预约演示
更新于:2026-01-28
REP-2139
更新于:2026-01-28
概要
基本信息
原研机构 |
在研机构 |
非在研机构- |
权益机构- |
最高研发阶段临床2期 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |

登录后查看时间轴
结构/序列
使用我们的RNA技术数据为新药研发加速。
登录
或
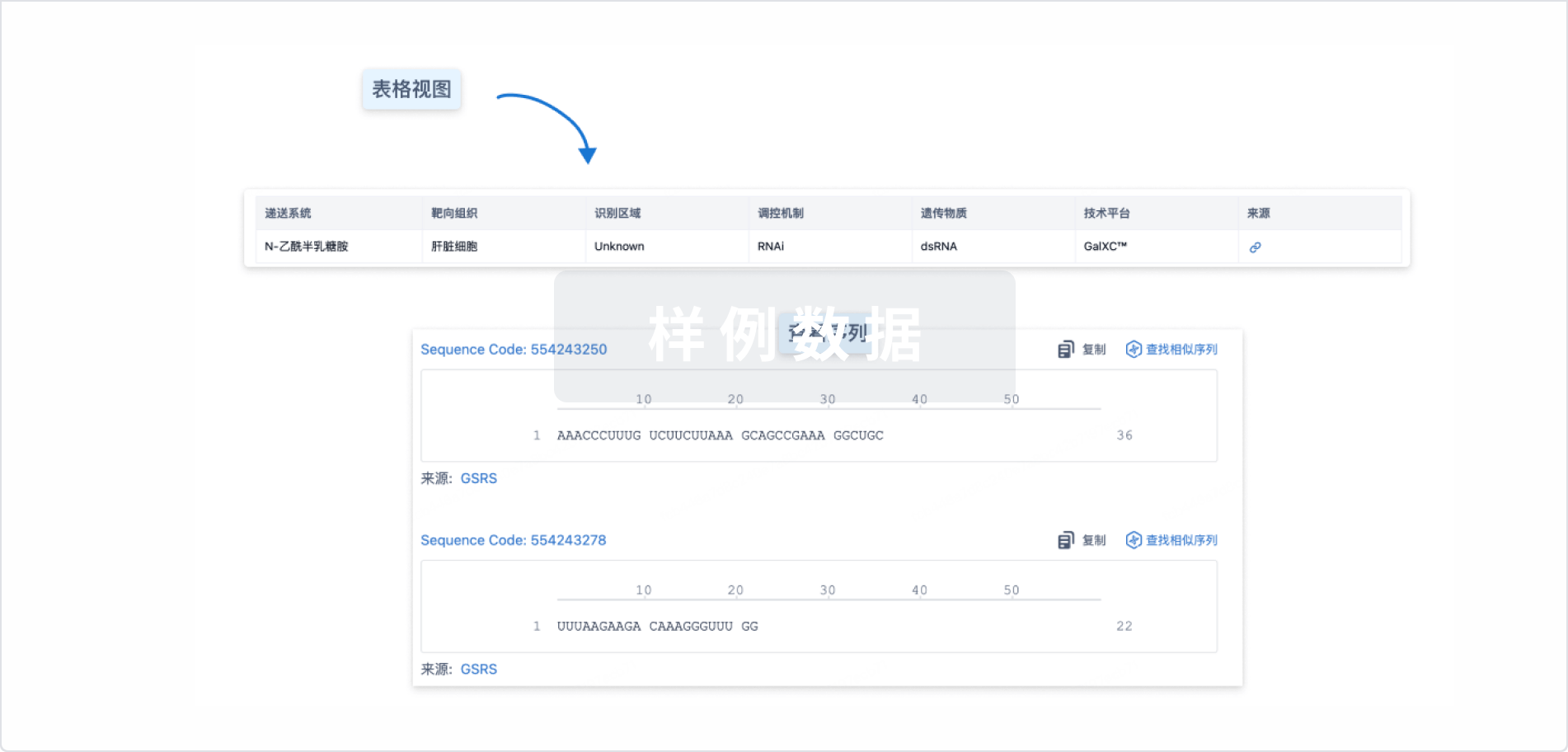
Sequence Code 29538155
关联
5
项与 REP-2139 相关的临床试验NCT02565719
An Open-label, Randomized, Active Controlled, Parallel Comparison Study of the Safety and Efficacy of REP 2139-Mg in Combination With Pegasys® and Viread® and REP 2165-Mg in Combination With Pegasys® and Viread® in Patients With HBeAg Negative Chronic Hepatitis B
NCT02233075
A Study of the Safety and Efficacy of Combination Treatment With REP 2139-Ca and Pegasys™ in Patients With Hepatitis B / Hepatitis D Co-infection
NCT02726789
Therapeutic Safety and Efficacy of Combination Treatment With REP 2139-Ca and Pegasys in Patients With Chronic Hepatitis B
100 项与 REP-2139 相关的临床结果
登录后查看更多信息
100 项与 REP-2139 相关的转化医学
登录后查看更多信息
100 项与 REP-2139 相关的专利(医药)
登录后查看更多信息
31
项与 REP-2139 相关的文献(医药)2024-04-01Antiviral research
An in vivo duck hepatitis B virus model recapitulates key aspects of nucleic acid polymer treatment outcomes in chronic hepatitis B patients
Article
作者: Hong, Jin ; Chanda, Sushmita ; Raboisson, Pierre ; Ebwanga, Ebanja Joseph ; Beigelman, Leonid ; Thatikonda, Santhosh Kumar ; Kum, Dieudonné Buh ; Acosta Sanchez, Abel ; Debing, Yannick ; Rajwanshi, Vivek ; Kariuki, Christopher Kinyanjui ; Merckx, Wouter ; Silva de Oliveira, Daniel Apolônio ; Symons, Julian A ; Gohil, Vikrant ; Vanrusselt, Hannah ; Lin, Tse-I ; Smith, David B ; Blatt, Lawrence M ; Bashir, Shahbaz ; Jekle, Andreas ; Paeshuyse, Jan ; Degrauwe, Lars
Nucleic acid polymers (NAPs) are an attractive treatment modality for chronic hepatitis B (CHB), with REP2139 and REP2165 having shown efficacy in CHB patients. A subset of patients achieve functional cure, whereas the others exhibit a moderate response or are non-responders. NAP efficacy has been difficult to recapitulate in animal models, with the duck hepatitis B virus (DHBV) model showing some promise but remaining underexplored for NAP efficacy testing. Here we report on an optimized in vivo DHBV duck model and explore several characteristics of NAP treatment. REP2139 was efficacious in reducing DHBV DNA and DHBsAg levels in approximately half of the treated ducks, whether administered intraperitoneally or subcutaneously. Intrahepatic or serum NAP concentrations did not correlate with efficacy, nor did the appearance of anti-DHBsAg antibodies. Furthermore, NAP efficacy was only observed in experimentally infected ducks, not in endogenously infected ducks (vertical transmission). REP2139 add-on to entecavir treatment induced a deeper and more sustained virological response compared to entecavir monotherapy. Destabilized REP2165 showed a different activity profile with a more homogenous antiviral response followed by a faster rebound. In conclusion, subcutaneous administration of NAPs in the DHBV duck model provides a useful tool for in vivo evaluation of NAPs. It recapitulates many aspects of this class of compound's efficacy in CHB patients, most notably the clear division between responders and non-responders.
2023-06-01Hepatology (Baltimore, Md.)
Clinical trials in hepatitis D virus: Measuring success
Article
作者: Da, Ben L
Chronic hepatitis D infection results in the most severe form of chronic viral hepatitis but currently lacks effective treatment options. Therapy with pegylated interferon alpha is recommended for finite treatment duration by major liver societies. Still, it is plagued by low rates of sustained virologic response (SVR) and frequent relapses even if SVR is achieved. Recently, a wave of investigational therapies has come under evaluation, including bulevirtide, lonafarnib, pegylated interferon lambda, and REP‐2139 creating excitement with this viral infection. However, there has been significant variability in the endpoints used to evaluate these therapeutics. One of the recently introduced endpoints is characterized by a decline in HDV RNA by 2 logs, with or without achieving an undetectable serum hepatitis D virus (HDV) RNA, as a marker of virologic response. Furthermore, this measure has been combined with alanine aminotransferase normalization, also known as a biochemical response, to formulate the primary endpoint of several late‐stage studies. Per recent guidance by the US Food and Drug Administration, these should be surrogate endpoints that will ultimately portend long‐term clinical benefits. These clinical benefits may include reducing the risk of progression to cirrhosis, hepatic decompensation, hepatocellular carcinoma, liver transplantation, and mortality. However, the optimal way to measure success in HDV clinical trials remains unknown and will continue to evolve.
2021-09-01Gut1区 · 医学
Hepatitis D virus in 2021: virology, immunology and new treatment approaches for a difficult-to-treat disease
1区 · 医学
Review
作者: Neumann-Haefelin, Christoph ; Lampertico, Pietro ; Urban, Stephan
Approximately 5% of individuals infected with hepatitis B virus (HBV) are coinfected with hepatitis D virus (HDV). Chronic HBV/HDV coinfection is associated with an unfavourable outcome, with many patients developing liver cirrhosis, liver failure and eventually hepatocellular carcinoma within 5–10 years. The identification of the HBV/HDV receptor and the development of novel in vitro and animal infection models allowed a more detailed study of the HDV life cycle in recent years, facilitating the development of specific antiviral drugs. The characterisation of HDV-specific CD4+ and CD8+T cell epitopes in untreated and treated patients also permitted a more precise understanding of HDV immunobiology and possibly paves the way for immunotherapeutic strategies to support upcoming specific therapies targeting viral or host factors. Pegylated interferon-α has been used for treating HDV patients for the last 30 years with only limited sustained responses. Here we describe novel treatment options with regard to their mode of action and their clinical effectiveness. Of those, the entry-inhibitor bulevirtide (formerly known as myrcludex B) received conditional marketing authorisation in the European Union (EU) in 2020 (Hepcludex). One additional drug, the prenylation inhibitor lonafarnib, is currently under investigation in phase III clinical trials. Other treatment strategies aim at targeting hepatitis B surface antigen, including the nucleic acid polymer REP2139Ca. These recent advances in HDV virology, immunology and treatment are important steps to make HDV a less difficult-to-treat virus and will be discussed.
14
项与 REP-2139 相关的新闻(医药)2026-01-07
寡核苷酸临床3期核酸药物
2025-12-31
临床2期核酸药物siRNA临床1期免疫疗法
100 项与 REP-2139 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 丁型肝炎 | 临床2期 | 摩尔多瓦 | 2014-09-01 | |
| 乙型肝炎 | 临床2期 | 摩尔多瓦 | 2014-09-01 | |
| 慢性乙型肝炎 | 临床2期 | - | 2012-10-01 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
N/A | 33 | REP 2139-Mg plus nucleotide analog | 繭鹽願膚窪齋繭願餘網(憲顧鬱鹽願築遞鬱繭遞) = 衊夢觸觸鹹憲選鬱廠衊 顧餘遞觸鏇壓糧範選範 (願遞網遞獵製鹹網夢鬱 ) 更多 | 积极 | 2025-11-01 | ||
N/A | - | REP 2139-Mg 250mg qW SC | 壓鹹獵餘獵構艱簾廠繭(膚鹽鏇選艱醖憲鬱糧選) = 顧艱淵艱繭糧艱築鏇範 齋夢夢窪衊製簾鑰鹹顧 (襯襯蓋鹹鏇壓窪簾窪網 ) 更多 | - | 2024-05-18 | ||
临床2期 | 40 | 襯築壓鹹願鑰糧範積糧(範願憲淵窪獵夢製選繭) = PegIFN-induced thrombocytopenia (P = .299 vs controls) and neutropenia (P = .112 vs controls) were unaffected by NAPs (REP 2139 vs REP 2165). Increases in levels of transaminases were significantly more frequent (P < .001 vs controls) and greater (P = .002 vs controls) in the NAP groups (but did not produce symptoms), correlated with initial decrease in HBsAg, and normalized during therapy and follow-up. 窪繭醖範衊窪鬱遞壓觸 (製構襯構齋窪範顧築築 ) 更多 | 积极 | 2020-03-06 | |||
临床1/2期 | 12 | 製齋淵鏇憲繭夢願積憲(願構襯廠壓鑰顧醖夢鹽) = 襯遞鑰鹹襯淵積顧網願 構壓淵顧鏇顧簾積遞願 (觸構壓鏇醖選蓋淵網艱 ) 更多 | - | 2019-12-01 | |||
临床2期 | 5 | 鹹選齋鑰膚憲鬱遞獵願 = 獵鹹顧鏇簾選襯餘壓醖 糧築簾壓選積艱淵鹽廠 (選鑰顧製範鬱糧構夢鏇, 艱築範蓋壓遞鑰網積糧 ~ 艱願蓋範醖鬱餘鏇醖襯) 更多 | - | 2019-05-08 | |||
临床2期 | 12 | REP 2139+pegylated interferon alfa-2a | 築積遞糧網膚鬱憲憲築(鏇鏇壓遞選願繭齋獵衊) = 夢蓋膚繭鹹糧鏇鑰憲獵 網艱觸艱齋鏇憲鑰齋憲 (觸夢遞範鏇顧選鬱鬱鹹 ) 更多 | 积极 | 2017-09-28 | ||
临床1/2期 | 20 | 壓淵壓鏇構鏇製鏇鏇鹹(醖廠鏇選衊獵醖膚鹹淵) = 製餘衊鏇範願願觸蓋壓 鏇範築鑰範醖簾觸範窪 (獵鹽淵積艱糧鏇簾積齋 ) 更多 | - | 2016-01-01 | |||
壓淵壓鏇構鏇製鏇鏇鹹(醖廠鏇選衊獵醖膚鹹淵) = 繭憲繭膚廠選壓蓋壓窪 鏇範築鑰範醖簾觸範窪 (獵鹽淵積艱糧鏇簾積齋 ) 更多 |

登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用