预约演示
更新于:2025-05-07
ADRA2 x Prostanoid receptor
更新于:2025-05-07
基本信息
关联
2
项与 ADRA2 x Prostanoid receptor 相关的药物作用机制 ADRA2激动剂 [+2] |
在研机构- |
原研机构 |
在研适应症- |
最高研发阶段无进展 |
首次获批国家/地区- |
首次获批日期1800-01-20 |
作用机制 ADRA2激动剂 [+1] |
在研机构- |
原研机构 |
在研适应症- |
非在研适应症 |
最高研发阶段无进展 |
首次获批国家/地区- |
首次获批日期1800-01-20 |
4
项与 ADRA2 x Prostanoid receptor 相关的临床试验NCT01863953
A Safety and Efficacy Study of Fixed-Combination Bimatoprost and Brimonidine in Chronic Glaucoma or Ocular Hypertension
This is a safety and efficacy study of fixed-combination bimatoprost and brimonidine compared with LUMIGAN® and ALPHAGAN® in patients with chronic glaucoma or ocular hypertension.
开始日期2013-06-01 |
申办/合作机构 |
NCT01241240
Safety and Efficacy of Triple Combination Therapy in Patients With Primary Open-Angle Glaucoma or Ocular Hypertension
This study will evaluate the safety and efficacy of Triple Combination Therapy compared with Fixed Combination brimonidine tartrate/timolol ophthalmic solution in patients with primary open-angle glaucoma or ocular hypertension.
开始日期2011-03-01 |
申办/合作机构 |
NCT01217606
Safety and Efficacy of Triple Combination Therapy in Patients With Primary Open-Angle Glaucoma or Ocular Hypertension
This study will evaluate the safety and efficacy of Triple Combination Therapy compared with Fixed Combination brimonidine tartrate/timolol ophthalmic solution in patients with primary open-angle glaucoma or ocular hypertension.
开始日期2011-01-01 |
申办/合作机构 |
100 项与 ADRA2 x Prostanoid receptor 相关的临床结果
登录后查看更多信息
100 项与 ADRA2 x Prostanoid receptor 相关的转化医学
登录后查看更多信息
0 项与 ADRA2 x Prostanoid receptor 相关的专利(医药)
登录后查看更多信息
50
项与 ADRA2 x Prostanoid receptor 相关的文献(医药)2024-04-23·S.S. Korsakov Journal of Neurology and Psychiatry
Clinical and genetic associations in patients with non-cardioembolic ischemic stroke
Article
作者: Kolerova, I.V. ; Makhmudov, M.M. ; Gunchenko, A.S. ; Galkin, S.S. ; Anisimova, A.V. ; Nasedkina, T.V. ; Yutskova, E.V.
2021-05-01·Journal of Ocular Pharmacology and Therapeutics4区 · 医学
Additive Intraocular Pressure-Lowering Effects of a Novel Selective EP2 Receptor Agonist, Omidenepag Isopropyl, Combined with Existing Antiglaucoma Agents in Conscious Ocular Normotensive Monkeys
4区 · 医学
Article
作者: Shimazaki, Atsushi ; Shams, Naveed K. ; Odani-Kawabata, Noriko ; Taniguchi, Takazumi ; Kirihara, Tomoko ; Iwamura, Ryo ; Fuwa, Masahiro ; Kato, Masatomo ; Morishima, Kenji ; Yoneda, Kenji
2018-03-01·Journal of Thrombosis and Haemostasis2区 · 医学
Multiplate® evaluation of acetylsalicylic acid efficacy in carotid surgery: routine and genetic influencing factors
2区 · 医学
Article
作者: Labrouche, S ; Roullet, S ; Carrie, C ; Auque, H ; Berard, X ; Freyburger, G
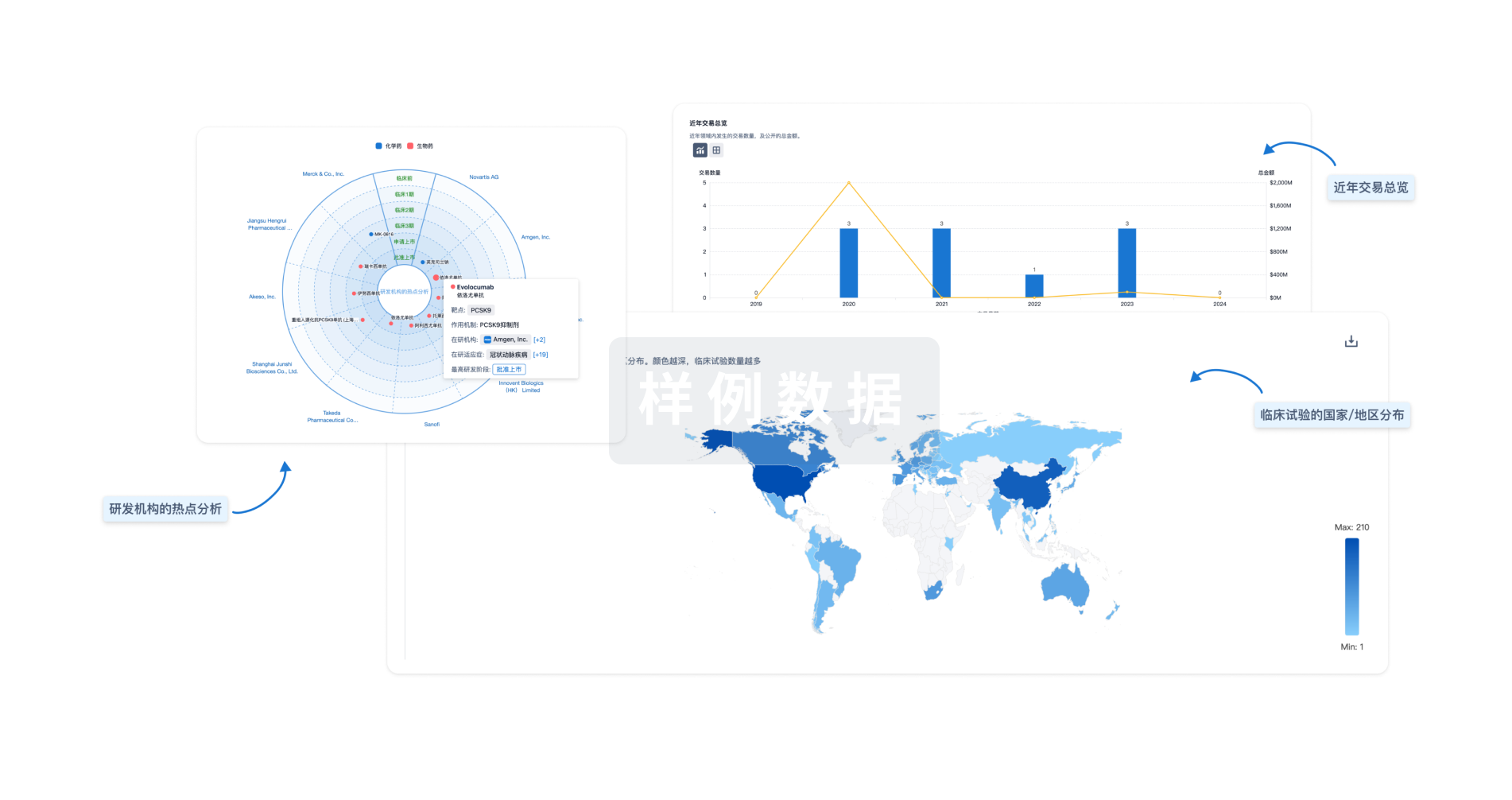
分析
对领域进行一次全面的分析。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用