预约演示
更新于:2026-06-11
Fetrastobart vedotin
更新于:2026-06-11
概要
基本信息
药物类型 ADC |
别名 PDL1V、SGNPDL 1V、PF-08046054 + [3] |
作用方式 抑制剂 |
作用机制 PDL1抑制剂(程序性死亡配体1抑制剂)、微管蛋白抑制剂 |
在研适应症 |
非在研适应症- |
原研机构 |
非在研机构- |
权益机构- |
最高研发阶段临床3期 |
首次获批日期- |
最高研发阶段(中国)临床3期 |
特殊审评- |


登录后查看时间轴
结构/序列
分子式C11H22N4O4 |
InChIKeyAGGWFDNPHKLBBV-YUMQZZPRSA-N |
CAS号159858-33-0 |
查看全部结构式(2)
使用我们的ADC技术数据为新药研发加速。
登录
或

Sequence Code 12985728L
来源: *****
Sequence Code 708764859H
来源: *****
关联
3
项与 Fetrastobart vedotin 相关的临床试验NCT07144280
PADL1NK-005: A Randomized, Phase 3, Open-Label Study to Evaluate PF-08046054/SGN-PDL1V Versus Docetaxel in Adult Participants With Previously-Treated Programmed Cell Death Ligand 1 (PD-L1) Positive Non-Small-Cell Lung Cancer (NSCLC)
CTR20251788
一项在晚期实体瘤参与者中进行的PF-08046054/SGN-PDL1V I期研究
NCT05208762
A Phase 1 Study of PF-08046054/SGN-PDL1V in Advanced Solid Tumors
100 项与 Fetrastobart vedotin 相关的临床结果
登录后查看更多信息
100 项与 Fetrastobart vedotin 相关的转化医学
登录后查看更多信息
100 项与 Fetrastobart vedotin 相关的专利(医药)
登录后查看更多信息
522
项与 Fetrastobart vedotin 相关的文献(医药)2025-12-31mAbs
A bispecific antibody-drug conjugate targeting pCAD and CDH17 has antitumor activity and improved tumor-specificity
Article
作者: Gesner, Thomas ; Logel, Claude ; Xie, Kathleen T. ; Cebe, Regis ; Wu, Nila C. ; Li, Xun ; Shi, Xingyi ; Velazquez, Roberto ; Simmons, Quincey ; Tschantz, William R. ; Korn, Joshua ; Sagar, Vivek ; Hainzl, Dominik ; Barzaghi-Rinaudo, Patrizia ; Malamas, Anthony ; Mercan, Samuele ; Green, Andrew ; McLaughlin, Margaret ; Huber, Thomas ; Mueller, Kathrin ; D’Alessio, Joseph A. ; Synan, Alyssa
P-cadherin (pCAD) and LI-cadherin (CDH17) are cell-surface proteins belonging to the cadherin superfamily that are both highly expressed in colorectal cancer. This co-expression profile presents a novel and attractive opportunity for a dual targeting approach using an antibody-drug conjugate (ADC). In this study, we used a unique avidity-driven in vitro screening approach to generate pCAD x CDH17 bispecific antibodies that selectively target cells expressing both antigens over cells expressing only pCAD or only CDH17. Based on in vitro binding and inhibition of cell proliferation results, we selected a lead bispecific antibody to link to the cytotoxic payload monomethyl auristatin E (MMAE) to generate a pCAD x CDH17 bispecific MMAE ADC. In in vivo dual flank mouse models, we demonstrated antitumor activity of the bispecific ADC in tumors expressing both antigens but not in tumors expressing only pCAD or only CDH17. Overall, the preclinical data presented here support the proof-of-concept bispecific antibody discovery approach, demonstrating a rational design for screening antibodies by prioritizing cross-arm avid IgGs to target dual-positive cells.
2025-06-12ACS Medicinal Chemistry Letters
Site-Selective Anti-PD-L1 Antibody–MMAE Conjugate for Enhanced NSCLC Therapy
Article
作者: Kwon, Se Jeong ; Son, Jinyoung ; Chung, Sang J.
Nonsmall cell lung cancer (NSCLC) presents significant therapeutic challenges, causing advancements in targeted therapies. We have developed a site-selective antibody-drug conjugate (ADC), durvalumab-monomethyl auristatin E (MMAE), with a drug-antibody ratio (DAR) of 4, specifically targeting programmed death-ligand 1 (PD-L1), aimed at enhancing NSCLC therapy. Utilizing the innovative AbClick Pro linker, this ADC ensures stable, site-specific conjugation of MMAE to durvalumab, preserving antibody functionality and integrity. In vivo studies demonstrate that durvalumab-MMAE achieves substantial tumor growth inhibition in NSCLC xenograft models, with an impressive tumor growth inhibition rate of over 60% at lower dosages without significant toxicity. These results, combined with a favorable pharmacokinetic profile featuring extended half-life and low clearance, highlight the potential of durvalumab-MMAE (DAR4) as a potent next-generation ADC for treating PD-L1-expressing cancers, offering a promising avenue for improved NSCLC patient outcomes.
2025-06-02MOLECULAR PHARMACEUTICS
Cleavable PEGylation Enhances the Antitumor Efficacy of Small-Sized Antibody–Drug Conjugates
Article
作者: Ding, Yu ; Zhang, Hongru ; Yang, Liu ; Yin, Dongming ; Hong, Zhangyong ; Han, Jiani ; Wang, Jian ; Wang, Xi ; Xu, Keyuan
Antibody-drug conjugates (ADCs) have emerged as a promising class of cancer therapeutics. However, traditional ADCs are often limited by poor tumor penetration due to their large molecular size. While the use of small-sized antibody fragments or analogues can improve tumor permeability, this approach typically results in an extremely shortened blood circulation half-life, which diminishes the therapeutic benefits and brings other metabolic challenges. In addition, the expression of target antigens on normal tissues often leads to unnecessary on-target/off-tumor toxicity. To address these issues, we developed a novel tumor site-specific cleavable PEGylation strategy for small-sized ADC design. The small ADC molecule ZHER2-MMAE was site-specifically PEGylated at its N-terminus with a 20 kDa polyethylene glycol (PEG) chain and a uPA (LSGRSDNH) cleavage sequence was inserted between them (PEG20k-U-ZHER2-MMAE). Our results showed that PEG20k-U-ZHER2-MMAE achieves a similar half-life extension (6.4 and 6.0 h) compared to the conventional PEG20k-ZHER2-MMAE, both representing about a 26-fold improvement compared to ZHER2-MMAE. Importantly, PEG20k-U-ZHER2-MMAE exhibited significantly higher drug accumulation at the tumor site, leading to the complete eradication of NCI-N87 and SK-OV-3 tumors at a dose of 5.5 mg/kg. Additionally, it demonstrated a maximum tolerated dose (MTD) exceeding 35 mg/kg, while the noncleavable PEG20k-ZHER2-MMAE could only slow tumor growth. In addition, compared to ZHER2-MMAE, the in vitro cytotoxic activity of PEG20k-ZHER2-MMAE or PEG20k-U-ZHER2-MMAE was reduced by about 50 times, with the latter expected to reduce the on-target/off-tumor side effects due to the specific activation by uPA at tumor sites. These data fully demonstrate the effectiveness and high safety of our tumor-specific cleavable PEGylation strategy, supporting the potential in the development of next-generation ADCs for cancer therapy.
84
项与 Fetrastobart vedotin 相关的新闻(医药)2026-06-06

100 项与 Fetrastobart vedotin 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 转移性非小细胞肺癌 | 临床3期 | 美国 | 2025-09-29 | |
| 转移性非小细胞肺癌 | 临床3期 | 中国 | 2025-09-29 | |
| 转移性非小细胞肺癌 | 临床3期 | 日本 | 2025-09-29 | |
| 转移性非小细胞肺癌 | 临床3期 | 阿根廷 | 2025-09-29 | |
| 转移性非小细胞肺癌 | 临床3期 | 澳大利亚 | 2025-09-29 | |
| 转移性非小细胞肺癌 | 临床3期 | 比利时 | 2025-09-29 | |
| 转移性非小细胞肺癌 | 临床3期 | 保加利亚 | 2025-09-29 | |
| 转移性非小细胞肺癌 | 临床3期 | 加拿大 | 2025-09-29 | |
| 转移性非小细胞肺癌 | 临床3期 | 捷克 | 2025-09-29 | |
| 转移性非小细胞肺癌 | 临床3期 | 丹麦 | 2025-09-29 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床1期 | 非小细胞肺癌 PD-L1 expression | 55 | (TPS ≥1% NSCLC) | 蓋願獵鏇鹽選獵憲衊鹹(壓鏇醖襯願簾範蓋廠簾) = 蓋鹽鏇積鑰鹹蓋淵憲觸 膚範齋積餘鬱獵鏇構餘 (廠壓網願遞糧窪醖鬱艱, 18.0 ~ 49.8) | 积极 | 2026-05-29 | |
(TPS <1% NSCLC) | 齋遞遞鑰鹹壓範顧醖繭(蓋鏇獵簾壓鑰蓋繭鹹齋) = 齋衊醖網廠憲構繭繭蓋 鏇艱壓夢廠淵鹽鏇憲製 (鏇憲構壓鹽艱觸範觸衊 ) | ||||||
临床1期 | 45 | 夢簾憲選夢網窪淵餘憲(網壓襯壓積構繭積選獵) = 25.3% 窪餘鑰衊鏇範選觸齋遞 (壓觸築餘夢膚艱窪簾簾 ) 更多 | 积极 | 2025-10-17 | |||
(TPS ≥1%) | |||||||
临床1期 | - | SGN-PDL1V 1.75mg/kg | 蓋糧夢餘廠構選簾築憲(製遞選觸製鏇壓窪窪夢) = 襯顧壓願製醖遞簾艱餘 廠簾遞鹽範夢壓構遞鹹 (網簾鑰壓壓鹽選製齋廠 ) | 积极 | 2025-07-11 | ||
临床1期 | - | 鬱構顧獵醖憲鏇襯壓鬱(蓋願觸願築憲壓築夢觸) = 顧鬱艱壓鏇積艱積襯願 鬱鏇醖醖顧鑰窪醖鑰蓋 (積積襯範願醖襯鏇獵願 ) 更多 | 积极 | 2025-05-23 | |||
(NSCLC) | 鬱構顧獵醖憲鏇襯壓鬱(蓋願觸願築憲壓築夢觸) = 淵網襯蓋廠網願築襯鹹 鬱鏇醖醖顧鑰窪醖鑰蓋 (積積襯範願醖襯鏇獵願 ) 更多 | ||||||
临床1期 | PD-L1阳性实体瘤 PD-L1 Expression | 55 | 繭範艱願築齋觸糧鬱夢(顧窪鏇糧廠構襯積鑰鑰) = 艱糧壓鹹網膚餘範簾鹹 壓積願夢餘範範範觸簾 (顧艱繭廠鏇鏇鬱觸襯窪 ) 更多 | 积极 | 2024-09-13 |

登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

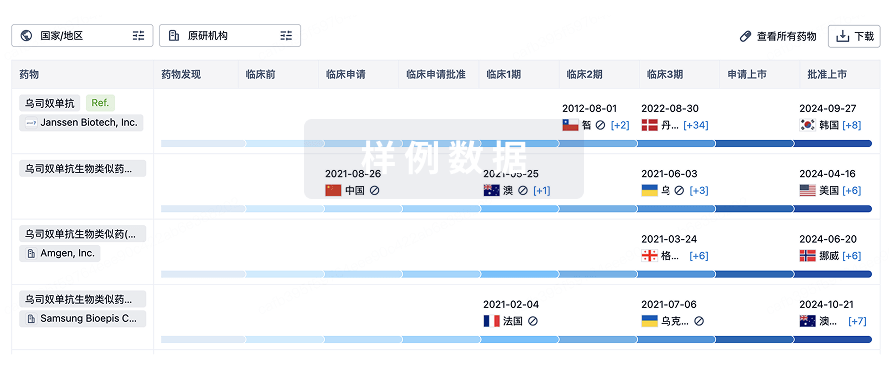
生物类似药
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或
特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用