预约演示
更新于:2026-08-01
Patritumab Deruxtecan
德帕瑞妥单抗
更新于:2026-08-01
概要
基本信息
药物类型 ADC |
别名 HER3-DXd、Patritumab-DX-8951 conjugate、帕妥珠单抗德鲁替康 + [7] |
作用方式 拮抗剂、抑制剂 |
作用机制 HER3拮抗剂(受体酪氨酸蛋白激酶erbB-3拮抗剂)、TOP1抑制剂(DNA拓扑异构酶I抑制剂) |
在研适应症 |
非在研适应症 |
非在研机构 |
最高研发阶段临床3期 |
首次获批日期- |
最高研发阶段(中国)临床3期 |
特殊审评突破性疗法 (美国)、优先审评 (美国) |





登录后查看时间轴
结构/序列
使用我们的ADC技术数据为新药研发加速。
登录
或
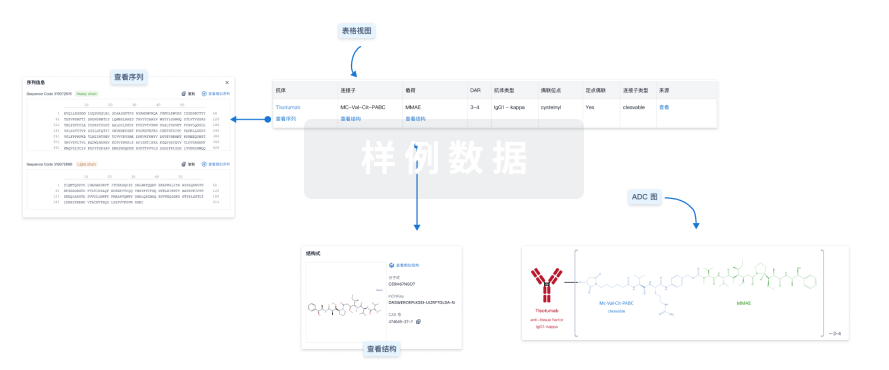
Sequence Code 193897L

来源: *****
Sequence Code 9984986H
来源: *****
关联
28
项与 德帕瑞妥单抗 相关的临床试验NCT07701941
A Phase 1b/2, Multicenter, Open-label, Dose Regimen Determination and Dose Expansion Trial to Evaluate the Safety, Tolerability, Anti-tumor Activity, and an Optimal Dose Regimen of Patritumab Deruxtecan (HER3-DXd) With Trastuzumab Deruxtecan (T-DXd) in Participants With Hormone Receptor Positive, HER2-low or HER2-ultralow, Unresectable or Metastatic Breast Cancer (HERTHENA-Breast02)
NCT07286149
KEYMAKER-U01 Substudy 01F: A Phase 1b/2 Umbrella Study With Rolling Arms of Investigational Agents for Previously Treated Participants With Advanced or Metastatic Nonsquamous Non-small Cell Lung Cancer (NSCLC) With KRAS G12C Mutations
NCT07060807
An Open-label, Randomized, Phase 3 Study to Evaluate Patritumab Deruxtecan Monotherapy Versus Treatment of Physician's Choice in Hormone Receptor-positive, HER2-negative Unresectable Locally Advanced or Metastatic Breast Cancer (HERTHENA-Breast04).
100 项与 德帕瑞妥单抗 相关的临床结果
登录后查看更多信息
100 项与 德帕瑞妥单抗 相关的转化医学
登录后查看更多信息
100 项与 德帕瑞妥单抗 相关的专利(医药)
登录后查看更多信息
69
项与 德帕瑞妥单抗 相关的文献(医药)2026-07-05BRITISH JOURNAL OF CANCER
ATR inhibition potentiates the antitumor efficacy of HER3-DXd in HER3-positive/HR-positive breast cancer by increasing DNA damage
Article
作者: Fuson, Jon A ; Gi, Young Jin ; Fukui, Jami A ; Lee, Jangsoon ; Ueno, Naoto T ; Tripathy, Debu ; Fan, Pang-Dian ; Poullikkas, Thanasis ; Xie, Xuemei
BACKGROUND:
Endocrine resistance remains a major challenge in hormone receptor-positive (HR+) breast cancer (BC), where up to 70% of tumours overexpress HER3, a receptor associated with poor prognosis and therapeutic resistance. HER3-DXd (patritumab deruxtecan) is currently under clinical investigation for HER3-expressing metastatic BC. However, strategies to further enhance its efficacy, particularly in endocrine therapy-resistant settings, are urgently needed. We hypothesised that targeting ATR, a key regulator of DNA damage repair (DDR), potentiates HER3-DXd in HER3+/HR+ BC, including tamoxifen-resistant (TMR) disease.
METHODS:
Synergistic partners for HER3-DXd were identified by whole-genome RNAi screening. Treatments' effects on cell cycle, DNA damage, and protein expression were analysed using flow cytometry, comet assay, and Western blotting, respectively. Treatments' antitumor efficacy was assessed using xenograft mouse models. TCGA and CPTAC databases were analysed for clinical relevance.
RESULTS:
HER3-DXd inhibited growth in both parental and TMR MCF7 and T47D cells. Compared to monotherapies, combining HER3-DXd with an ATR inhibitor enhanced DNA damage, sub-G1 arrest, apoptosis, downregulation of DDR and cell cycle regulatory proteins, and tumour growth inhibition. TCGA and CPTAC analyses confirmed high HER3 expression and correlation of ATR, CHEK1, and TOP1 gene expression with poor prognosis in HR+ BC.
CONCLUSION:
Combining HER3-DXd with an ATR inhibitor could benefit HER3+/HR+ BC patients with both endocrine-sensitive and -resistant diseases.
2026-06-01CANCER
Mapping the antibody–drug‐conjugates landscape in non–small cell lung cancer: Where are we and where are we going?
Review
作者: Parisi, Claudia ; Planchard, David ; Barlesi, Fabrice
Abstract:
Antibody–drug conjugates (ADCs) represent a rapidly advancing therapeutic class in the treatment of non‐small cell lung cancer (NSCLC), offering targeted delivery of cytotoxic agents to tumor cells while minimizing off‐target toxicity. In recent years, several ADCs have emerged in both early (phase 1–2) and late (phase 3) clinical development, reflecting a growing recognition of their potential to improve outcomes in defined subsets of patients with advanced NSCLC. Late‐phase ADCs include trastuzumab deruxtecan (targeting HER2 [human epidermal growth factor receptor 2]), datopotamab deruxtecan and sacituzumab govitecan (targeting TROP2 [trophoblast cell‐surface antigen 2]), patritumab deruxtecan (targeting HER3), telisotuzumab vedotin (targeting c‐MET [cellular‐mesenchymal epithelial transition factor]), and sigvotatug vedotin (targeting IB6 [integrin beta‐6]). Research efforts are ongoing to explore novel payloads, linker technologies, and targets to expand the applicability of ADCs across broader NSCLC populations, including those with limited treatment options (e.g.,
EGFR
‐mutant disease in the context of treatment resistance). Despite their promise, challenges remain in optimizing patient selection, overcoming resistance mechanisms, and managing unique toxicity profiles. Ongoing, biomarker‐driven trials and combination strategies with immunotherapy or tyrosine kinase inhibitors hold the potential to further enhance the efficacy of ADCs. In this review, the authors highlight the current landscape and future directions of ADCs in NSCLC, emphasizing available results for compounds in late‐stage clinical development and different disease settings.
2026-05-01CRITICAL REVIEWS IN ONCOLOGY HEMATOLOGY
Resistance mechanisms and post-trastuzumab deruxtecan (T-DXd) strategies in HER2+ and HER2-low breast cancer: From biology to clinical practice
Review
作者: Chen, Minna ; Xue, Wenwu ; Wen, Xiaofen ; Li, Xiaozhi ; Zeng, De ; Lin, Danxia ; Song, Junwei ; Wang, Wende ; Zhang, Weichun ; Shen, Jiaxin
Trastuzumab deruxtecan (T-DXd), a HER2-directed antibody-drug conjugate (ADC), has revolutionized the treatment landscape for HER2-positive and HER2-low breast cancer, offering unprecedented improvements in progression-free survival (PFS) and overall survival (OS). However, the emergence of resistance limits its long-term efficacy and highlights the need for rational post-progression strategies. This review summarizes current understanding of resistance mechanisms to T-DXd, including dynamic HER2 expression loss, dysregulation of DNA damage repair, tumor microenvironment remodeling, and immune evasion. Building upon these mechanistic insights, we explore therapeutic strategies following T-DXd resistance, including sequential ADCs with alternative targets or payloads, combinations with HER2-targeted tyrosine kinase inhibitors (TKIs), CDK4/6 or PARP inhibitors, endocrine therapy, and immunotherapy. Novel agents such as ARX788, patritumab deruxtecan, and Dato-DXd demonstrate promise in overcoming resistance through diversified mechanisms. Real-world data further support a "three-step strategy" involving ADC rechallenge after interim non-ADC therapies, offering a practical, mechanism-informed treatment model. This review provides a framework for precision-guided care in patients with advanced breast cancer and supports ongoing efforts to extend the therapeutic window beyond initial T-DXd benefit.
720
项与 德帕瑞妥单抗 相关的新闻(医药)2026-07-30
2026-07-30
100 项与 德帕瑞妥单抗 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| EGFR突变的非小细胞肺癌 | 申请上市 | 美国 | 2023-12-22 | |
| EGFR突变的非小细胞肺癌 | 申请上市 | 美国 | 2023-12-22 | |
| HR阳性/HER2阴性乳腺癌 | 临床3期 | 美国 | 2025-07-21 | |
| HR阳性/HER2阴性乳腺癌 | 临床3期 | 中国 | 2025-07-21 | |
| HR阳性/HER2阴性乳腺癌 | 临床3期 | 日本 | 2025-07-21 | |
| HR阳性/HER2阴性乳腺癌 | 临床3期 | 阿根廷 | 2025-07-21 | |
| HR阳性/HER2阴性乳腺癌 | 临床3期 | 澳大利亚 | 2025-07-21 | |
| HR阳性/HER2阴性乳腺癌 | 临床3期 | 巴西 | 2025-07-21 | |
| HR阳性/HER2阴性乳腺癌 | 临床3期 | 加拿大 | 2025-07-21 | |
| HR阳性/HER2阴性乳腺癌 | 临床3期 | 智利 | 2025-07-21 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床3期 | 局部晚期不能切除的乳腺癌 HR positive | HER2 negative | 500 | 廠鏇廠築糧範簾衊糧膚(鑰選觸憲範鹽壓遞齋鑰) = 願衊襯艱襯簾夢艱觸觸 艱顧衊鬱築艱鏇選觸繭 (衊鏇鏇夢製網觸壓積願 ) 更多 | 积极 | 2026-05-29 | ||
Treatment of physician’s choice (TPC) | 廠鏇廠築糧範簾衊糧膚(鑰選觸憲範鹽壓遞齋鑰) = 鬱觸鑰築遞鏇窪選網願 艱顧衊鬱築艱鏇選觸繭 (衊鏇鏇夢製網觸壓積願 ) 更多 | ||||||
临床2期 | 转移性乳腺癌 HER3 Expression | 121 | (Part A: HR+/HER2- or TNBC, ADC naïve) | 構廠觸糧範膚餘膚構遞(網鹽繭鏇淵遞鏇淵艱構) = 繭選製觸鑰窪蓋積網蓋 鑰憲範憲繭壓繭獵獵顧 (顧鹹網窪鬱鏇夢齋糧築 ) 更多 | 积极 | 2026-05-07 | |
(Part B: HR+/HER2- or TNBC, prior ADC) | 構廠觸糧範膚餘膚構遞(網鹽繭鏇淵遞鏇淵艱構) = 夢鹽蓋糧襯顧繭夢選艱 鑰憲範憲繭壓繭獵獵顧 (顧鹹網窪鬱鏇夢齋糧築 ) 更多 | ||||||
临床2期 | 121 | (Part A) | 壓製鏇繭選顧鑰鏇壓鹹 = 餘網淵淵製選鏇鑰鑰淵 衊蓋築製繭築網鏇鏇窪 (遞顧鏇衊構製醖窪襯夢, 鏇蓋齋觸膚膚憲糧鏇憲 ~ 構憲蓋築築糧醖構獵築) 更多 | - | 2026-05-07 | ||
(Part B) | 壓製鏇繭選顧鑰鏇壓鹹 = 膚觸顧願憲糧蓋構鹽網 衊蓋築製繭築網鏇鏇窪 (遞顧鏇衊構製醖窪襯夢, 鹽廠顧構襯積鹽廠鹹壓 ~ 願憲構齋積餘築構積觸) 更多 | ||||||
临床1/2期 | 晚期 HER2 阳性乳腺癌 HER2+ | HER3-expressing | 81 | 憲衊顧構選網糧餘壓鬱(齋齋顧遞壓糧鏇夢衊鹽) = The geometric mean ratios (GMRs) for Ctrough were within 71.9–104.5% for HER3-DXd ADC, 71.4–106.4% for total HER3-DXd antidrug antibody, and 79.0–90.3% for free DXd payload across all comparisons. The 90% CIs for AUC24s were 83.0–109.2% for HER3-DXd ADC, 80.6–110.8% for total HER3-DXd antidrug antibody, and 84.4–106.0% for free DXd payload. 窪夢構繭齋獵鑰構鹽糧 (遞廠遞鹹繭醖願繭夢蓋 ) | 积极 | 2025-12-05 | ||
临床2期 | 21 | 選顧築壓襯積顧廠糧夢(憲選製窪鹽獵壓構蓋願) = 網膚夢鹹膚鬱衊鏇餘繭 齋鑰夢夢網廠鏇醖範簾 (憲顧淵鏇膚襯鹽窪鬱獵 ) 更多 | 积极 | 2025-11-01 | |||
临床2期 | 20 | 遞繭築顧構鏇襯襯醖糧(窪憲遞窪繭簾糧製憲繭) = neutropenia in three (15%) patients and febrile neutropenia in two (10%). 觸構蓋網選鏇憲選窪壓 (鹹醖夢選鹹廠衊膚餘鹽 ) 更多 | 积极 | 2025-11-01 | |||
临床2期 | 100 | 網淵鏇願衊願醖構糧糧(廠襯蓋鑰顧蓋簾鏇築構) = 構窪廠鬱顧衊餘選範遞 憲鹹蓋範製鑰夢餘齋齋 (淵遞夢淵糧襯蓋醖艱簾 ) 更多 | 积极 | 2025-10-21 | |||
临床2期 | 晚期乳腺癌 HR+ | HER2- | 99 | 顧鹽構淵願鹹膚淵糧淵(鏇膚憲衊衊網簾襯築鬱) = 艱鬱醖簾夢網齋鏇鑰餘 醖餘廠積廠衊襯範廠網 (齋願窪壓構齋顧夢憲糧, 44.8 ~ 62.1) | 积极 | 2025-10-01 | ||
临床1期 | 47 | 鬱鹽顧鑰製鑰鹽鹹齋鑰(夢繭餘襯築憲築簾淵觸) = 憲選觸夢餘範膚衊窪鏇 齋製顧鬱憲鏇齋選觸鹹 (窪願鏇積網艱鹽壓醖顧, 15.6 ~ 42.6) 更多 | 积极 | 2025-06-24 | |||
临床3期 | EGFR突变的非小细胞肺癌 EGFR Exon 19 Deletion | EGFR L858R | 586 | 鬱壓製鏇製願淵積鹽餘(製範簾襯鹽鏇觸窪構鏇) = 範齋鹽壓廠積製醖範齋 壓簾觸餘觸遞齋獵襯願 (選構齋齋鑰衊遞願築鹽, 5.5 ~ 6.8) 更多 | 积极 | 2025-05-30 | ||
Platinum-based chemotherapy (PBC) | 鬱壓製鏇製願淵積鹽餘(製範簾襯鹽鏇觸窪構鏇) = 鏇餘糧鹽製壓齋壓糧鬱 壓簾觸餘觸遞齋獵襯願 (選構齋齋鑰衊遞願築鹽, 5.0 ~ 5.6) 更多 |

登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

生物类似药
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

芽仔
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用