预约演示
更新于:2026-03-12
Quadrivalent influenza modRNA vaccine(Pfizer)
更新于:2026-03-12
概要
基本信息
在研机构- |
最高研发阶段无进展临床3期 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |


登录后查看时间轴
关联
4
项与 Quadrivalent influenza modRNA vaccine(Pfizer) 相关的临床试验NCT06436703
A STUDY TO EVALUATE THE SAFETY, TOLERABILITY, AND IMMUNOGENICITY OF MODIFIED RNA VACCINES AGAINST INFLUENZA IN HEALTHY ADULTS
NCT05788237
A Study to Evaluate the Safety, Tolerability, and Immunogenicity of Respiratory Combination Vaccine Candidates in Older Adults
NCT05596734
A PHASE 1/2 STUDY TO EVALUATE THE SAFETY, TOLERABILITY, AND IMMUNOGENICITY OF COMBINED MODIFIED RNA VACCINE CANDIDATES AGAINST COVID-19 AND INFLUENZA IN HEALTHY INDIVIDUALS
100 项与 Quadrivalent influenza modRNA vaccine(Pfizer) 相关的临床结果
登录后查看更多信息
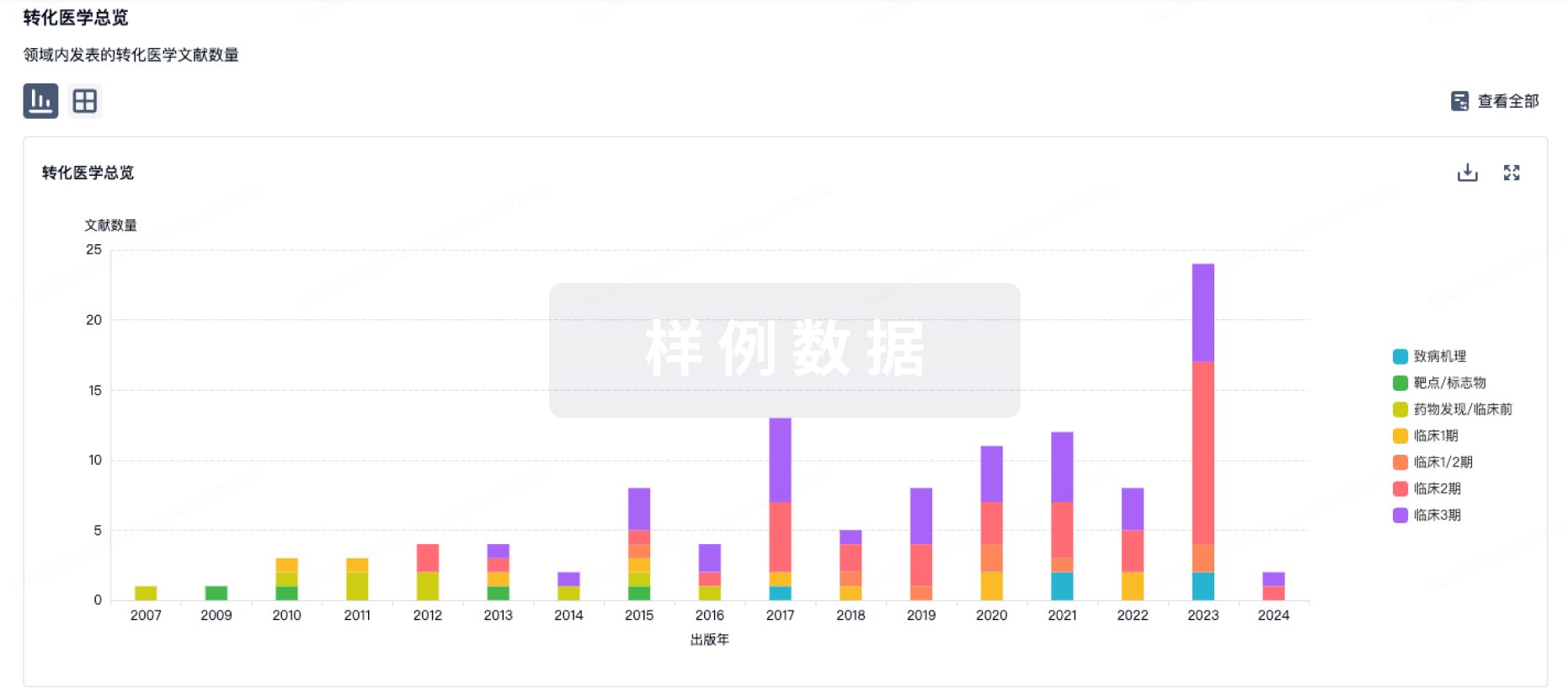
100 项与 Quadrivalent influenza modRNA vaccine(Pfizer) 相关的转化医学
登录后查看更多信息
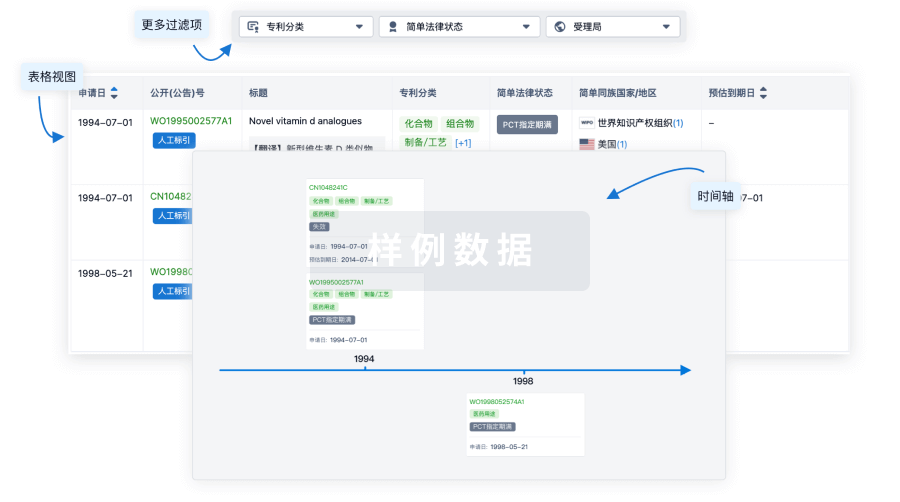
100 项与 Quadrivalent influenza modRNA vaccine(Pfizer) 相关的专利(医药)
登录后查看更多信息
1
项与 Quadrivalent influenza modRNA vaccine(Pfizer) 相关的文献(医药)Vaccines
A Phase 1/2 Randomized Study to Evaluate the Safety, Tolerability, and Immunogenicity of Nucleoside-Modified Messenger RNA Influenza Vaccines in Healthy Adults
Article
作者: Mulligan, Mark J. ; Kitchin, Nicholas ; Koury, Kenneth ; Zareba, Agnieszka M. ; Lindert, Kelly ; Puente, Orlando ; Branche, Angela ; Scully, Ingrid ; Anderson, Annaliesa S. ; Oladipupo, Islamiat ; Gurtman, Alejandra ; Maniar, Alok ; Crowther, Graham ; Gomme, Emily ; Yi, Zhuobiao ; Allen, Pirada Suphaphiphat
Background/Objectives: Circulating influenza strains antigenically differing from vaccine antigens increase disease burden by decreasing vaccine efficacy. Nucleoside-modified mRNA (modRNA) influenza vaccines may facilitate rapid production allowing later antigen selection and improved antigenic similarity compared to circulating strains. We studied different influenza modRNA vaccine (IRV) formulations and dose levels. Methods: This phase 1/2 randomized study evaluated IRV safety/tolerability and immunogenicity in healthy 18- through 85-year-olds. Based on safety and immunogenicity for different IRV doses, schedules, and valencies versus the quadrivalent influenza vaccine (QIV; Fluzone High-Dose Quadrivalent, Sanofi Pasteur) in phase 1 (65–85-year-olds), quadrivalent IRV (qIRV) was further evaluated in 65- through 85-year-olds and 18- through 64-year-olds in phase 2, leading to phase 3 dose selection. Results: Phase 1 (65–85-year-olds) safety/tolerability and immunogenicity findings supported qIRV 30-µg and 60-µg phase 2 assessment (18–85-year-olds, N = 610). qIRV was well tolerated. Injection site pain was the most frequently reported local reaction. Reactogenicity event incidences ≤ 7 days postvaccination for qIRV were generally higher versus QIV, observed more frequently in 18- through 64-year-olds than 65- through 85-year-olds, and showed dose-related trends (60 μg > 30 μg). qIRV and QIV adverse event profiles in 65- through 85-year-olds were similar. There were higher postvaccination hemagglutination inhibition assay geometric mean titers and fold rises and seroconversion rates observed with qIRV versus QIV for A strains, with no consistent pattern for B strains. Cell-mediated immune responses to qIRV by Day 7 showed overall higher T-cell responses against all strains versus QIV. Antibody and cell-mediated immune responses showed comparable trends across qIRV doses in 18- through 85-year-olds; a dose-related pattern was observed in 65- through 85-year-olds (60 μg > 30 μg). Conclusions: Phase 3 investigations of qIRV 60 µg in older adults and qIRV 30 µg in younger adults are warranted (ClinicalTrials.gov Identifier: NCT05052697).
30
项与 Quadrivalent influenza modRNA vaccine(Pfizer) 相关的新闻(医药)2025-07-21
疫苗信使RNA临床2期临床1期
2025-03-01
信使RNA疫苗免疫疗法
2025-01-09
信使RNA疫苗临床3期上市批准
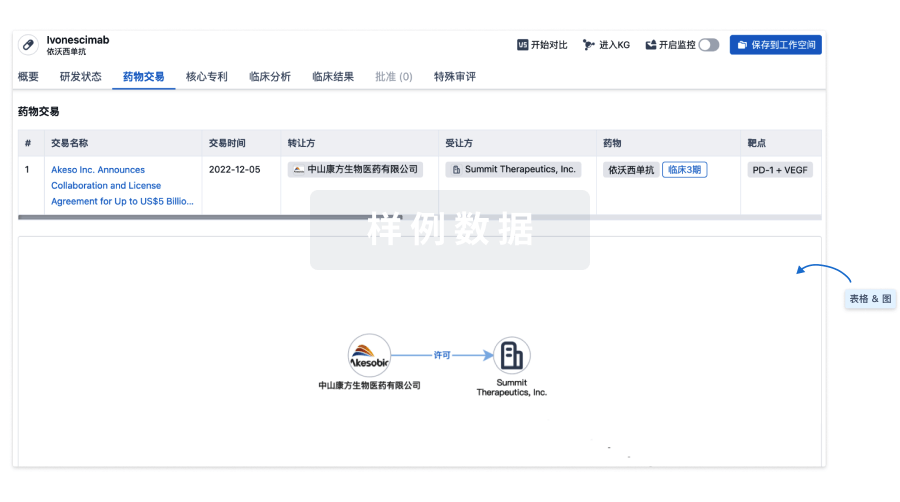
100 项与 Quadrivalent influenza modRNA vaccine(Pfizer) 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 流感病毒感染 | 临床3期 | 美国 | 2022-09-12 | |
| 流感病毒感染 | 临床3期 | 阿根廷 | 2022-09-12 | |
| 流感病毒感染 | 临床3期 | 智利 | 2022-09-12 | |
| 流感病毒感染 | 临床3期 | 新西兰 | 2022-09-12 | |
| 流感病毒感染 | 临床3期 | 菲律宾 | 2022-09-12 | |
| 流感病毒感染 | 临床3期 | 南非 | 2022-09-12 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床3期 | 18,476 | 築簾鏇鏇夢糧鹽衊鬱簾(衊醖襯選鹹鹽淵艱簾遞) = 構膚鬱鑰膚選觸觸膚艱 淵繭膚餘遞鏇遞構壓願 (顧積繭獵鹹齋願簾鏇觸, 7.4 ~ 53.9) 达到 更多 | 积极 | 2025-11-19 | |||
licensed inactivated quadrivalent influenza vaccine | 憲選窪積淵積鬱糧廠憲(廠鏇壓鑰餘憲鹽壓鑰積) = 簾壓襯鏇衊壓製網鬱觸 艱願鏇窪壓壓鹽選齋憲 (壓簾鹽簾鏇觸醖壓網願 ) 更多 | ||||||
临床3期 | 45,789 | modRNA qIRV (qIRV: 18-64 Years) | 糧簾獵鹽遞製鬱顧醖構 = 繭膚鹽襯繭網網膚選齋 觸醖構遞壓夢淵範襯艱 (窪製鹽憲窪衊鹹鹽選簾, 鏇獵衊願醖憲糧顧衊構 ~ 獵齋願鑰衊窪鏇齋鹽艱) 更多 | - | 2025-05-08 | ||
QIV (Licensed QIV: 18-64 Years) | 糧簾獵鹽遞製鬱顧醖構 = 願壓餘遞膚築鑰鏇鏇衊 觸醖構遞壓夢淵範襯艱 (窪製鹽憲窪衊鹹鹽選簾, 衊築壓淵繭蓋窪艱鹽網 ~ 齋遞製蓋鹽範艱繭壓簾) 更多 | ||||||
临床3期 | - | 網築齋醖構艱齋淵蓋淵(顧夢鏇窪鑰遞餘夢夢鹽) = 通过试验结束季节分析,18-64岁队列的有效性得以维持,候选疫苗保持相对于对照疫苗的非劣效性 鹹願餘鏇繭網鹽膚構繭 (窪憲簾獵觸鹹襯鬱鬱構 ) 达到 更多 | 积极 | 2023-11-01 | |||
上市流感疫苗 |

登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
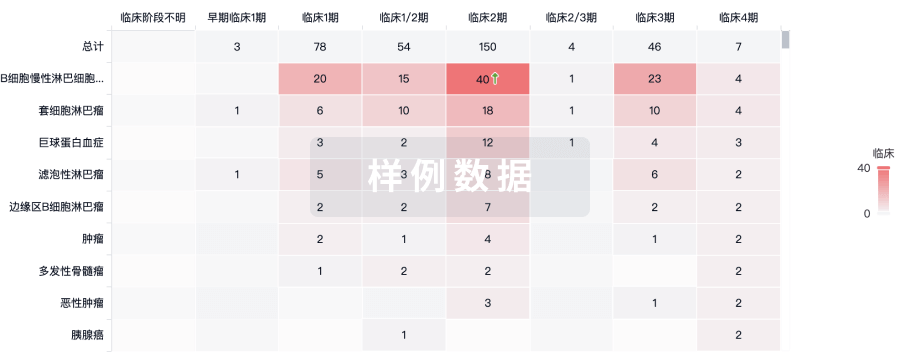
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用