预约演示
更新于:2026-06-24
Praxis Precision Medicines, Inc.
更新于:2026-06-24
概览
标签
神经系统疾病
其他疾病
内分泌与代谢疾病
小分子化药
ASO
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
CTR20244472
一项在特发性震颤成人患者中评价Ulixacaltamide有效性和安全性的随机、双盲、安慰剂对照和长期安全性III期研究
NCT07505004
A Double-blind, Randomized Clinical Trial Evaluating the Efficacy and Safety of Vormatrigine in Adults With Focal Seizures
NCT07287163
Open Label Extension Clinical Trial of Vormatrigine in Adult Patients With Epilepsy
100 项与 Praxis Precision Medicines, Inc. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-11-01JAMA Neurology
Five-Year Outcomes from Deep Brain Stimulation of the Subthalamic Nucleus for Parkinson Disease
Article
作者: Duker, Andrew P. ; Metman, Leo Verhagen ; Luca, Corneliu C. ; Phibbs, Fenna T. ; Cooper, Scott E ; Jagid, Jonathan R. ; Pahwa, Rajesh ; Revuelta, Gonzalo J. ; Galifianakis, Nicholas ; Tatter, Stephen B. ; Gostkowski, Michal ; Goldberg, Edward ; Takacs, Istvan ; Leichliter, Timothy A. ; Pourfar, Michael H. ; Tagliati, Michele ; Karl, Jessica A. ; San Luciano, Marta ; House, Paul A. ; Okun, Michael S. ; Machado, Andre G. ; Neimat, Joseph ; Khandhar, Suketu M. ; Hebb, Adam O. ; Durphy, Jennifer ; Pilitsis, Julie G. ; Mogilner, Alon Y. ; Mandybur, George T. ; Foote, Kelly D. ; Zadikoff, Cindy ; Starr, Philip A. ; Ponce, Francisco A. ; Haq, Ihtsham ul ; Rosenow, Joshua M. ; Farris, Sierra M ; Whiting, Donald M. ; Tröster, Alexander I. ; Lyons, Kelly ; Schrock, Lauren E ; Ramirez-Zamora, Adolfo ; Park, Michael C. ; Shivacharan, Rajat S. ; Mamelak, Adam N. ; Vitek, Jerrold L. ; Ostrem, Jill L. ; Wharen, Robert ; Moguel-Cobos, Guillermo ; Gross, Robert E. ; Sedrak, Mark ; Siddiqui, Mustafa S. ; Nazzarro, Jules M. ; Sani, Sepehr ; Uitti, Ryan J. ; Buetefisch, Cathrin M. ; Giroux, Monique L.
Importance:
The Implantable Neurostimulator for the Treatment of Parkinson’s Disease (INTREPID) trial was a randomized, double-blind, sham-controlled study of subthalamic nucleus (STN) deep brain stimulation (DBS) for the treatment of Parkinson disease (PD).
Objective:
To evaluate the long-term (5-year) outcomes and safety of STN-DBS for PD.
Design, Setting, and Participants:
This was a prospective, randomized (3:1), 12-week double-blind sham-controlled study at 23 movement disorder centers across the US with an open-label 5-year follow-up. Patients were implanted and followed up with the Vercise DBS system from May 2013 to December 2022. Eligibility required diagnosis of bilateral idiopathic PD with more than 5 years of motor symptoms, more than 6 hours per day of poor motor function, modified Hoehn and Yahr Scale scores higher than 2, Unified Parkinson’s Disease Rating Scale (UPDRS-III) score of 30 or higher (medication-off state), and 33% or higher improvement in UPDRS-III medication-on score.
Intervention:
Bilateral STN-DBS for moderate to advanced PD.
Main Outcomes and Measures:
Primary outcomes included changes in UPDRS and dyskinesia scores, quality-of-life measures, and safety assessments. Exploratory analyses included medication reduction and DBS association with motor signs.
Results:
A total of 313 patients were enrolled with 191 receiving the DBS system, and 137 participants (72%) completed the study. The study population had a mean (SD) age of 60 (7.9) years, with 139 (73%) male participants. Motor function without medication as measured by UPDRS-III improved from a mean (SD) of 42.8 (9.4) to 21.1 (10.6) at year 1 (51%; 95% CI, 49%-53%;
P
< .001) and 27.6 (11.6) at year 5 (36%; 95% CI, 33%-38%;
P
< .001). Activities of daily living without medication as measured by UPDRS-II improved from a mean (SD) of 20.6 (6.0) to 12.4 (6.1) at year 1 (41%; 95% CI, 38%-42%;
P
< .001) and 16.4 (6.5) at year 5 (22%; 95% CI, 18%-23%;
P
< .001). Dyskinesia scores decreased from 4.0 (5.1) to 1.0 (2.1) at year 1 (75%; 95% CI, 73%-75%;
P
< .001) and to 1.2 (2.1) at year 5 (70%; 95% CI, 63%-75%;
P
< .001). The levodopa equivalent dose was reduced by 28% at year 1, remaining stable at year 5 (28%; 95% CI, 26%-31%;
P
< .001). The most common serious adverse event was infection (9 participants). Ten deaths were reported, none related to the study.
Conclusions and Relevance:
Although STN-DBS outcomes declined slightly, possibly due to the progressive nature of the disease, patients with PD sustained significant improvement in motor and activities of daily living scores, along with a stable reduction in anti-parkinsonian medication over the 5-year follow-up period.
2025-01-07BRAIN
Nav1.2 channel mutations preventing fast inactivation lead to SCN2A encephalopathy
Article
作者: Howell, Katherine B ; Tao, Elaine ; Corry, Ben ; Andersen, Erik ; Berecki, Géza ; Petrou, Steven ; Kahlig, Kris ; Wolff, Markus ; Coorg, Rohini K
Abstract:
SCN2A gene-related early-infantile developmental and epileptic encephalopathy (EI-DEE) is a rare and severe disorder that manifests in early infancy. SCN2A mutations affecting the fast inactivation gating mechanism can result in altered voltage dependence and incomplete inactivation of the encoded neuronal Nav1.2 channel and lead to abnormal neuronal excitability.In this study, we evaluated clinical data of seven missense Nav1.2 variants associated with DEE and performed molecular dynamics simulations, patch-clamp electrophysiology and dynamic clamp real-time neuronal modelling to elucidate the molecular and neuron-scale phenotypic consequences of the mutations.The N1662D mutation almost completely prevented fast inactivation without affecting activation. The comparison of wild-type and N1662D channel structures suggested that the ambifunctional hydrogen bond formation between residues N1662 and Q1494 is essential for fast inactivation. Fast inactivation could also be prevented with engineered Q1494A or Q1494L Nav1.2 channel variants, whereas Q1494E or Q149K variants resulted in incomplete inactivation and persistent current. Molecular dynamics simulations revealed a reduced affinity of the hydrophobic IFM-motif to its receptor site with N1662D and Q1494L variants relative to wild-type. These results demonstrate that the interactions between N1662 and Q1494 underpin the stability and the orientation of the inactivation gate and are essential for the development of fast inactivation. Six DEE-associated Nav1.2 variants, with mutations mapped to channel segments known to be implicated in fast inactivation were also evaluated. Remarkably, the L1657P variant also prevented fast inactivation and produced biophysical characteristics that were similar to those of N1662D, whereas the M1501V, M1501T, F1651C, P1658S and A1659V variants resulted in biophysical properties that were consistent with gain-of-function and enhanced action potential firing of hybrid neurons in dynamic action potential clamp experiments. Paradoxically, low densities of N1662D or L1657P currents potentiated action potential firing, whereas increased densities resulted in sustained depolarization.Our results provide novel structural insights into the molecular mechanism of Nav1.2 channel fast inactivation and inform treatment strategies for SCN2A-related EI-DEE. The contribution of non-inactivating Nav1.2 channels to neuronal excitability may constitute a distinct cellular mechanism in the pathogenesis of SCN2A-related DEE.
2023-04-01Neurobiology of disease
Biophysical characterization and modelling of SCN1A gain-of-function predicts interneuron hyperexcitability and a predisposition to network instability through homeostatic plasticity
Article
作者: Petrou, Steven ; Polster, Tilman ; Berecki, Géza ; Bryson, Alexander
SCN1A gain-of-function variants are associated with early onset developmental and epileptic encephalopathies (DEEs) that possess distinct clinical features compared to Dravet syndrome caused by SCN1A loss-of-function. However, it is unclear how SCN1A gain-of-function may predispose to cortical hyper-excitability and seizures. Here, we first report the clinical features of a patient carrying a de novo SCN1A variant (T162I) associated with neonatal-onset DEE, and then characterize the biophysical properties of T162I and three other SCN1A variants associated with neonatal-onset DEE (I236V) and early infantile DEE (P1345S, R1636Q). In voltage clamp experiments, three variants (T162I, P1345S and R1636Q) exhibited changes in activation and inactivation properties that enhanced window current, consistent with gain-of-function. Dynamic action potential clamp experiments utilising model neurons incorporating Nav1.1. channels supported a gain-of-function mechanism for all four variants. Here, the T162I, I236V, P1345S, and R1636Q variants exhibited higher peak firing rates relative to wild type and the T162I and R1636Q variants produced a hyperpolarized threshold and reduced neuronal rheobase. To explore the impact of these variants upon cortical excitability, we used a spiking network model containing an excitatory pyramidal cell (PC) and parvalbumin positive (PV) interneuron population. SCN1A gain-of-function was modelled by enhancing the excitability of PV interneurons and then incorporating three simple forms of homeostatic plasticity that restored pyramidal cell firing rates. We found that homeostatic plasticity mechanisms exerted differential impact upon network function, with changes to PV-to-PC and PC-to-PC synaptic strength predisposing to network instability. Overall, our findings support a role for SCN1A gain-of-function and inhibitory interneuron hyperexcitability in early onset DEE. We propose a mechanism through which homeostatic plasticity pathways can predispose to pathological excitatory activity and contribute to phenotypic variability in SCN1A disorders.
100 项与 Praxis Precision Medicines, Inc. 相关的药物交易
登录后查看更多信息
100 项与 Praxis Precision Medicines, Inc. 相关的转化医学
登录后查看更多信息
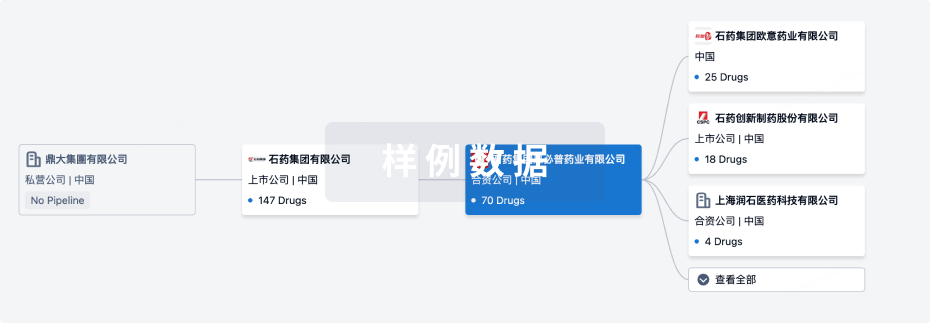
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月28日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
药物发现
1
12
临床前
临床3期
2
2
申请上市
其他
2
登录后查看更多信息
当前项目
登录后查看更多信息
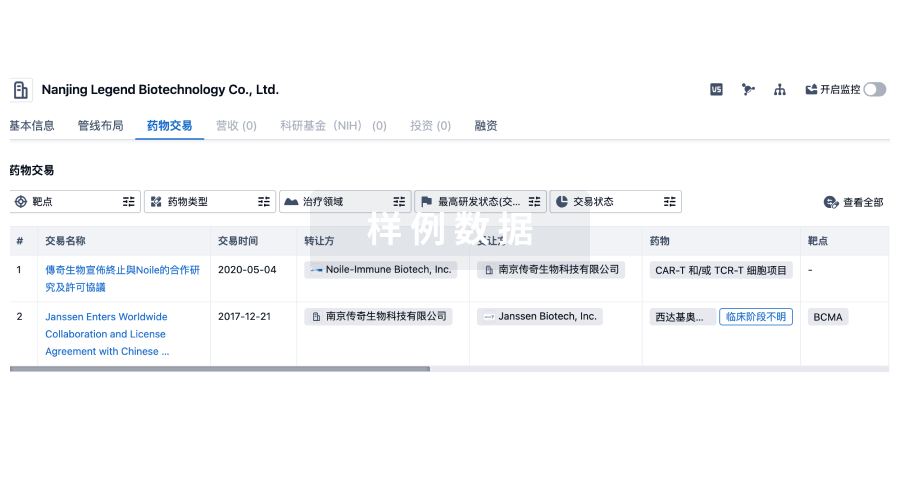
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
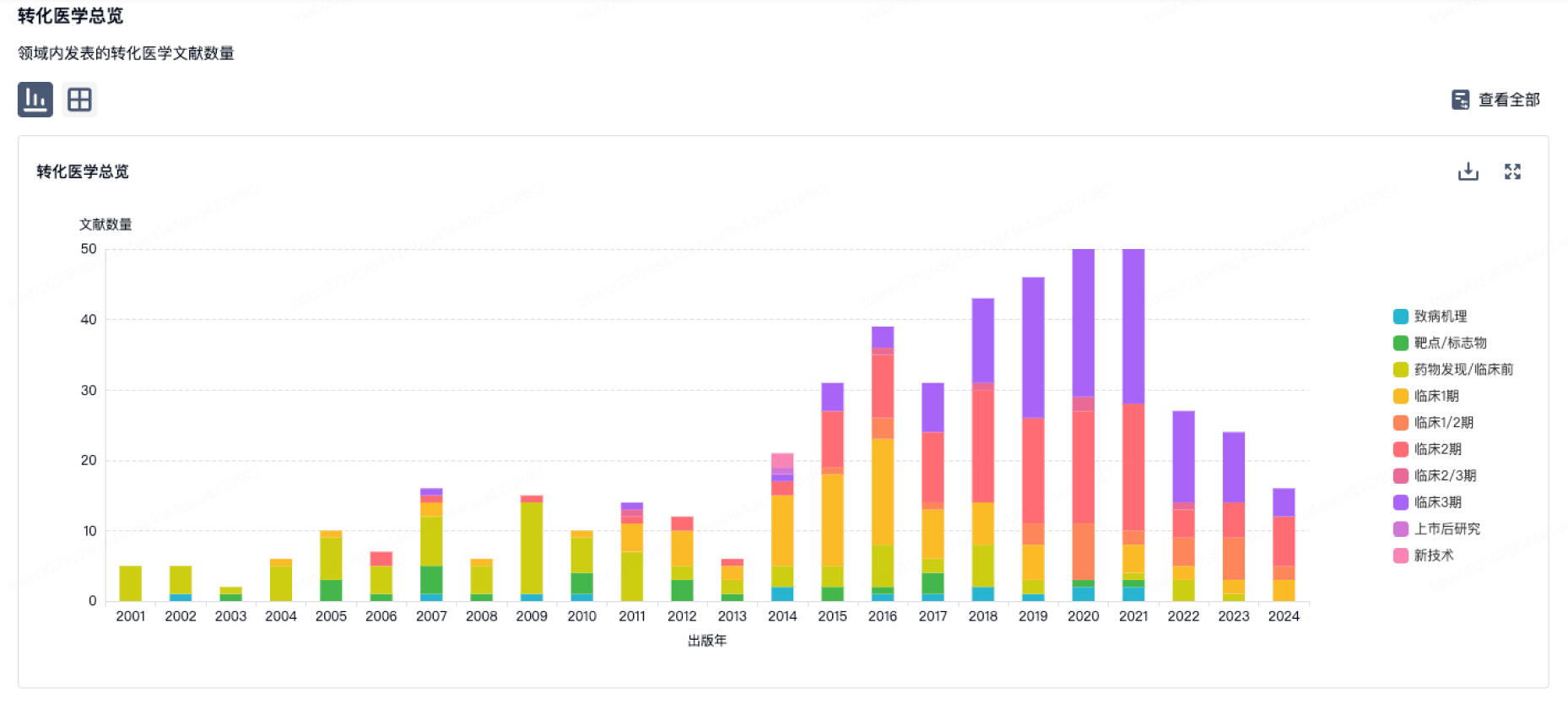
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用