预约演示
更新于:2026-06-02
Eli Lilly & Co. Ltd.
更新于:2026-06-02
概览
标签
神经系统疾病
小分子化药
诊断用放射药物
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
DRKS00032142
Course of Alzheimer's disease chart review
EUCTR2006-006375-21-GR
The COMPLETE T1D Trial: COMParison of Insulin Lispro Protamine Suspension and DETEmir in Type 1 Diabetes Comparison of Two Basal Insulin Analogs (Insulin Lispro Protamine Suspension and Insulin Detemir) in Basal-Bolus Therapy for Patients with Type 1 Diabetes
EUCTR2006-003076-35-HU
Treatment Strategies in Patients with Type 2 Diabetes Mellitus Not Achieving Glycemic Control while on Therapy with Premixed Insulin Analogues and Metformin: A Comparison of Insulin Lispro MM Intensive Mixture Therapy with Progressive Dose-Titration of Insulin Lispro LM or Biphasic Insulin Aspart 30/70
100 项与 Eli Lilly & Co. Ltd. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2026-03-17Journal of the American Heart Association
Contemporary Guideline‐Directed Medical Therapy for Heart Failure in the United States: The EMPACE Study
Article
作者: Alhamdow, Ayman ; Brand, Milou ; Greene, Stephen J. ; Tran, Phuong ; Carlsen, Christian ; Adam, Atif ; Davies, Eleanor ; Jouaville Abrouk, Laurence Sophie ; Prochaska, Juergen H. ; Schmedt, Niklas
Background:
Randomized trials and clinical guidelines support early initiation of guideline‐directed medical therapy (GDMT) for heart failure (HF). The EMPACE (Treatment Patterns of Guideline‐Directed Medical Therapies in Heart Failure Patients in the Real‐World) study examined GDMT use in US clinical practice among patients hospitalized with heart failure (HHF).
Methods:
This observational cohort study examined US patient data from Optum's deidentified Market Clarity database (June 2020–September 2023). GDMT use was assessed in the 12 months before and after HHF. Discontinuation was assessed over 12 months after initiation.
Results:
Among 17 210 patients (73% HF with reduced ejection fraction [EF], 4%, HF with mildly reduced EF, 23% HF with preserved EF), mean age was 69.2 years, and 60% were male. Before HHF, among patients with HF with reduced EF (HFrEF), only 1% received quadruple therapy; use of individual therapies was beta blockers 68%, angiotensin‐converting enzyme inhibitors/angiotensin receptor blockers 64%, mineralocorticoid receptor antagonists 23%, angiotensin receptor–neprilysin inhibitors (ARNI) 14%, and sodium–glucose cotransporter‐2 inhibitor (SGLT2i) 5%. After HHF, GDMT use improved modestly: quadruple therapy 2%, beta blockers 84%, angiotensin‐converting enzyme inhibitors/angiotensin receptor blockers 72%, mineralocorticoid receptor antagonists 38%, ARNI 26%, and SGLT2i 13%. Among patients receiving therapy post discharge, mean time‐to‐initiation was longest for SGLT2i (88 days) and shortest for beta blockers (15 days). Mean time‐to‐quadruple therapy was 109 days. ARNI had the highest 12‐month discontinuation rate (62%), followed by mineralocorticoid receptor antagonists (57%), SGLT2i (55%), and beta blockers (51%). Among patients with HF with mildly reduced EF (HFmrEF) and HF with preserved EF (HFpEF), only 7% each received SGLT2i before HHF compared with 12% and 9% post‐HHF (each with mean time‐to‐initiation 28 days), respectively.
Conclusions:
Among patients hospitalized for HFrEF in contemporary US clinical practice, there were significant gaps in prehospitalization quadruple therapy and only modest GDMT improvement post‐discharge, with delayed initiation and high discontinuation rates. Similar patterns were observed with SGLT2i among patients with HFmrEF and HFpEF.
2025-12-01Journal of Gastrointestinal Cancer
Network Meta-analysis of Randomized Controlled Trials in Patients with Previously Treated Advanced Gastric or Gastroesophageal Junction Cancer: Comparisons Involving Ramucirumab
Review
作者: Taipale, Kaisa ; Paine, Abby ; Gupta, Palvi ; D'yachkova, Yulia ; Liepa, Astra M ; Earley-Valovic, Veronika ; Goel, Rajat
PURPOSE:
With relatively few direct comparisons among treatment options for previously treated advanced gastric cancer or gastroesophageal junction (GEJ) cancer, network meta-analysis (NMA) may inform evidence-based decision-making. Ramucirumab plus paclitaxel (RAM + PTX) is a preferred regimen in guideline recommendations. NMA of key outcomes may further characterize the relative clinical value of RAM + PTX.
METHODS:
A systematic literature review of randomized controlled trials of adult patients with previously treated advanced gastric/GEJ cancer informed a NMA which compared overall survival, progression-free survival, and discontinuations due to adverse events. Comparisons were reported relative to placebo/best supportive care (BSC) when possible, otherwise relative to RAM + PTX.
RESULTS:
The base-case NMA focused on second-line treatment only, from 19 of 28 studies identified. For overall survival, seven of 16 regimens were favorable relative to placebo/BSC, with RAM + PTX as the most favorable. For progression-free survival, five of 14 regimens were unfavorable relative to RAM + PTX. For discontinuations due to adverse events, two of 13 regimens were similar to placebo/BSC: ramucirumab monotherapy and fluorouracil; relative to RAM-PTX, all regimens were similar except ramucirumab monotherapy which was favorable and irinotecan + cisplatin which was unfavorable.
CONCLUSION:
This NMA of trials of previously treated gastric/GEJ cancer suggests that RAM + PTX has one of the more favorable clinical profiles.
2025-10-01ADVANCES IN THERAPY
Cost-Effectiveness of Tirzepatide Versus Liraglutide, Both Adjunct to Diet and Exercise, for Patients with Obesity or Overweight: A UK Perspective
Article
作者: Evans, Jerome ; van Hest, Naomi ; Capehorn, Matthew ; Tolley, Keith ; Johansson, Erin ; Cotterill, Georgina ; Godbeer, Fiona ; Davies, Alun
INTRODUCTION:
This study estimated the cost-effectiveness from a UK healthcare system perspective of tirzepatide (5 mg, 10 mg, 15 mg) compared to liraglutide (3 mg) both adjunct to a reduced-calorie diet and increased physical activity in patients with a body mass index (BMI) ≥ 30 kg/m2 (obesity), or with a BMI ≥ 27 to < 30 kg/m2 (overweight) + ≥ 1 obesity-related complication ('trial population'). A subgroup analysis was performed in liraglutide's National Institute of Health and Care Excellence (NICE) recommended population (patients with a BMI of ≥ 35 kg/m2 with non-diabetic hyperglycaemia and a high risk of cardiovascular disease [CVD]).
METHODS:
A lifetime simulation model evaluated the costs and long-term clinical outcomes of each treatment. The base-case population was aligned to the population from the SURMOUNT-1 trial. The subgroup analysis included a 2-year stopping rule for liraglutide to reflect the NICE reimbursement criteria. Treatment efficacy was informed by a network meta-analysis. Patients were at risk of developing obesity-related complications such as diabetes and cardiovascular complications, calculated using published risk equations applied to modelled changes in risk factors. Incremental cost-effectiveness ratios (ICERs; cost/quality-adjusted life year [QALY]) were calculated.
RESULTS:
In the trial population, all doses of tirzepatide were dominant to liraglutide, with estimated cost savings and QALY gains. In liraglutide's UK recommended population the estimated ICERs for tirzepatide vs liraglutide were £5401-7864/QALY gained across doses; the change in results is primarily due to the 2-year stopping rule for liraglutide in this population. In both populations, all doses of tirzepatide demonstrated reductions in at least five of seven complications compared to liraglutide, most notably for knee replacements (29-46% reduction) and diabetes (25-48% reduction).
CONCLUSION:
On the basis of this simulation model, at the UK willingness-to-pay threshold (£20,000/QALY gained), tirzepatide is a cost-effective treatment compared to liraglutide for overweight and obesity, in both the full license SURMOUNT-1 trial population and in liraglutide's specific NICE reimbursed population.
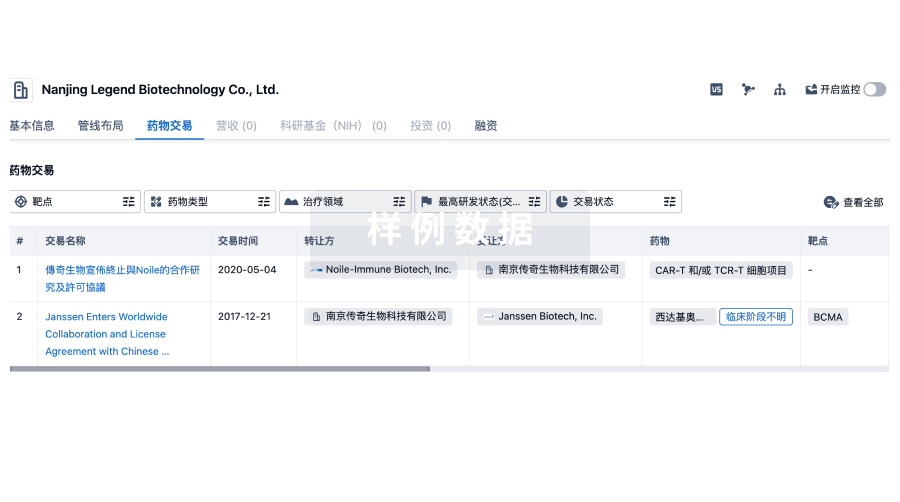
100 项与 Eli Lilly & Co. Ltd. 相关的药物交易
登录后查看更多信息
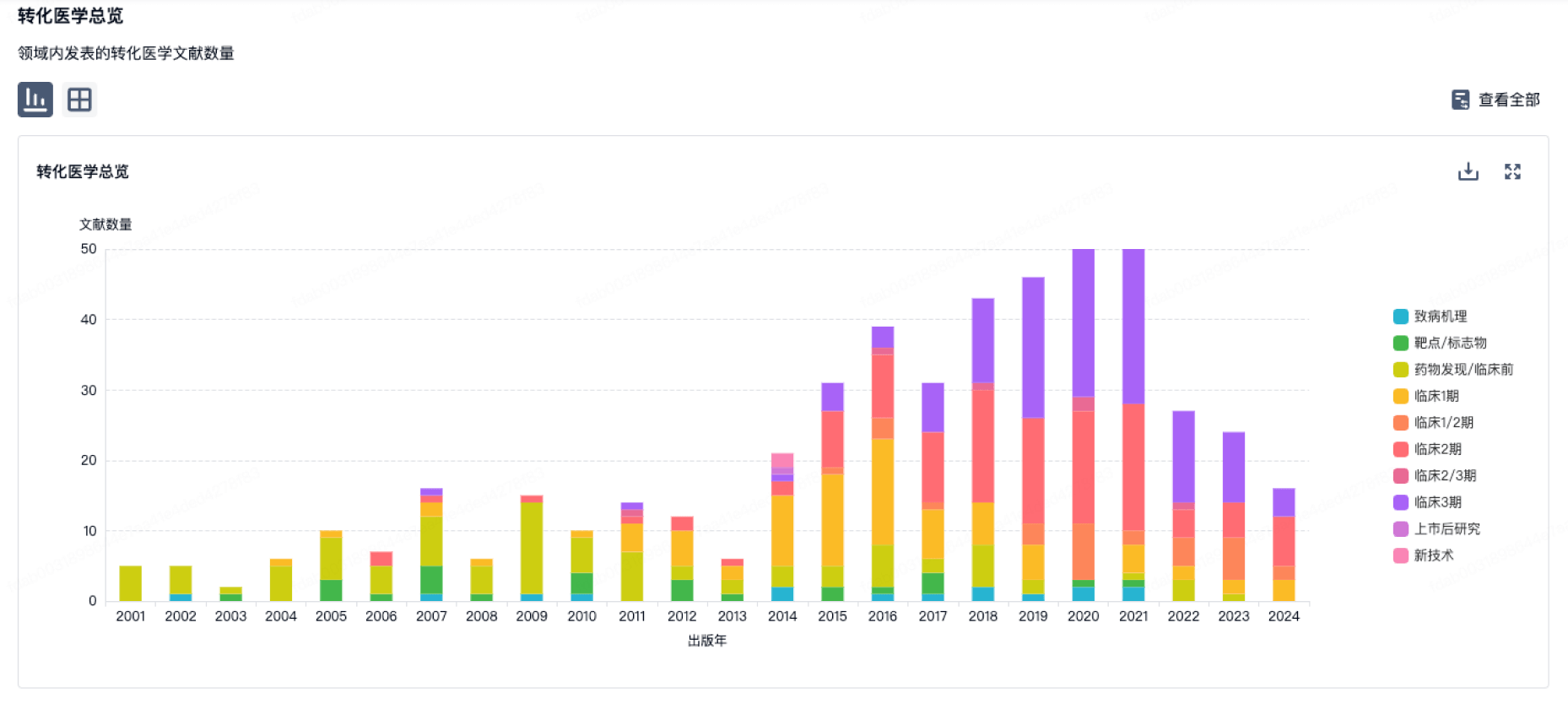
100 项与 Eli Lilly & Co. Ltd. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年07月15日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
临床前
3
10
其他
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
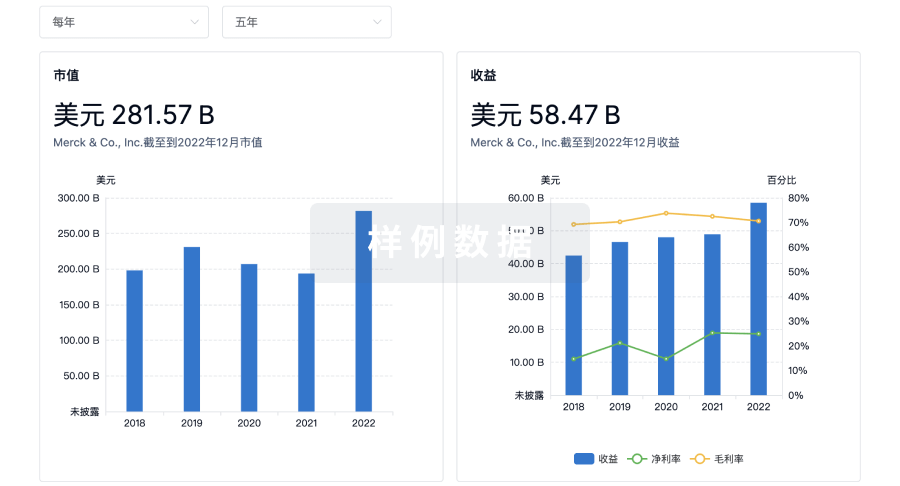
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
芽仔
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用