
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用