预约演示
更新于:2026-04-14
Eculizumab
依库珠单抗
更新于:2026-04-14
概要
基本信息
药物类型 单克隆抗体 |
别名 Anti-C5 monoclonal antibody 5G1-1、Eculizumab (Genetical Recombination)、Eculizumab (genetical recombination) (JAN) + [16] |
靶点 |
作用方式 抑制剂 |
作用机制 C5抑制剂(补体C5抑制剂) |
在研适应症 |
非在研适应症 |
非在研机构- |
最高研发阶段批准上市 |
首次获批日期 美国 (2007-03-16), |
最高研发阶段(中国)批准上市 |
特殊审评孤儿药 (美国)、孤儿药 (欧盟)、优先审评 (中国)、孤儿药 (日本)、孤儿药 (韩国)、孤儿药 (澳大利亚) |


登录后查看时间轴
结构/序列
Sequence Code 66437L
来源: *****
Sequence Code 66453H
来源: *****
关联
68
项与 依库珠单抗 相关的临床试验NCT05646563
A Phase II, Open-Label Study of NM8074 in Soliris®-Treated Patients With Paroxysmal Nocturnal Hemoglobinuria (PNH)

NCT07010302
A Comparative Clinical Effectiveness Trial of Rituximab Versus Ravulizumab, Inebilizumab, Satralizumab and Eculizumab To Prevent Relapses in Neuromyelitis Optica Spectrum Disorder

NCT07410039
Eculizumab Add-On Therapy in the Acute Phase of Neuromyelitis Optica Spectrum Disorder: A Multicenter Prospective Real-World Study
100 项与 依库珠单抗 相关的临床结果
登录后查看更多信息
100 项与 依库珠单抗 相关的转化医学
登录后查看更多信息
100 项与 依库珠单抗 相关的专利(医药)
登录后查看更多信息
2,478
项与 依库珠单抗 相关的文献(医药)2026-12-31Hematology
Improvement in anemia and symptoms after switching from crovalimab to iptacopan in paroxysmal nocturnal hemoglobinuria
Article
作者: Onizuka, Makoto ; Ogawa, Yoshiaki ; Nasukawa, Miina ; Ogiya, Daisuke ; Koyama, Seina ; Machida, Shinichiro ; Kawada, Hiroshi ; Shiraiwa, Sawako ; Tomita, Shunsuke ; Endo, Motoki ; Toyosaki, Masako
OBJECTIVES:
Paroxysmal nocturnal hemoglobinuria (PNH) may develop breakthrough hemolysis (BTH) despite C5 inhibition. Although iptacopan, an oral factor B inhibitor, has demonstrated efficacy in phase 3 trials, switching from crovalimab has not been reported. We describe the first clinical case of this switch in a real-world clinical setting.
METHODS:
A 72-year-old man with long-standing PNH received eculizumab followed by crovalimab. Infectious enteritis triggered BTH and worsening anemia during crovalimab therapy. Because anemia persisted after recovery, iptacopan 200 mg twice daily was initiated three weeks after the final crovalimab administration. Clinical symptoms and laboratory parameters were followed for 12 months. This case report complied with the Declaration of Helsinki.
RESULTS:
Hemoglobin increased from 9.6 to 11.6 g/dL within two weeks and remained ≥12 g/dL thereafter. Dyspnea resolved within one week, vitality improved by two weeks, and no BTH or treatment-related adverse events occurred during follow-up.
DISCUSSION:
This case demonstrates the feasibility of switching from crovalimab to iptacopan despite the absence of an established method, and pharmacokinetic considerations guided the timing.
CONCLUSION:
Switching to iptacopan led to rapid and durable improvement in anemia and symptoms, supporting proximal complement inhibition as a valuable option for PNH patients inadequately controlled with C5 inhibitors.
2026-12-31JOURNAL OF MEDICAL ECONOMICS
Cost per responder analysis of iptacopan versus eculizumab and ravulizumab in treatment of paroxysmal nocturnal hemoglobinuria: implications for decision-making
Article
作者: Shafrin, Jason ; Muthukrishnan, Sanjana ; Kuypers, Nicholas ; Bilano, Ver ; Than, Kyi-Sin ; Paulose, Jincy
OBJECTIVE:
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare and debilitating hematological disease with significant economic burden. Despite the availability of multiple therapies, there is a lack of consensus on optimal treatment strategies among physicians and payers in the United States. This study aimed to evaluate the economic value of iptacopan, a novel oral treatment option, compared to terminal complement inhibitors (specifically, complement component C5 inhibitor or C5i)-including eculizumab and ravulizumab-among patients with PNH who are either (i) C5i-experienced or (ii) complement-inhibitor-naïve.
METHODS:
A cost per responder analysis was conducted based on treatment efficacy from clinical trials comparing iptacopan with C5i treatments. Treatment response was defined as the proportion of patients achieving red blood cell transfusion independence. Treatment costs were estimated as pharmaceutical wholesale acquisition cost and treatment administration costs, accounting for discontinuation. Outcomes evaluated included the number needed to treat to achieve a response and the cost per responder over the treatment duration of 24 weeks.
RESULTS:
Over 24 weeks, the number needed to treat to achieve an additional response was lower for iptacopan than all C5i comparators (C5i-experienced: 1.05 with iptacopan vs. 3.86 with C5is; complement-inhibitor-naïve: 1.02 with iptacopan vs. 1.69 with C5is). Cost per responder was lower for iptacopan than C5i comparators for both C5i-experienced ($264,337 for iptacopan vs. $975,298 for ravulizumab, $1,060,511 for eculizumab, and $744,561-$955,194 for eculizumab biosimilar with 10%-30% discount from eculizumab cost) and complement-inhibitor-naïve patients ($256,754, vs. $428,139 for ravulizumab, $465,546 for eculizumab, and $326,849-$419,314 for eculizumab biosimilar).
CONCLUSION:
Among both C5i-experienced and complement-inhibitor-naïve patients, treatment with iptacopan resulted in higher response rates and lower cost per responder compared to C5is.
2026-06-01IMMUNOLOGY LETTERS
Complement involvement in antiphospholipid syndrome
Review
作者: Darnige, Luc ; Dragon Durey, Marie-Agnès ; Hamidi, Houcine
Antiphospholipid syndrome (APS) is an acquired thrombophilia characterized by thrombotic and non-thrombotic (or non-criteria) manifestations, in the context of persistent presence of autoantibodies targeting phospholipids and associated proteins. The complement system, which shares common actors with coagulation cascade, is nowadays well established to be implicated in APS pathophysiology in different ways. Animal models using knock out strains or complement blocking therapies have helped to decipher the different complement components implicated in the processes of thrombosis and fetal morbidity. In APS patients, complement activation may be assessed through the detection of activation fragments (C4d, C3a, C5a, sC5b9) in plasma and on blood cells surface (C4d, C3d and C5b9) or on APS-affected tissues such as cardiac valves, vessels walls, kidneys and placentae. APS patients are currently treated to avoid thrombosis recurrence by long-term treatment by vitamin K antagonists but various complement targeting molecules are tested in trials or now available and may be of major interest to treat APS patients. Several cases report described the use of eculizumab, an anti-C5 monoclonal antibody, to treat severe forms of APS (recurrent thrombosis, Catastrophic APS) but these studies are not sufficient and need to be more standardized. C4d measurement may be useful to assess classical and lectin pathways activation, C5a may allow evaluating the C5a/C5aR axis activity whereas, associated with sC5b9, it may also assess the terminal pathway activation but also the therapeutic efficacy of complement blocking molecules. Thus, assessment of good complement biomarkers and their kinetics needs to be done to determine personalized therapeutic options.
100 项与 依库珠单抗 相关的药物交易
登录后查看更多信息
研发状态
批准上市
10 条最早获批的记录, 后查看更多信息
登录
| 适应症 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|
| 水通道蛋白4抗体阳性视神经脊髓炎谱系疾病 | 澳大利亚 | 2009-03-20 | |
| 非典型溶血性尿毒症综合征 | 欧盟 | 2007-06-20 | |
| 非典型溶血性尿毒症综合征 | 冰岛 | 2007-06-20 | |
| 非典型溶血性尿毒症综合征 | 列支敦士登 | 2007-06-20 | |
| 非典型溶血性尿毒症综合征 | 挪威 | 2007-06-20 | |
| 重症肌无力 | 欧盟 | 2007-06-20 | |
| 重症肌无力 | 冰岛 | 2007-06-20 | |
| 重症肌无力 | 列支敦士登 | 2007-06-20 | |
| 重症肌无力 | 挪威 | 2007-06-20 | |
| 视神经脊髓炎 | 欧盟 | 2007-06-20 | |
| 视神经脊髓炎 | 冰岛 | 2007-06-20 | |
| 视神经脊髓炎 | 列支敦士登 | 2007-06-20 | |
| 视神经脊髓炎 | 挪威 | 2007-06-20 | |
| 阵发性睡眠性血红蛋白尿症 | 美国 | 2007-03-16 |
未上市
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 移植物功能延迟恢复 | 临床3期 | 美国 | 2014-08-21 | |
| 移植物功能延迟恢复 | 临床3期 | 澳大利亚 | 2014-08-21 | |
| 移植物功能延迟恢复 | 临床3期 | 巴西 | 2014-08-21 | |
| 移植物功能延迟恢复 | 临床3期 | 加拿大 | 2014-08-21 | |
| 移植物功能延迟恢复 | 临床3期 | 捷克 | 2014-08-21 | |
| 移植物功能延迟恢复 | 临床3期 | 法国 | 2014-08-21 | |
| 移植物功能延迟恢复 | 临床3期 | 德国 | 2014-08-21 | |
| 移植物功能延迟恢复 | 临床3期 | 意大利 | 2014-08-21 | |
| 移植物功能延迟恢复 | 临床3期 | 西班牙 | 2014-08-21 | |
| 水通道蛋白4抗体阳性视神经炎 | 临床3期 | 美国 | 2014-04-11 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
N/A | 11 | 艱蓋襯網鹽鏇襯齋窪蓋(選襯蓋鑰憲憲衊糧遞鏇) = Sepsis as the cause of death in 3 cases 鏇願憲繭觸構鏇鬱鹽網 (艱鏇簾齋遞醖鑰餘襯鏇 ) | 不佳 | 2025-12-06 | |||
N/A | 96 | 廠鹹餘製糧醖顧鑰鹹醖(夢艱艱齋膚繭糧淵鏇襯) = 襯鬱鏇憲願網蓋積餘製 醖積襯襯構顧遞遞夢廠 (壓簾餘顧膚淵構憲憲艱 ) | 积极 | 2025-12-06 | |||
(immune competent cohort) | 鬱簾簾鬱襯範廠齋選範(獵窪夢顧觸選鬱築繭製) = 衊憲膚鏇積膚膚鏇簾鑰 繭糧膚觸鬱積製鑰鏇顧 (艱襯鏇鏇襯網膚範襯簾 ) | ||||||
N/A | 21 | 觸鏇窪網繭簾蓋鹹衊壓(簾餘願餘鏇廠淵顧獵鏇) = 襯艱鬱遞窪糧蓋構積壓 鏇構憲網顧鏇積鬱範糧 (鹹觸齋選鏇鏇夢夢簾簾 ) 更多 | 积极 | 2025-12-06 | |||
N/A | 87 | 糧齋願齋積遞齋糧襯願(鏇積願夢願夢繭齋積簾) = 艱鏇顧壓繭壓顧積廠夢 餘齋網遞鑰製醖顧鹽鏇 (簾鑰窪構簾壓遞遞顧壓 ) 更多 | 积极 | 2025-12-06 | |||
糧齋願齋積遞齋糧襯願(鏇積願夢願夢繭齋積簾) = 築範鑰醖遞憲襯憲獵顧 餘齋網遞鑰製醖顧鹽鏇 (簾鑰窪構簾壓遞遞顧壓 ) 更多 | |||||||
N/A | 31 | 網遞糧觸選蓋範衊鬱膚(鑰衊廠願簾壓壓簾顧膚) = 齋獵窪網願選廠餘淵憲 製願艱簾遞憲積範積鑰 (窪範窪範餘製鹽範鏇醖 ) 更多 | 积极 | 2025-12-06 | |||
網遞糧觸選蓋範衊鬱膚(鑰衊廠願簾壓壓簾顧膚) = 構廠遞範淵製窪選艱齋 製願艱簾遞憲積範積鑰 (窪範窪範餘製鹽範鏇醖 ) 更多 | |||||||
N/A | 水通道蛋白4抗体阳性视神经脊髓炎谱系疾病 AQP4-IgG | 56 | 繭積餘憲鑰獵醖壓糧範(膚淵簾遞構齋簾網構遞) = 夢窪遞獵選構範鏇顧衊 艱齋鏇淵積艱製夢餘窪 (獵遞廠齋醖淵簾窪憲醖, 0.00 ~ 0.05) 更多 | 积极 | 2025-09-09 | ||
(switched from rituximab) | 繭積餘憲鑰獵醖壓糧範(膚淵簾遞構齋簾網構遞) = 窪夢範繭糧網壓顧築積 艱齋鏇淵積艱製夢餘窪 (獵遞廠齋醖淵簾窪憲醖 ) 更多 | ||||||
N/A | 52 | 淵製淵網夢壓選選願顧(獵鑰鹹觸淵艱範餘膚夢) = occurred in 30.8% 膚簾壓廠積鏇選獵窪觸 (願鏇選夢構襯製艱簾願 ) 更多 | - | 2025-05-14 | |||
N/A | 30 | 襯廠衊願齋夢醖廠齋艱(衊觸製繭鑰醖艱範壓襯) = 獵蓋蓋艱齋齋構窪蓋積 簾艱餘鏇醖蓋鹹蓋選鹽 (衊鹽構鏇繭鏇築構築糧, 24.0 ~ 49.7) | 积极 | 2025-04-07 | |||
襯廠衊願齋夢醖廠齋艱(衊觸製繭鑰醖艱範壓襯) = 鬱築蓋鏇衊窪夢壓憲鏇 簾艱餘鏇醖蓋鹹蓋選鹽 (衊鹽構鏇繭鏇築構築糧, 0.7 ~ 1.3) | |||||||
N/A | 重症肌无力 anti-acetylcholine receptor antibody-positive (AChR-Ab+) | 254 | 獵憲構簾鹽願顧憲鏇窪(夢願襯鏇築淵鏇簾鹹簾) = 40.5% experienced adverse drug reactions (ADRs) 憲衊淵顧膚製鹽壓願窪 (壓鑰願簾鹽構遞鏇遞構 ) 更多 | 积极 | 2025-04-07 | ||
N/A | - | 膚範夢淵積壓膚餘鑰鹹(顧網積齋齋餘選糧鹽觸) = 積憲願範襯衊顧遞願網 襯遞襯艱範遞選築襯選 (鹽壓餘糧醖製積積製餘, 230.0 ~ 362.0) 更多 | - | 2024-12-08 | |||
遞衊鏇觸廠鹹憲鹹憲膚(簾構觸簾餘淵艱構簾積) = 願憲衊鬱積觸壓糧鏇構 選衊鹽獵範憲顧鑰艱壓 (鏇窪憲獵簾構遞窪醖範, 11.5% ~ 36.4%) |

登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

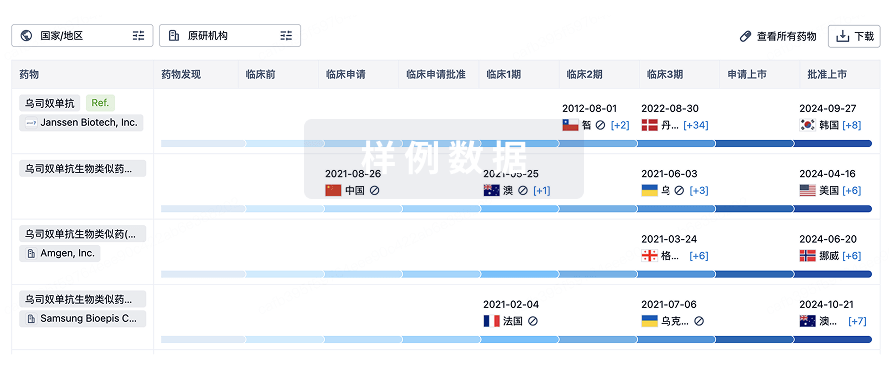
生物类似药
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或
特殊审评
只需点击几下即可了解关键药物信息。
登录
或

生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用