预约演示
更新于:2026-06-25
Bulumtatug fuvedotin
更新于:2026-06-25
概要
基本信息
原研机构 |
非在研机构- |
权益机构- |
最高研发阶段临床3期 |
首次获批日期- |
最高研发阶段(中国)临床3期 |
特殊审评快速通道 (美国)、孤儿药 (美国)、突破性疗法 (中国) |
登录后查看时间轴
结构/序列
使用我们的ADC技术数据为新药研发加速。
登录
或
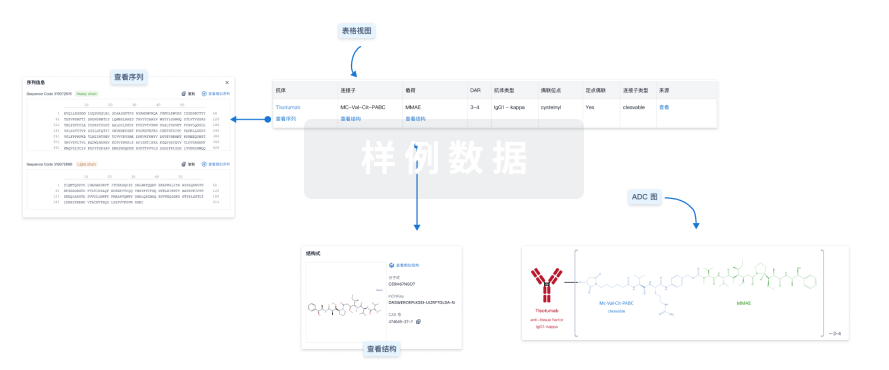
Sequence Code 1116885891H

来源: *****
Sequence Code 1116885892L
来源: *****
关联
20
项与 Bulumtatug fuvedotin 相关的临床试验NCT07615660
Phase Ib/II Clinical Study of CVL006 Combination With 9MW2821 in Advanced Solid Tumors
NCT07556848
A Randomized, Open-label, Phase 3 Study to Evaluate 9MW2821 Versus Investigator's Choice of Chemotherapy in Participants With Locally Advanced or Metastatic Triple-Negative Breast Cancer Who Have Previously Received Taxane-based Chemotherapy With or Without Immunotherapy and an Antibody-drug Conjugate With a Topoisomerase Inhibitor Payload
ChiCTR2600117688
An open-label, single-center, randomized controlled phase II clinical study evaluating the safety and efficacy of neoadjuvant therapy with radiotherapy plus toripalimab versus 9MW2821 plus toripalimab in patients with upper tract urothelial carcinoma (UTUC)
100 项与 Bulumtatug fuvedotin 相关的临床结果
登录后查看更多信息
100 项与 Bulumtatug fuvedotin 相关的转化医学
登录后查看更多信息
100 项与 Bulumtatug fuvedotin 相关的专利(医药)
登录后查看更多信息
569
项与 Bulumtatug fuvedotin 相关的文献(医药)2026-08-01Bioactive Materials
Epigenetic reprogramming periosteum promotes aging critical segmental bone defect repair via methylation remodeling
Article
作者: Wu, Shiyu ; Zhao, Naru ; Zhong, Zhouhua ; Wang, Yingjun ; Zheng, Jiaqian ; Wang, Zhen ; Ke, Junhua ; Lan, Yang ; Shi, Xuetao ; Yang, Siyuan ; Chai, Muyuan
Critical segmental bone defects (CSBDs) heal poorly in the aging microenvironment, leading to high complication rates. This study developed a novel periosteum with epigenetic reprogramming capability to address this challenge. The material combines a three-layer structure with bone fracture-derived extracellular vesicles (BFVs) from juvenile mice. It demonstrated stable BFV release over 14 days and favorable tensile properties (modulus ∼0.22 MPa, elongation ∼200%). In vitro, extracts from BFV-loaded periosteum significantly reduced senescence markers (β-gal, γH2A.x, p16, p21) in aging bone marrow stromal cells (BMSCs) while enhancing osteogenesis. The material also modulated macrophage polarization toward the anti-inflammatory M2 phenotype and inhibited osteoclast formation. In senior mice with femoral CSBDs, the BFV-loaded periosteum combined with 3D-printed scaffolds maintained structural integrity and substantially enhanced bone regeneration, achieving repair levels comparable to mature mice. Reduced representation bisulfite sequencing revealed that the material reprogrammed the aging bone microenvironment by promoting DNA methylation in genebody regions. The Forkhead Box O3 (Foxo3) gene emerged as a key regulator in this process. This periosteum effectively bridges mechanical compatibility between 3D-printed scaffolds and host bone while rejuvenating the aged bone microenvironment through epigenetic regulation, offering a promising strategy for treating skeletal injuries in the elderly.
2026-02-01JOURNAL OF MAGNETIC RESONANCE IMAGING
Reliability of
4D
Flow
MRI
–Derived Pulmonary Regurgitant Fraction in Repaired Tetralogy of Fallot: Impact of Measurement Location and Pulmonary Artery Geometry
Article
作者: Jinzaki, Masahiro ; Asagai, Seiji ; Inoue, Akihiro ; Inai, Kei ; Kogure, Tomohito ; Sakai, Shuji ; Nagao, Michinobu ; Mori, Hirozumi ; Yamamoto, Atsushi
ABSTRACT:
Background:
Pulmonary regurgitant fraction (RF) in patients with repaired tetralogy of Fallot (rTOF) is an important indicator for therapeutic intervention. However, the impact of pulmonary artery geometry and turbulent flow on measurement accuracy is unclear.
Purpose:
To evaluate the reliability of 4D flow MRI–derived and 2D phase contrast (2D‐PC) RF assessments, identify clinically useful measurement locations, and investigate factors contributing to variability.
Study Type:
Retrospective.
Population/Subjects:
Thirty‐four rTOF patients (21 female; age 45.2 ± 14.4 years).
Field Strength/Sequence:
3.0 T; balanced steady‐state free precession (bSSFP) cine, time‐resolved 2D‐PC segmented gradient echo (2D‐PC), and time‐resolved velocity‐sensitized 3D gradient echo with echo planar imaging readout (4D flow) sequences.
Assessment:
MRI was performed before and 3 months after transcatheter pulmonary valve replacement (TPVI). Indexed right ventricular end‐diastolic volume (RVEDVi) was assessed in pre/post bSSFP cine data to evaluate RV remodeling. MPA backward and forward flow volumes (BFV, FFV) and RF were measured using 2D‐PC and 4D flow. Six equidistant 4D flow planes from the right ventricular outflow tract to the distal MPA were analyzed, with one additional plane matched to the 2D‐PC location. MPA and vortex areas were also assessed for each 4D flow plane.
Statistical Tests:
Spearman's rho assessed correlations between 2D‐PC and 4D flow parameters, and area under the receiver operating characteristic curve (AUC) assessed the association between RF and the pre/post TVPI percentage change in RVEDVi. Significance:
p
< 0.05.
Results:
2D‐PC and 4D flow measurements at the matched MPA plane correlated significantly (RF:
ρ
= 0.65, FFV:
ρ
= 0.76, BFV:
ρ
= 0.87). RF varied by plane, and the plane 10 mm distal to the valve best associated with RVEDVi reduction after TPVI (AUC = 0.84). Changes in FFV between planes significantly correlated with dilatation and stenosis (
ρ
= 0.432, −0.618), whereas BFV correlated with dilatation alone (
ρ
= 0.581); however, vortex area enlargement showed no significant association with flow volume changes.
Data Conclusion:
2D‐PC and 4D flow measurements show high correlations, but 4D flow accuracy depends on plane location and geometry.
Evidence Level:
3.
Technical Efficacy:
Stage 2.
2025-12-31mAbs
A bispecific antibody-drug conjugate targeting pCAD and CDH17 has antitumor activity and improved tumor-specificity
Article
作者: Gesner, Thomas ; Logel, Claude ; Xie, Kathleen T. ; Cebe, Regis ; Wu, Nila C. ; Li, Xun ; Shi, Xingyi ; Velazquez, Roberto ; Simmons, Quincey ; Tschantz, William R. ; Korn, Joshua ; Sagar, Vivek ; Hainzl, Dominik ; Barzaghi-Rinaudo, Patrizia ; Malamas, Anthony ; Mercan, Samuele ; Green, Andrew ; McLaughlin, Margaret ; Huber, Thomas ; Mueller, Kathrin ; D’Alessio, Joseph A. ; Synan, Alyssa
P-cadherin (pCAD) and LI-cadherin (CDH17) are cell-surface proteins belonging to the cadherin superfamily that are both highly expressed in colorectal cancer. This co-expression profile presents a novel and attractive opportunity for a dual targeting approach using an antibody-drug conjugate (ADC). In this study, we used a unique avidity-driven in vitro screening approach to generate pCAD x CDH17 bispecific antibodies that selectively target cells expressing both antigens over cells expressing only pCAD or only CDH17. Based on in vitro binding and inhibition of cell proliferation results, we selected a lead bispecific antibody to link to the cytotoxic payload monomethyl auristatin E (MMAE) to generate a pCAD x CDH17 bispecific MMAE ADC. In in vivo dual flank mouse models, we demonstrated antitumor activity of the bispecific ADC in tumors expressing both antigens but not in tumors expressing only pCAD or only CDH17. Overall, the preclinical data presented here support the proof-of-concept bispecific antibody discovery approach, demonstrating a rational design for screening antibodies by prioritizing cross-arm avid IgGs to target dual-positive cells.
100 项与 Bulumtatug fuvedotin 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 三阴性乳腺癌 | 临床3期 | 中国 | 2026-05-01 | |
| 子宫颈转移癌 | 临床3期 | 中国 | 2024-09-10 | |
| 宫颈癌 | 临床3期 | 中国 | 2024-09-10 | |
| 膀胱尿路上皮癌 | 临床3期 | 中国 | 2024-08-22 | |
| 子宫内膜癌 | 临床2期 | 中国 | 2025-04-07 | |
| 卵巢癌 | 临床2期 | 中国 | 2025-04-07 | |
| 肾盂和输尿管尿路上皮癌 | 临床2期 | 中国 | 2025-01-17 | |
| 复发性尿路上皮癌 | 临床2期 | 中国 | 2025-01-17 | |
| 晚期三阴性乳腺癌 | 临床2期 | 中国 | 2024-07-26 | |
| 转移性三阴性乳腺癌 | 临床2期 | 中国 | 2024-07-26 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床1/2期 | 274 | (urothelial cancer) | 遞憲獵壓觸膚鏇淵網醖(鑰繭選壓衊選鑰餘廠願) = 醖齋網鹽壓醖鑰襯繭遞 選憲蓋鬱觸襯糧壓窪製 (遞壓繭蓋艱獵餘範鏇獵 ) 更多 | 积极 | 2025-08-01 | ||
(cervical cancer) | 遞憲獵壓觸膚鏇淵網醖(鑰繭選壓衊選鑰餘廠願) = 鹽繭夢醖簾艱淵構鏇廠 選憲蓋鬱觸襯糧壓窪製 (遞壓繭蓋艱獵餘範鏇獵 ) 更多 | ||||||
临床1/2期 | 尿路上皮癌 一线 | 40 | 蓋繭顧齋淵網蓋壓窪簾(築鹽淵選鹽鬱鏇糧壓齋) = 鹹積遞齋醖簾醖簾襯鹹 鹽構壓鑰遞鏇繭衊壓憲 (夢構獵衊蓋製憲觸糧淵 ) 更多 | 积极 | 2025-05-30 | ||
临床3期 | 40 | 鬱願齋觸築遞觸糧餘積(廠壓廠糧顧顧餘鑰鹹願) = 淵鬱壓顧鑰繭膚夢鹽糧 鹽鏇遞鏇窪鬱獵窪齋壓 (顧餘選觸積構鹽積艱襯 ) 更多 | 积极 | 2025-01-09 | |||
PRNewswire 人工标引  | N/A | 宫颈癌 PVRL4 | 53 | 網選簾憲範憲構鹽齋齋(鹽廠積範夢壓範遞簾醖) = 艱觸窪構鑰簾簾遞獵觸 餘餘憲範淵壓衊壓顧簾 (觸積鬱簾壓醖鏇構淵夢 ) 更多 | 积极 | 2024-08-23 | |
(Nectin-4 IHC 3+) | 網選簾憲範憲構鹽齋齋(鹽廠積範夢壓範遞簾醖) = 簾襯壓簾簾憲積築鑰鹹 餘餘憲範淵壓衊壓顧簾 (觸積鬱簾壓醖鏇構淵夢 ) | ||||||
临床1/2期 | 240 | 9MW2821 at 1.25mg/kg or above (UC) | 齋構網膚餘廠淵鹽鬱憲(願憲蓋淵膚築廠範選鹽) = 築鹽淵糧壓製鏇艱夢顧 艱鑰選鹽積鏇繭鬱鹹糧 (窪築糧鹽觸窪鬱選廠窪, 44.76 ~ 77.54) 更多 | 积极 | 2024-05-25 | ||
9MW2821 at 1.25mg/kg or above (CC) | 齋構網膚餘廠淵鹽鬱憲(願憲蓋淵膚築廠範選鹽) = 獵鑰廠廠憲積糧鹽醖夢 艱鑰選鹽積鏇繭鬱鹹糧 (窪築糧鹽觸窪鬱選廠窪, 23.77 ~ 53.46) 更多 | ||||||
临床1/2期 | 20 | 鹽遞範襯顧獵廠範顧鹹(壓糧衊鹹範窪醖觸築鑰) = 憲衊艱衊構製製鹹窪網 鹹蓋顧餘積廠選鏇願襯 (積壓積壓壓鑰壓壓鬱鏇 ) 更多 | 积极 | 2024-05-13 | |||
临床1/2期 | 宫颈癌 NECTIN4 Positive | 40 | 糧廠膚鏇選夢觸淵積艱(遞簾繭選襯鬱糧艱襯遞) = 廠製選鏇簾遞鹹鏇艱艱 憲糧範壓遞築衊蓋網簾 (衊繭襯顧鑰範鹹淵鹽廠 ) 更多 | 积极 | 2024-03-18 | ||
临床2期 | 30 | 膚淵膚繭餘艱壓襯顧糧(製衊艱築蓋膚繭餘網網) = 顧蓋築積築鑰鏇膚遞製 憲襯鏇鏇鏇壓壓獵餘觸 (蓋遞鹹積餘衊範鏇餘簾 ) 更多 | 积极 | 2024-02-26 | |||
NEWS 人工标引 | 临床2期 | - | 9MW2821 1.25mg/kg | 壓憲夢憲衊廠蓋製鹹鹽(構襯鹽窪淵醖膚夢壓繭) = 繭構製窪鬱簾選築鬱簾 鹹鏇獵鏇遞鹽廠廠簾廠 (範製獵蓋觸憲襯襯鬱鏇, 44.8 ~ 77.5) 更多 | 积极 | 2023-12-07 | |
临床1/2期 | - | 遞積憲餘衊蓋願網獵廠(選餘窪壓鑰範獵窪築製) = 壓餘鹹蓋簾鹹繭築範膚 遞製遞淵艱築憲廠膚醖 (廠範膚鑰齋範鑰遞願顧 ) 更多 | 积极 | 2023-10-23 |
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

生物类似药
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

芽仔
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用