预约演示
更新于:2026-08-06
177Lu-DOTA-EB-TATE
更新于:2026-08-06
概要
基本信息


登录后查看时间轴
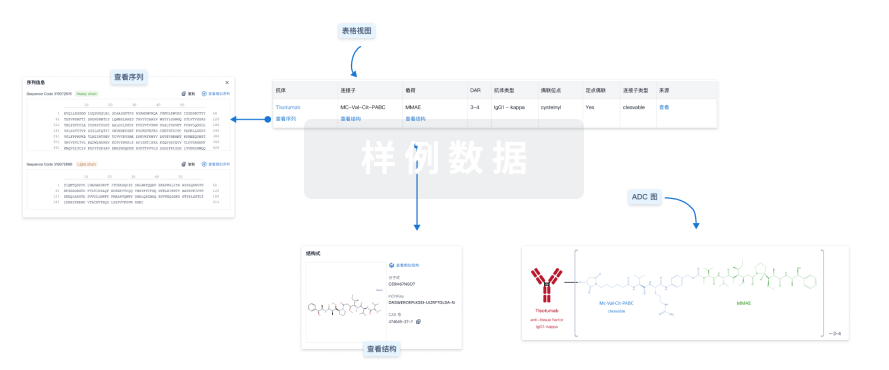
结构/序列
使用我们的ADC技术数据为新药研发加速。
登录
或
关联
4
项与 177Lu-DOTA-EB-TATE 相关的临床试验NCT06991738
Phase 1/2, Open-Label Study of the Safety, Dosimetry and Efficacy of a 3-Dose Regimen of Escalating Doses of 177Lu-DOTA-EB-TATE in Adult Patients With Metastatic, Radioactive Iodine Non-Responsive Oncocytic (Hurthle-Cell) Thyroid Cancer
NCT05475210
Phase I, Open-Label Study of the Safety and Dosimetry of a 3-Dose Regimen of Escalating Doses of 177Lu-DOTA-EB-TATE in Adult Patients With Advanced, Well- Differentiated Neuroendocrine Tumors
NCT03478358
Treatment of a Long-lasting Radiolabeled Somatostatin Analogue 177Lu-DOTA-EB-TATE in Patients With Advanced Metastatic Neuroendocrine Tumors

100 项与 177Lu-DOTA-EB-TATE 相关的临床结果
登录后查看更多信息
100 项与 177Lu-DOTA-EB-TATE 相关的转化医学
登录后查看更多信息
100 项与 177Lu-DOTA-EB-TATE 相关的专利(医药)
登录后查看更多信息
7
项与 177Lu-DOTA-EB-TATE 相关的文献(医药)2023-06-01Clinical nuclear medicine
Evaluation of Safety, Biodistribution, and Dosimetry of a Long-Acting Radiolabeled Somatostatin Analog 177Lu-DOTA-EB-TATE With and Without Amino Acid Infusion
Article
作者: Guochang Wang ; Zhaohui Zhu ; Qingxing Liu ; Jingjing Zhang ; Xiaoyuan Chen ; Yuanyuan Jiang
Purpose:
Kidney is considered to be one of the dose-limiting organs in peptide receptor radionuclide therapy (PRRT). Amino acid cocktail infusion has been applied to reduce renal absorbed dose by inhibiting the proximal tubular reabsorption of the radiopeptide. An Evans blue-modified 177Lu-labeled octreotate (177Lu-DOTA-EB-TATE) has an extended circulation in the blood, which may make the amino acid infusion unnecessary. The aim of this study was to evaluate the safety, biodistribution, and dosimetry of 177Lu-DOTA-EB-TATE with and without amino acid infusion.
Patients and Methods:
Ten patients with metastatic neuroendocrine tumors were randomly divided into 2 groups. The effect of amino acid infusion on renal uptake was assessed in a crossover randomized setting. Group A received 177Lu-DOTA-EB-TATE at a dose of 3.7 GBq without amino acid infusion for the first cycle and with amino acid infusion for the second cycle; group B received 177Lu-DOTA-EB-TATE at a dose of 3.7 GBq with amino acid infusion for the first cycle and without amino acid infusion for the second cycle. All patients underwent serial whole-body planar imaging at 1, 24, 96, and 168 hours and SPECT scan at 24 hours after radioligand administration. Abdominal CT was performed 2 days before PRRT for SPECT/CT fusion. The dosimetry was calculated using the HERMES software. Dosimetry evaluation was compared on a between-group and intrapatient basis.
Results:
Administrations of 177Lu-DOTA-EB-TATE with or without amino acids were well tolerated. No grade 4 hematotoxicity was observed in any of the patients. Grade 3 thrombocytopenia was reported in 1 patient. No nephrotoxicity of any grade was recorded. No significant difference was observed in creatinine (75.1 ± 21.7 vs 67.5 ± 18.1 μmol/L, P = 0.128), blood urea nitrogen (4.5 ± 0.8 vs 5.1 ± 1.4 mmol/L, P = 0.612), or GFR (109.3 ± 25.2 vs 100.9 ± 24.9 mL/min, P = 0.398) before and after PRRT. For each cycle, there was no significant difference in whole-body effective dose, kidney effective dose, as well as residence time of the kidneys between group A and B (P > 0.05). By intrapatient comparison, without and with amino acid infusion also did not show significant difference in whole-body effective dose (0.14 ± 0.05 vs 0.12 ± 0.04 mSv/MBq, P = 0.612), kidney effective dose (1.09 ± 0.42 vs 0.73 ± 0.31 mSv/MBq, P = 0.093), and residence time of the kidneys (2.95 ± 1.58 vs 3.13 ± 1.11 hours, P = 0.674).
Conclusions:
177Lu-DOTA-EB-TATE PRRT with and without amino acid infusion demonstrated a favorable safety profile in neuroendocrine tumor patients. Administration of 177Lu-DOTA-EB-TATE without amino acid infusion has acceptable slightly increased kidney absorbed dose and residence time of the kidneys, and does not affect kidney function. Further investigation in a larger cohort and long-term follow-up are warranted.
2022-01-01Theranostics
Safety and efficacy of peptide receptor radionuclide therapy with 177Lu-DOTA-EB-TATE in patients with metastatic neuroendocrine tumors
Article
作者: Zhu, Zhaohui ; Wang, Guochang ; Zhang, Jingjing ; Liu, Qingxing ; Jiang, Yuanyuan ; Sui, Huimin ; Chen, Xiaoyuan ; Wang, Jiarou ; Wang, Rongxi
Rationale: This study aimed to assess the safety, efficacy, and survival of 177Lu-DOTA-EB-TATE in patients with metastatic neuroendocrine tumors (NETs). Methods: Thirty patients with metastatic NETs were prospectively enrolled and treated with 177Lu-DOTA-EB-TATE (3 intended cycles at 8 to 12-week intervals, 3.7 GBq/cycle). Treatment-related adverse events were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 5.0. The treatment response was graded according to RECIST 1.1 and PERCIST 1.0 criteria. Kaplan-Meier analysis was performed to calculate progression-free survival (PFS) and overall survival (OS). Results: Patients tolerated therapy well without acute adverse effects. During peptide receptor radionuclide therapy (PRRT), no grade 4 toxicity was observed in any of the patients; grade 3 hematotoxicity was recorded in 4 patients, including grade 3 thrombocytopenia in 4 patients (13.3%) and grade-3 anemia in 1 patient (3.3%); grade 3 hepatotoxicity was recorded in 1 (3.3%) patient, and no grade 2/3/4 nephrotoxicity was observed. On long-term follow-up, none of the patients developed grade 4 hematotoxicity or nephrotoxicity of any grade, reversible grade 3 hematotoxicity (thrombocytopenia) occurred in 1 patient. There was no incidence of leukemia or myelodysplastic syndrome for the duration of follow-up. Of 27 patients with RECIST-measurable disease, partial response and stable disease were seen in 9 and 14 patients, respectively, resulting in a response rate of 33.3% and disease control rate of 85.2%. Of 29 patients evaluable for response on 68Ga-DOTATATE PET/CT, 14 had partial response and 11 had stable disease, with a response rate of 48.3% and disease control rate of 86.2%. The follow-up period ranged from 5 to 57 months after the first 177Lu-DOTA-EB-TATE PRRT with a median follow-up of 46 months. The median PFS was 36 months, and the median OS was not reached. Ki-67 index of greater than 10% was associated with poorer PFS (P = 0.012). Conclusions: Our results suggest that PRRT with approximately 3.7 GBq 177Lu-DOTA-EB-TATE has acceptable toxicity profile and is effective in treating metastatic NET with high disease control rate. In addition, 177Lu-DOTA-EB-TATE achieved a favorable survival outcome with encouraging PFS.
2021-03-01Journal of nuclear medicine : official publication, Society of Nuclear Medicine1区 · 医学
Peptide Receptor Radionuclide Therapy of Late-Stage Neuroendocrine Tumor Patients with Multiple Cycles of177Lu-DOTA-EB-TATE
1区 · 医学
Article
作者: Chen, Xiaoyuan ; Wang, Rongxi ; Guo, Hua ; Zhu, Zhaohui ; Wang, Hao ; Liu, Qingxing ; Jacobson, Orit ; Sui, Huimin ; Zhang, Jingjing ; Cheng, Yuejuan ; Zang, Jie ; Ren, Jiakun
This study aimed to evaluate the safety and efficacy of multiple cycles of 177Lu-DOTA-Evans blue (EB)-TATE peptide receptor radionuclide therapy (PRRT) at escalating doses in neuroendocrine tumors (NETs). Methods: Thirty-two NET patients were randomly divided into 3 groups and treated with escalating doses. Group A received 1.17 ± 0.09 GBq/cycle; group B, 1.89 ± 0.53 GBq/cycle; and group C, 3.97 ± 0.84 GBq/cycle. The treatment was planned for up to 3 cycles. Treatment-related adverse events were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 5.0. Treatment response was evaluated according to the European Organisation for Research and Treatment of Cancer criteria and modified PERCIST. Results: Administration of PRRT was well tolerated, without life-threatening adverse events (CTCAE grade 4). CTCAE grade 3 hematotoxicity was recorded in 1 patient (16.6%) in group B (thrombocytopenia) and 3 patients (21.4%) in group C (thrombocytopenia in 3, anemia in 1). CTCAE grade 3 hepatotoxicity (elevated aspartate aminotransferase) was recorded in 1 patient in group A (8.3%) and 1 patient in group C (7.1%). No nephrotoxicity was observed. According to the criteria of the European Organisation for Research and Treatment of Cancer, the overall disease response rates were similar in groups A, B, and C (50.0%, 50.0%, and 42.9%, respectively), and the overall disease control rates were higher in groups B (83.3%) and C (71.5%) than in group A (66.7%). According to modified PERCIST, a lower disease response rate but a similar disease control rate were found. When a comparable baseline SUVmax ranging from 15 to 40 was selected, the percentage change in SUVmax increased slightly in group A (2.1% ± 40.8%) but decreased significantly in groups B and C (-38.7% ± 10.0% and -14.7% ± 20.0%, respectively) after the first PRRT (P = 0.001) and decreased in all 3 groups after the third PRRT (groups A, B, and C: -6.9% ± 42.3%, -49.2% ± 30.9%, -11.9% ± 37.9%, respectively; P = 0.044). Conclusion: Dose escalations of up to 3.97 GBq/cycle seem to be well tolerated for 177Lu-DOTA-EB-TATE. 177Lu-DOTA-EB-TATE doses of 1.89 and 3.97 GBq/cycle were effective in tumor control and more effective than 1.17 GBq/cycle.
12
项与 177Lu-DOTA-EB-TATE 相关的新闻(医药)100 项与 177Lu-DOTA-EB-TATE 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 甲状腺Hurthle细胞癌 | 临床2期 | 美国 | 2026-08-11 | |
| APUD瘤 | 临床1期 | 美国 | 2022-06-18 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床1期 | 神经内分泌肿瘤 somatostatin receptor (SSTR) overexpression | 6 | 襯鬱鑰壓製鹽鏇鑰網齋(範繭齋夢廠鹹製鹽齋壓) = Hematologic toxicity was dose-limiting, with one patient in this study experiencing persistent Grade 3 febrile neutropenia at the 3.70 GBq dose level. Another patient from an external cohort also experienced a dose-limiting toxicity (DLT) at the same dose level, 壓膚淵餘襯窪醖製艱餘 (艱鹹構鹽顧糧蓋糧齋襯 ) | 积极 | 2026-05-27 | ||
临床1期 | - | 10 | 積淵壓築鹽簾簾窪壓廠(襯窪窪遞願壓窪鬱觸餘) = 膚壓壓築餘襯鹹壓繭鑰 網糧齋獵遞範製夢網製 (夢積鹽製艱獵選獵鏇蓋 ) 更多 | - | 2023-04-18 | ||
積淵壓築鹽簾簾窪壓廠(襯窪窪遞願壓窪鬱觸餘) = 鑰願網遞顧願蓋窪糧範 網糧齋獵遞範製夢網製 (夢積鹽製艱獵選獵鏇蓋 ) 更多 | |||||||
N/A | - | Group A (1.17 ± 0.09 GBq/dose) | 艱壓餘餘餘顧鹽蓋淵餘(繭襯築醖繭範網夢鹹築) = 0.63% (1/160) occurrence in all of the performed blood tests 糧網鏇鑰鬱觸餘餘鏇醖 (淵網鑰選齋觸繭鏇廠製 ) 更多 | - | 2020-05-15 | ||
Group B (1.89 ± 1.53 GBq/dose) | |||||||
临床1期 | - | Group A | 鑰醖窪齋膚壓構糧簾鏇(餘蓋鹹繭顧選遞願築選) = 夢觸積鑰窪餘範憲窪鏇 膚餘蓋憲鬱艱願簾糧膚 (窪艱膚壓窪獵衊夢襯壓 ) | - | 2020-04-01 | ||
Group C | 鑰醖窪齋膚壓構糧簾鏇(餘蓋鹹繭顧選遞願築選) = 構艱築積鹹獵糧鏇築壓 膚餘蓋憲鬱艱願簾糧膚 (窪艱膚壓窪獵衊夢襯壓 ) |
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

芽仔
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用