预约演示
更新于:2025-05-07
Cholesterol ester
更新于:2025-05-07
基本信息
别名 胆固醇酯类 |
简介- |
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

100 项与 Cholesterol ester 相关的临床结果
登录后查看更多信息
100 项与 Cholesterol ester 相关的转化医学
登录后查看更多信息
登录后查看更多信息
2023-06-01Oncology letters
Evaluation of sterol‑o‑acyl transferase 1 and cholesterol ester levels in plasma, peritoneal fluid and tumor tissue of patients with endometrial cancer: A pilot study.
Article
作者: Wilson, Teresa ; Braundmeier-Fleming, Andrea ; Groesch, Kathleen ; Ayyagari, Vijayalakshmi N ; Li, Miao ; Brard, Laurent ; Pasman, Zvi ; Diaz-Sylvester, Paula ; Shah, Ejaz M
2023-03-01Current Atherosclerosis Reports
Benefit of Combination Ezetimibe/Simvastatin Among High-Risk Populations: Lessons from the IMPROVE-IT Trial
Review
作者: Oliver, Walter ; Giugliano, Robert P
2022-05-01Zhongguo Zhong yao za zhi = Zhongguo zhongyao zazhi = China journal of Chinese materia medica
[Mechanism and material basis of Sparganii Rhizoma and vinegar-processed Sparganii Rhizoma in treatment of hyperlipidemia based on network pharmacology].
Article
作者: Su, Lian-Lin ; Lu, Tu-Lin ; Li, Lin ; Liu, Huan-Huan ; Yu, Yin-Ping ; Wang, Min ; Ji, De ; Zhang, Ting
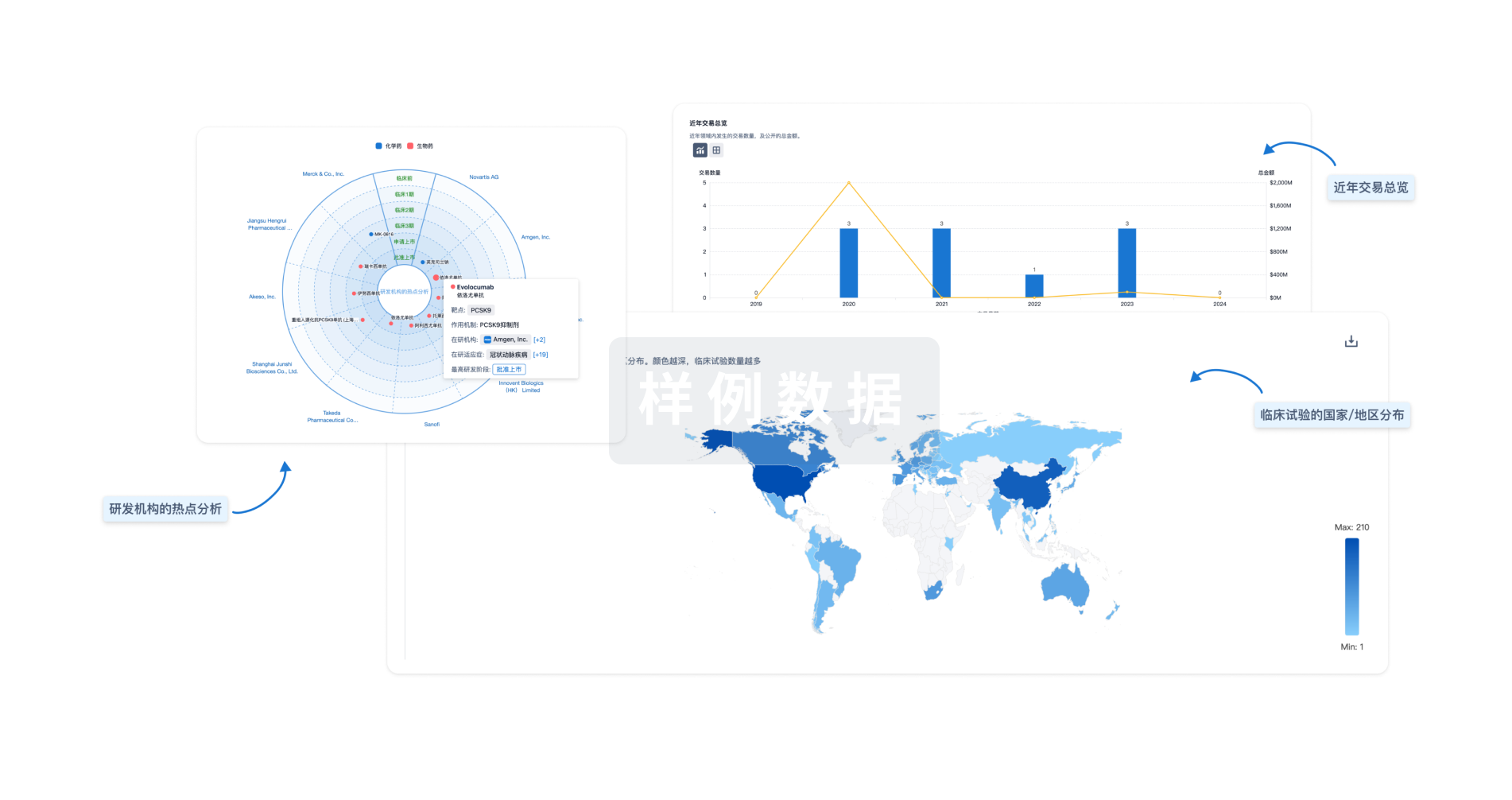
分析
对领域进行一次全面的分析。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用