预约演示
更新于:2026-05-18
BCMA CAR-T cells(Shenzhen Geno-Immune Medical Institute)
更新于:2026-05-18
概要
基本信息
原研机构 |
在研机构 |
非在研机构- |
权益机构- |
最高研发阶段临床1/2期 |
首次获批日期- |
最高研发阶段(中国)临床1/2期 |
特殊审评- |
登录后查看时间轴
关联
2
项与 BCMA CAR-T cells(Shenzhen Geno-Immune Medical Institute) 相关的临床试验NCT06429150
Frontline Management of High-Risk Multiple Myeloma or Plasmacytoma With BCMA and GPRC5D Combination CAR-T Cell Therapy
NCT03271632
Multiple Antigen-specific CAR T Cells For the Treatment of Multiple Myeloma
100 项与 BCMA CAR-T cells(Shenzhen Geno-Immune Medical Institute) 相关的临床结果
登录后查看更多信息
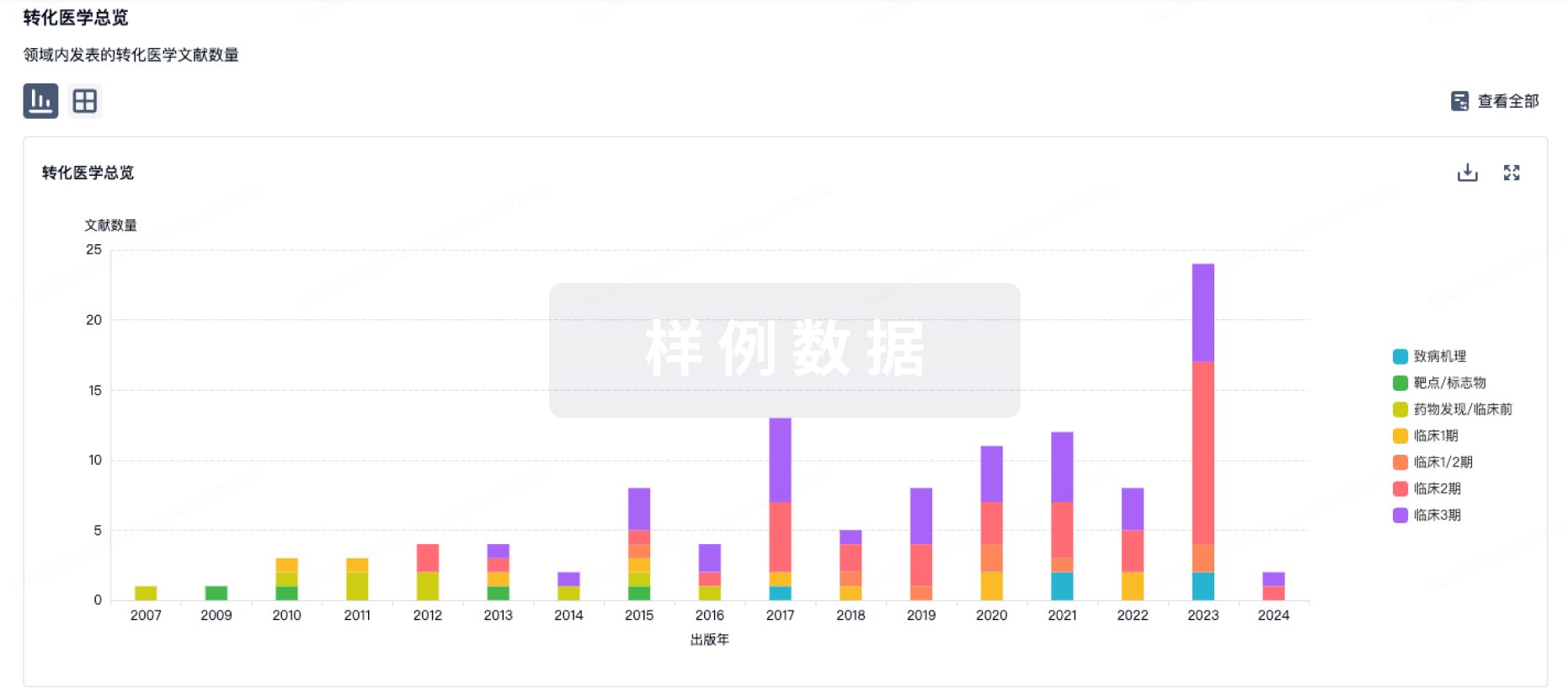
100 项与 BCMA CAR-T cells(Shenzhen Geno-Immune Medical Institute) 相关的转化医学
登录后查看更多信息
100 项与 BCMA CAR-T cells(Shenzhen Geno-Immune Medical Institute) 相关的专利(医药)
登录后查看更多信息
17
项与 BCMA CAR-T cells(Shenzhen Geno-Immune Medical Institute) 相关的文献(医药)2025-06-01NATURE MEDICINE
BCMA CAR T cells in a patient with relapsing idiopathic inflammatory myositis after initial and repeat therapy with CD19 CAR T cells
Article
作者: Müller, Fabian ; Wirsching, Andreas ; Grieshaber-Bouyer, Ricardo ; Spörl, Silvia ; Völkl, Simon ; Schett, Georg ; Hagen, Melanie ; Atzinger, Armin ; Böltz, Sebastian ; Zhang, Liang ; Kretschmann, Sascha ; Bucci, Laura ; Taubmann, Jule ; Mackensen, Andreas ; Raimondo, Maria Gabriella ; Tur, Carlo ; Eckstein, Markus ; Aigner, Michael ; Kharboutli, Soraya ; Munoz, Luis
Abstract:
CD19 chimeric antigen receptor (CD19 CAR) T cell therapy has been shown to induce stable drug-free remission in patients with refractory autoimmune disease. The management of potential relapses is currently unclear. Here we report on a 45-year-old woman with treatment-refractory Jo-1-associated anti-synthetase syndrome, who initially achieved disease remission after CD19 CAR T cell therapy but then experienced disease relapse after 9 months. After reinfusion of the same product, CAR T cells failed to expand and T cells targeting the CD19 CAR were detected. Despite full-dose lymphodepletion, no clinical response was observed. After bridging with anti-CD38 antibody daratumumab, which was efficacious with limited durability, plasma-cell-targeting B-cell maturation antigen (BCMA) CAR T cell therapy was performed. BCMA CAR T cells expanded, cleared plasma cells in lymphoid tissue, reduced autoantibody levels and re-induced stable drug-free remission. This case highlights the challenges in CAR T cell reinfusion, the potential of alternative targets and products, and suggests that the depletion of plasma cells may enhance therapeutic outcomes in patients who become treatment-refractory.
2024-11-01NATURE IMMUNOLOGY
Targeting systemic IL-2 to BCMA CAR-T cells
Article
作者: Sadelain, Michel ; Shi, Yuzhe
A review.CAR-T cells are revolutionizing the treatment of cancer and other diseases.A latest iteration in development involves fusion with an antigen-based CAR enhancer to provide low-affinity IL-2 signaling that might limit adverse effects.
2024-04-01Journal for immunotherapy of cancer
PD-1 downregulation enhances CAR-T cell antitumor efficiency by preserving a cell memory phenotype and reducing exhaustion
Article
作者: Mi, Jian-Qing ; Wang, Yan ; Ouyang, Wanyan ; Liu, Yuanfang ; Wang, Jin ; Zhao, Han ; Liu, Wei-Yang ; Xu, Nan ; Tao, Yi ; Liu, Feng ; Kang, Liqing ; Jin, Shi-Wei ; Liu, Zhiqiang ; Yu, Lei ; Zhang, Liuqingqing
Background:
Despite the encouraging outcome of chimeric antigen receptor T cell (CAR-T) targeting B cell maturation antigen (BCMA) in managing relapsed or refractory multiple myeloma (RRMM) patients, the therapeutic side effects and dysfunctions of CAR-T cells have limited the efficacy and clinical application of this promising approach.
Methods:
In this study, we incorporated a short hairpin RNA cassette targeting PD-1 into a BCMA-CAR with an OX-40 costimulatory domain. The transduced PD-1KD BCMA CAR-T cells were evaluated for surface CAR expression, T-cell proliferation, cytotoxicity, cytokine production, and subsets when they were exposed to a single or repetitive antigen stimulation. Safety and efficacy were initially observed in a phase I clinical trial for RRMM patients.
Results:
Compared with parental BCMA CAR-T cells, PD-1KD BCMA CAR-T cell therapy showed reduced T-cell exhaustion and increased percentage of memory T cells in vitro. Better antitumor activity in vivo was also observed in PD-1KD BCMA CAR-T group. In the phase I clinical trial of the CAR-T cell therapy for seven RRMM patients, safety and efficacy were initially observed in all seven patients, including four patients (4/7, 57.1%) with at least one extramedullary site and four patients (4/7, 57.1%) with high-risk cytogenetics. The overall response rate was 85.7% (6/7). Four patients had a stringent complete response (sCR), one patient had a CR, one patient had a partial response, and one patient had stable disease. Safety profile was also observed in these patients, with an incidence of manageable mild to moderate cytokine release syndrome and without the occurrence of neurological toxicity.
Conclusions:
Our study demonstrates a design concept of CAR-T cells independent of antigen specificity and provides an alternative approach for improving the efficacy of CAR-T cell therapy.
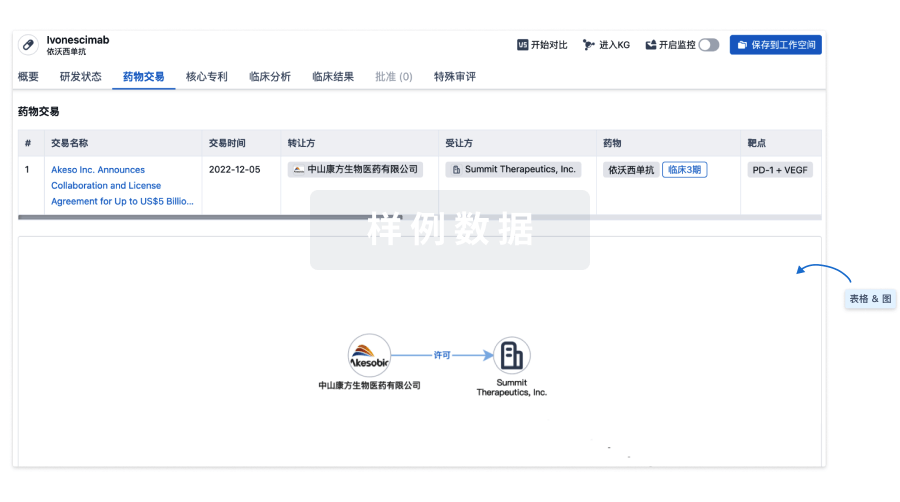
100 项与 BCMA CAR-T cells(Shenzhen Geno-Immune Medical Institute) 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 浆细胞瘤 | 临床2期 | 中国 | 2024-05-11 | |
| 浆细胞瘤 | 临床2期 | 俄罗斯 | 2024-05-11 | |
| 多发性骨髓瘤 | 临床2期 | 中国 | 2017-07-15 | |
| 浆细胞白血病 | 临床2期 | 中国 | 2017-07-15 | |
| 复发性多发性骨髓瘤 | 临床2期 | 中国 | 2017-07-15 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
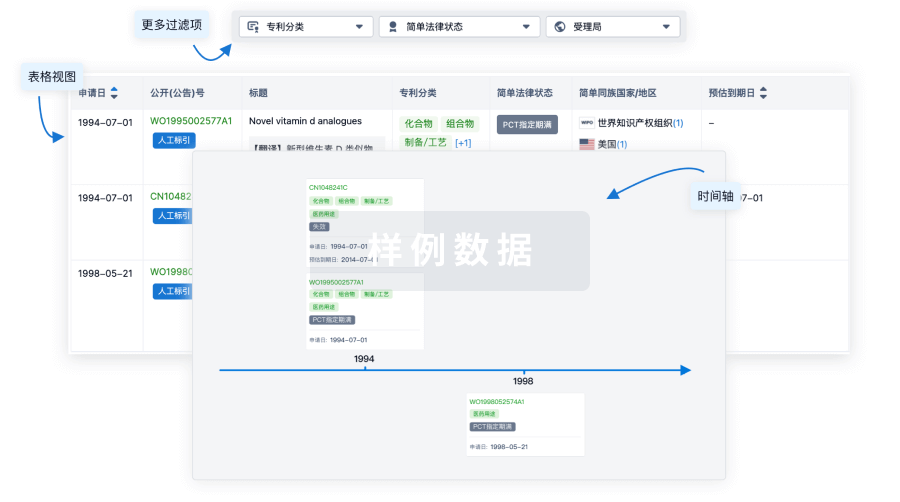
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
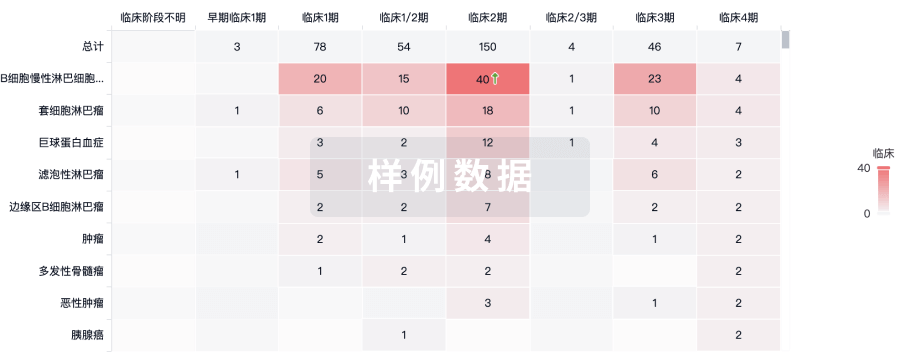
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用