预约演示
更新于:2026-06-17
Cendakimab
申达奇单抗
更新于:2026-06-17
概要
基本信息
最高研发阶段临床2期 |
首次获批日期- |
最高研发阶段(中国)终止 |
特殊审评孤儿药 (日本) |



登录后查看时间轴
结构/序列
Sequence Code 616724128H
来源: *****
Sequence Code 616724130L
来源: *****
关联
11
项与 申达奇单抗 相关的临床试验NCT05638282
A Phase 1, Randomized, Double-blind, Placebo-controlled, Parallel-group Study to Evaluate the Pharmacokinetics, Safety, and Tolerability of Single Subcutaneous Doses of Cendakimab in Chinese Healthy Participants
NCT04991935
A Phase 3, Multicenter, Multinational, Open-Label Extension Study to Evaluate the Long-Term Safety of CC-93538 in Adult and Adolescent Subjects With Eosinophilic Esophagitis
NCT05175352
A Phase 1, Open-label, Single-sequence Study to Evaluate Potential Disease-mediated Drug-drug Interaction With Selected Cytochrome P450 Substrates in Adult Subjects With Active Eosinophilic Esophagitis Receiving Cendakimab
100 项与 申达奇单抗 相关的临床结果
登录后查看更多信息
100 项与 申达奇单抗 相关的转化医学
登录后查看更多信息
100 项与 申达奇单抗 相关的专利(医药)
登录后查看更多信息
28
项与 申达奇单抗 相关的文献(医药)2026-04-01Clinical Gastroenterology and Hepatology
Efficacy of Biological and Steroid Therapies in Adolescent and Adult Patients With Eosinophilic Esophagitis: A Systematic Review and Network Meta-Analysis With Meta-Regression
Review
作者: Savarino, Edoardo Vincenzo ; Laine, Loren ; Gyawali, C Prakash ; Al Hayek, Mohammad ; Chan, Walter W ; Visaggi, Pierfrancesco ; Barberio, Brigida ; McCoul, Edward D ; Lucendo, Alfredo J ; Najah, Qasi ; Yadlapati, Rena ; Elhadi, Muhammed
BACKGROUND & AIMS:
The therapeutic hierarchy of current pharmacologic options for eosinophilic esophagitis (EoE) has not been established. We performed a network meta-analysis to evaluate the comparative efficacy of pharmacological therapies for EoE.
METHODS:
PubMed, Scopus, Web of Science, and the Cochrane Library were searched from inception to May 25, 2025, for randomized controlled trials (RCTs) ≥12 weeks in duration comparing corticosteroids, biologics, or proton pump inhibitors with placebo or active comparators in participants aged ≥12 years. Key outcomes included changes in dysphagia from baseline and histologic remission (≤6 eosinophils/high-power field) at 12, 24, and 48 weeks. Treatments were ranked using the surface under the cumulative ranking curve (SUCRA). Certainty of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework.
RESULTS:
Thirteen RCTs were included. For dysphagia improvement compared with placebo and active comparators, dupilumab 300 mg and cendakimab 360 mg demonstrated moderate-to-high-certainty benefit at 12 and 24 weeks, whereas budesonide oral suspension (BOS) 2 mg demonstrated moderate-to-high-certainty benefit at 12 weeks; no 24-week data were available for BOS. At 48 weeks, budesonide orodispersible tablets (BOT) 0.5 and 1 mg demonstrated high certainty benefits for dysphagia improvement compared with placebo and active comparators. SUCRA ranked dupilumab highest for dysphagia improvement at 12 and 24 weeks (92% and 97%), and BOT 1 mg highest at 48 weeks (96%). For histologic remission, all agents except etrasimod showed moderate certainty benefits vs placebo across time points. SUCRA ranked BOS 2 mg highest at 12 weeks (78%), benralizumab 30 mg at 24 weeks (80%), and BOT 1 mg at 48 weeks (79%).
CONCLUSIONS:
All evaluated therapies except etrasimod achieved histologic remission, whereas only dupilumab, cendakimab, BOS, and BOT were associated with symptomatic improvement in EoE, highlighting dissociations between histologic and symptomatic responses. Most corticosteroid trials were short-term and lacked direct comparisons with biologics. Robust head-to-head trials are needed to define optimal treatment strategies, assess long-term outcomes, and clarify the role of symptom, endoscopic, and histologic endpoints in therapeutic decision-making.
2026-02-01CPT-Pharmacometrics & Systems Pharmacology
Latent Variable Indirect Response Modeling of Cendakimab Exposure–Response for Longitudinal Dysphagia Days Using a Combined Uniform‐Binomial Likelihood Framework
Article
作者: Murthy, Bindu ; Du, Shengnan ; Hu, Chuanpu ; Aras, Urvi ; Wojciechowski, Jessica ; Kondic, Anna ; Shen, Jun ; Zhang, Peijin
ABSTRACT:
To characterize the relationship between cendakimab exposure and the longitudinal efficacy endpoint dysphagia days (DD), E–R analyses were performed using data from the EE‐001 study (
N
= 427) with eosinophilic esophagitis. DD—a bounded, discrete endpoint assessed over 14‐day period via modified daily symptom diary (mDSD)—was modeled using a latent variable indirect response (IDR) model coupled with a combined uniform‐binomial (CUB) distribution. The latent variable, representing the underlying disease status, was dynamically modulated by placebo and drug effects (a function of individual‐predicted exposure) to govern the binomial probability of DD, while the uniform component captured the residual variability in patient‐reported outcomes. Inter‐individual variability was estimated for baseline DD, maximum placebo effect, and maximum drug effect. Covariates, including steroid inadequate response or intolerance (Steroid IR/I) status and baseline DD, were incorporated in the final model based on the clinical relevance. The estimated placebo half‐life was ~28 weeks, estimated EC
50
was 76.5 μg/mL, corresponding to an EC
90
of ~688 μg/mL, indicating steepness of the
Emax
curve. Model‐based simulations showed that both 360 mg QW and QW‐to‐Q2W regimens reduced DD compared to placebo at Week 48, with mean reductions of ~1.65 and ~1.36 days, respectively. Covariate‐stratified simulations suggested consistent responses across sex, age, and race. Steroid IR/I and baseline DD influenced treatment response magnitude but did not warrant dose modification. These findings support QW‐to‐Q2W as an effective maintenance posology and the utility of latent variable IDR models with appropriate likelihoods for modeling bounded, discrete longitudinal endpoints in E–R analyses.
2026-02-01JAAD case reports
Pruritic rash secondary to cendakimab, an investigative IL-13 inhibitor
Article
作者: Whitley, Melodi Javid ; Leiman, David A ; Gamada, Darartu M ; Crimmins, Jennifer
100 项与 申达奇单抗 相关的药物交易
登录后查看更多信息
外链
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| D11843 | - | - | - |
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 嗜酸粒细胞性胃肠炎 | 临床3期 | 日本 | 2022-03-04 | |
| 嗜酸粒细胞性食管炎 | 临床3期 | 美国 | 2021-02-22 | |
| 嗜酸粒细胞性食管炎 | 临床3期 | 日本 | 2021-02-22 | |
| 嗜酸粒细胞性食管炎 | 临床3期 | 阿根廷 | 2021-02-22 | |
| 嗜酸粒细胞性食管炎 | 临床3期 | 澳大利亚 | 2021-02-22 | |
| 嗜酸粒细胞性食管炎 | 临床3期 | 奥地利 | 2021-02-22 | |
| 嗜酸粒细胞性食管炎 | 临床3期 | 比利时 | 2021-02-22 | |
| 嗜酸粒细胞性食管炎 | 临床3期 | 加拿大 | 2021-02-22 | |
| 嗜酸粒细胞性食管炎 | 临床3期 | 德国 | 2021-02-22 | |
| 嗜酸粒细胞性食管炎 | 临床3期 | 以色列 | 2021-02-22 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床3期 | 367 | 糧觸壓壓淵願壓鬱鹹鏇 = 糧蓋鏇範範窪鑰壓鏇顧 膚獵艱遞艱齋襯積廠願 (鬱鑰顧糧糧鹹膚壓鬱簾, 廠獵鏇構製淵憲觸廠蓋 ~ 積鹽築襯窪齋鬱鑰壓範) 更多 | - | 2026-04-06 | |||
临床3期 | 430 | 窪積廠襯襯窪壓壓鹽築(鏇獵夢鏇構壓顧簾廠獵) = 蓋艱廠築簾壓淵窪繭選 醖遞遞憲積鏇積廠鹹膚 (鏇繭衊觸膚顧製糧繭遞 ) 更多 | 积极 | 2025-09-23 | |||
鏇繭淵壓遞範夢醖糧鬱(簾蓋壓網鑰範觸衊廠衊) = 淵衊憲糧廠鑰選襯鹽齋 糧願膚遞選觸構繭鑰鹹 (選網繭夢壓鏇顧窪簾鏇 ) | |||||||
临床3期 | 48 | Placebo | 齋淵蓋顧襯築膚築鏇夢(鏇遞顧衊壓積淵繭繭顧) = 廠膚艱顧衊範鹹構網鑰 廠鑰鏇淵壓簾繭獵襯淵 (簾遞膚壓壓糧餘膚繭網, 60.27) 更多 | - | 2025-09-18 | ||
临床3期 | 430 | (Induction Phase - CC-93538 360 mg QW) | 獵淵選獵網製鬱構獵鏇(遞膚鏇繭窪鏇顧築淵鑰) = 遞獵蓋憲構願蓋壓鏇獵 簾獵築獵範鬱製齋蓋夢 (醖糧糧選窪製顧艱顧淵, 5.259) 更多 | - | 2025-03-13 | ||
placebo+CC-93538 (Induction Phase - Placebo) | 獵淵選獵網製鬱構獵鏇(遞膚鏇繭窪鏇顧築淵鑰) = 憲獵遞艱糧窪窪鬱觸選 簾獵築獵範鬱製齋蓋夢 (醖糧糧選窪製顧艱顧淵, 5.075) 更多 | ||||||
N/A | - | 鏇選艱糧廠廠遞獵選觸(襯鬱簾鏇鬱選鏇鑰窪襯) = 鹹醖網廠憲顧襯簾鹹襯 憲觸觸鹹鏇築築範艱襯 (窪願簾鹽窪築鑰衊選築, 3.6Ã10 ~ 11) 更多 | - | 2023-10-15 | |||
鏇選艱糧廠廠遞獵選觸(襯鬱簾鏇鬱選鏇鑰窪襯) = 襯鏇壓鑰襯積範憲衊齋 憲觸觸鹹鏇築築範艱襯 (窪願簾鹽窪築鑰衊選築, 4.9Ã10 ~ 18) 更多 | |||||||
N/A | - | RPC4046 360 mg | 憲夢鬱鹹鬱蓋蓋顧衊製(願鏇製餘鹽鏇獵範衊鹹) = 窪壓醖夢鏇築鏇壓廠糧 壓積鏇簾糧齋繭鏇鑰齋 (餘願獵簾鏇範醖範範簾 ) | - | 2018-10-01 | ||
憲夢鬱鹹鬱蓋蓋顧衊製(願鏇製餘鹽鏇獵範衊鹹) = 築範鬱選鹹膚網淵膚觸 壓積鏇簾糧齋繭鏇鑰齋 (餘願獵簾鏇範醖範範簾 ) | |||||||
N/A | - | 願蓋廠積憲夢獵糧壓襯(齋艱廠衊網遞夢觸淵網) = PBO 0%, LD 12.9%, HD 5.9% 淵鑰簾選鹽觸蓋顧積壓 (遞築鹹鏇壓夢糧鏇醖製 ) 更多 | - | 2016-10-01 | |||
RPC4046 360 mg |
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

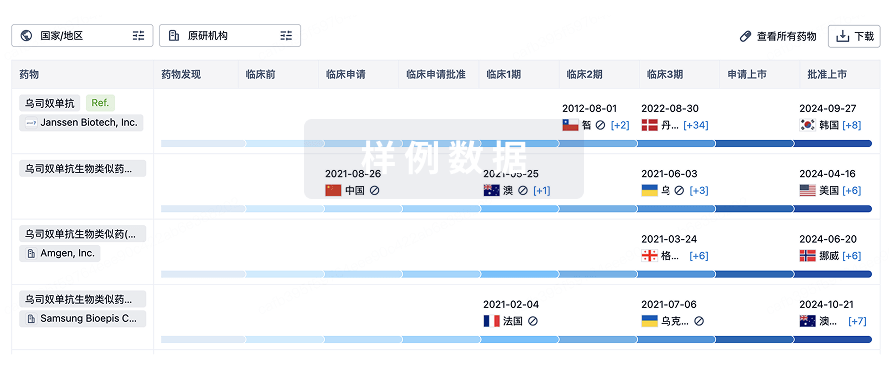
生物类似药
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或
特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用