预约演示
更新于:2025-09-09

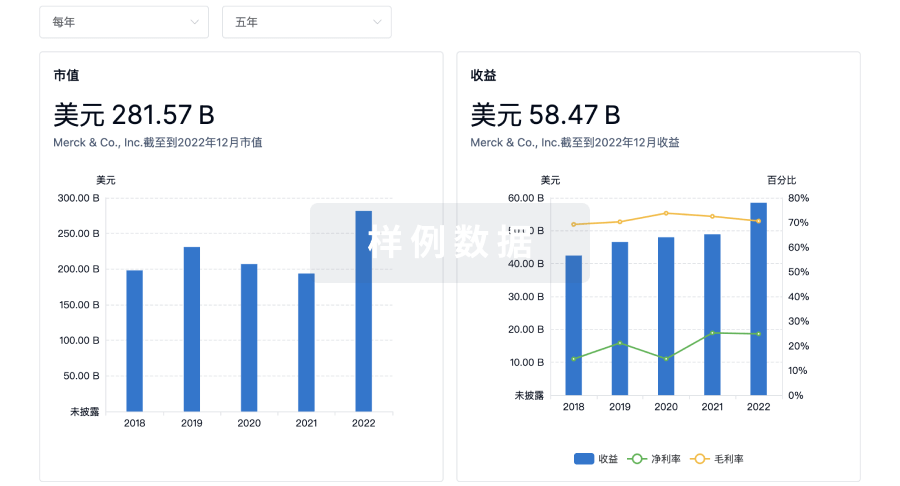
PTC Therapeutics, Inc.
更新于:2025-09-09
概览
标签
神经系统疾病
其他疾病
遗传病与畸形
小分子化药
腺相关病毒基因治疗
ASO
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
CTIS2023-506238-61-00
A Phase 3, Randomized, Crossover, Open-Label, Active-Controlled Study of Sepiapterin versus Sapropterin in Participants With Phenylketonuria =2 years of Age - PTC923-PKU-301
NCT06302348
A Phase 3b Open-Label Study of Long-Term Neurocognitive Outcomes in Children With Phenylketonuria Treated With Sepiapterin
ISRCTN79102999
A Phase III, randomized, crossover, open-label, active-controlled study of sepiapterin versus sapropterin in participants with phenylketonuria =2 years of age
100 项与 PTC Therapeutics, Inc. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-01-01Journal of Neuromuscular Diseases
In response to Gulcin Akinci’s and Haluk Topaloglu's letter regarding our article “Predictors of loss of ambulation in Duchenne muscular dystrophy: A systematic review and meta-analysis”
Letter
作者: Landfeldt, E ; Werner, C ; Kirschner, J ; Alemán, A ; Lochmüller, H ; Tomazos, I ; Ferizovic, N ; Zhang, R ; Abner, S
2025-01-01Genetic Testing and Molecular Biomarkers
REVEAL-CP: Selective Screening of Pediatric Patients for Aromatic L -Amino Acid Decarboxylase Deficiency with a Guthrie Card and In Silico Structural Modeling of One Index Case
Article
作者: Kuster, Alice ; Leuzzi, Vincenzo ; Liu, Emelline ; Amin, Sam ; Gowda, Vasantha ; Perduca, Massimiliano ; Strehle, Eugen-Matthias ; Bertoldi, Mariarita ; Battini, Roberta ; Johnson, Shelley ; Fox, Emily ; Lupo, Paul ; Werner, Christian
Background: The main objective of this prospective, multicenter study (REVEAL-CP) was to test children with cerebral palsy-like signs and symptoms for raised 3-O-methyldopa (3-OMD) blood levels, a biomarker for aromatic L-amino acid decarboxylase deficiency (AADCd). A secondary objective was to characterize the molecular basis for the defective aromatic L-amino acid decarboxylase (AADC) gene product. Methods: Patients were identified in pediatric secondary and tertiary care hospitals through database searches and personal communication. 3-OMD concentrations from Guthrie card tests were determined using liquid chromatography/mass spectrometry. If 3-OMD was raised, cerebrospinal fluid analysis and dopa decarboxylase (DDC) gene sequencing were performed. An in-silico mutagenesis analysis was carried out to model altered AADC enzymes. Results: In total, 166 patients were enrolled in this study. The median age was 8 years. Sixty-six patients (39.8%) had a diagnosis of cerebral palsy, with the most common type being "mixed" (n = 42; 25.3%). One patient (0.6%), an 11-month-old boy from Italy, was diagnosed with AADCd caused by a homozygous, pathogenic DDC variant (c.749C>T; p.Ser250Phe). Three-dimensional modeling of the Ser250Phe AADC enzyme variant revealed its destabilization. Conclusions: A Guthrie card test for 3-OMD is a recognized screening technique for AADCd. If universal newborn screening for this metabolic disease is not available, children with signs and symptoms of a movement disorder should be investigated for AADCd.
2024-10-01MOLECULAR THERAPY
Preclinical studies of gene replacement therapy for CDKL5 deficiency disorder
Article
作者: Narasimhan, Jana ; Wu, Michael C ; Cao, Liangxian ; Kim, Min Jung ; Wu, Zhijian ; Lee, Jeanee ; Southgate, Christopher ; Pear, Lisset ; Fotouh, Eman ; Pick, Joseph ; Voronin, Gregory ; Sheedy, Josephine ; Jung, Stephen ; Peters, Melinda ; DeMarco, Steven ; Saadipour, Khalil ; Varganov, Yakov ; Weetall, Marla ; Yalamanchili, Padmaja ; Sinha, Supriya ; Welch, Ellen M ; Lipari, Philip ; Gittens, Jamila ; Ray, Balmiki ; Mollin, Anna
Cyclin-dependent kinase-like 5 (CDKL5) deficiency disorder (CDD) is a rare neurodevelopmental disorder caused by a mutation in the X-linked CDKL5 gene. CDKL5 is a serine/threonine kinase that is critical for axon outgrowth and dendritic morphogenesis as well as synapse formation, maturation, and maintenance. This disorder is characterized by early-onset epilepsy, hypotonia, and failure to reach cognitive and motor developmental milestones. Because the disease is monogenic, delivery of the CDKL5 gene to the brain of patients should provide clinical benefit. To this end, we designed a gene therapy vector, adeno-associated virus (AAV)9.Syn.hCDKL5, in which human CDKL5 gene expression is driven by the synapsin promoter. In biodistribution studies conducted in mice, intracerebroventricular (i.c.v.) injection resulted in broader, more optimal biodistribution than did intra-cisterna magna (i.c.m.) delivery. AAV9.Syn.hCDKL5 treatment increased phosphorylation of EB2, a bona fide CDKL5 substrate, demonstrating biological activity in vivo. Our data provide proof of concept that i.c.v. delivery of AAV9.Syn.hCDKL5 to neonatal male Cdkl5 knockout mice reduces pathology and reduces aberrant behavior. Functional improvements were seen at doses of 3e11 to 5e11 vector genomes/g brain, which resulted in transfection of ≥50% of the neurons. Functional improvements were not seen at lower doses, suggesting a requirement for broad distribution for efficacy.
2025-09-02
临床结果上市批准临床3期临床2期疫苗
100 项与 PTC Therapeutics, Inc. 相关的药物交易
登录后查看更多信息
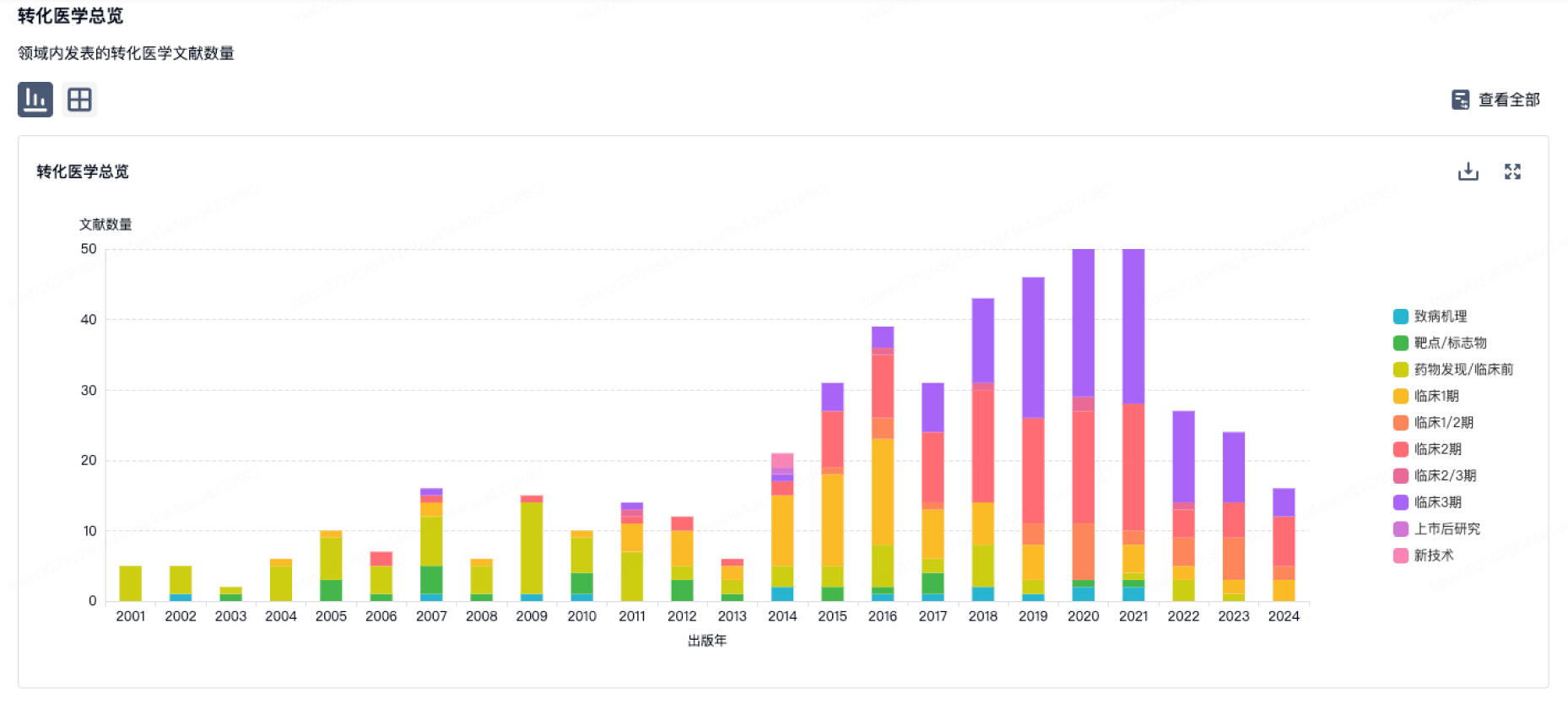
100 项与 PTC Therapeutics, Inc. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月30日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
药物发现
5
7
临床前
临床1期
3
1
临床2期
临床3期
1
4
批准上市
其他
16
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用