预约演示
更新于:2025-05-07
Polychondritis, Relapsing
复发性多软骨炎
更新于:2025-05-07
基本信息
别名 Atrophic Polychondritides, Chronic、Atrophic Polychondritis, Chronic、CHONDROMALACIA, SYSTEMIC + [52] |
简介 An acquired disease of unknown etiology, chronic course, and tendency to recur. It is characterized by inflammation and degeneration of cartilage and can result in deformities such as floppy ear and saddle nose. Loss of cartilage in the respiratory tract can lead to respiratory obstruction. |
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

NCT06941376
Pragmatic, Open-Label, Two-Stage, Pilot Study of Effectiveness of Immunomodulatory Medications for Patients With Relapsing Polychondritis
NCT06873100
Efficacy, Safety and Immunological Evaluation of Upadacitinib for Relapsing Polychondritis
NCT06561568
Additional Effects of Kinesio Taping on Knee Joint Proprioception and Spatiotemporal Gait Parameters in Patient With Chrondromalacia Patellae

100 项与 复发性多软骨炎 相关的临床结果
登录后查看更多信息
100 项与 复发性多软骨炎 相关的转化医学
登录后查看更多信息
登录后查看更多信息
2025-03-24Cureus
Early Diagnosis of Relapsing Polychondritis With Airway Involvement: A Case Report
Article
作者: Shundo, Yuki ; Himuro, Naoko ; Hamada, Naoki ; Fujita, Masaki ; Kushima, Natsumi ; Yanagihara, Toyoshi
2025-03-01La Revue de Médecine Interne
Syndromes auto-inflammatoires VEXAS-like : à propos de 2 cas
Article
作者: Masson, Helene ; Hirsch, Pierre ; Chretiennot, Andrea ; Mekinian, Arsene ; Devaux, Mathilde ; Jachiet, Vincent ; Salmeron, Geraldine ; Georgin-Lavialle, Sophie ; Sep-Hieng, Sonnthida ; Le Lostec, Zoe ; Veyssier-Belot, Catherine ; Ghit, Lilia ; Flandrin-Gresta, Pascale
2025-02-16Cureus
Sclerokeratitis and Secondary Glaucoma in Relapsing Polychondritis in a 30-Year-Old Asian Male Patient: A Case Report
Article
作者: Flores, Lovely Keziah C ; Siazon, Richmond R
2025-02-21
2024-02-22
·药智网
免疫疗法抗体药物偶联物细胞疗法上市批准
分析
对领域进行一次全面的分析。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
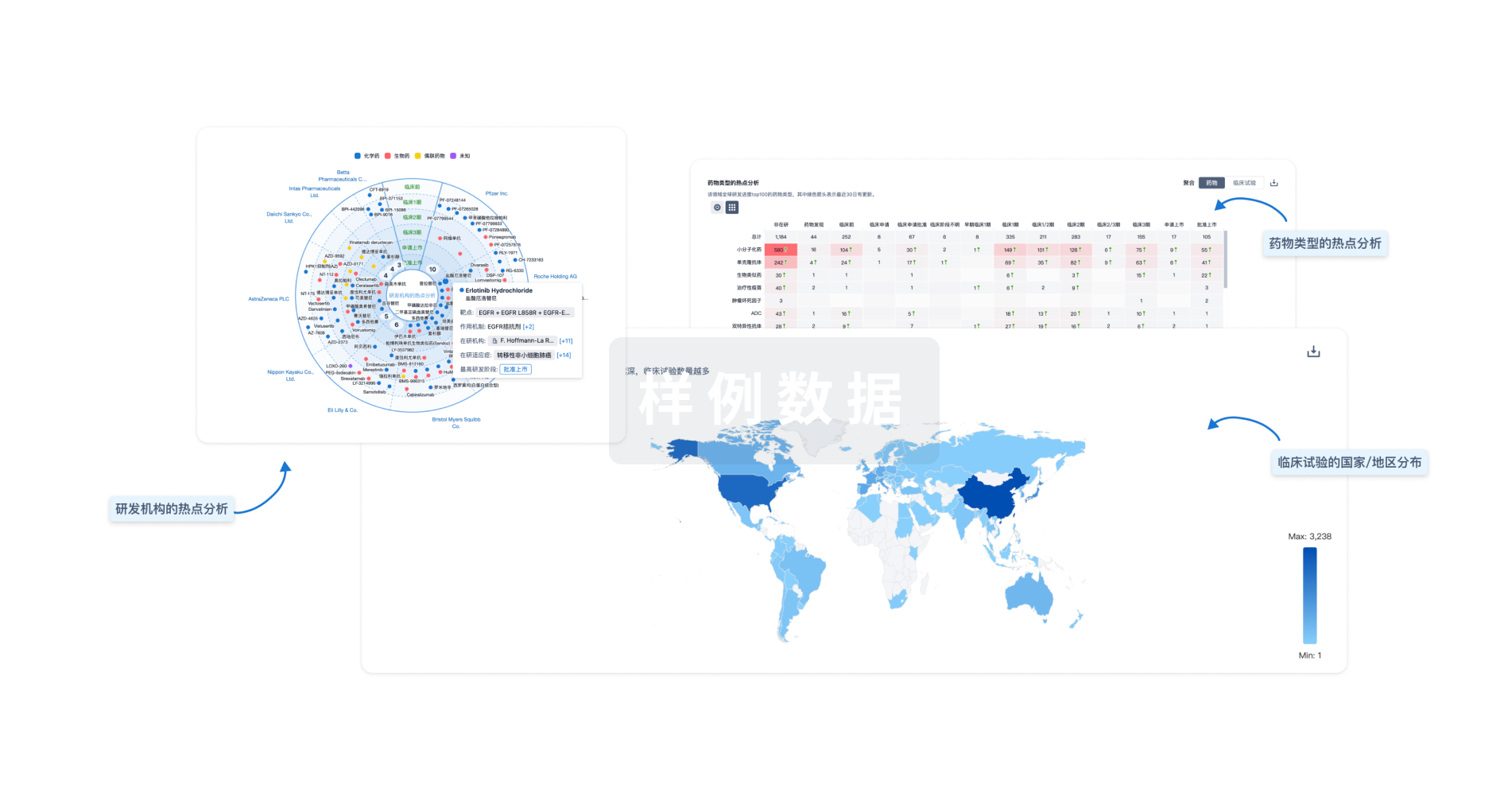
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用