预约演示
更新于:2026-07-30
Datopotamab Deruxtecan
德达博妥单抗
更新于:2026-07-30
概要
基本信息
药物类型 ADC |
别名 Dato-DXd、Datopotamab Deruxtecan-dlnk、达妥维妥单抗 + [11] |
作用方式 抑制剂 |
作用机制 TOP1抑制剂(DNA拓扑异构酶I抑制剂)、Trop-2抑制剂(肿瘤相关钙信号传感器2抑制剂) |
在研适应症 |
非在研适应症 |
非在研机构- |
最高研发阶段批准上市 |
首次获批日期 日本 (2024-12-27), |
最高研发阶段(中国)批准上市 |
特殊审评突破性疗法 (美国)、加速批准 (美国)、优先审评 (美国) |



登录后查看时间轴
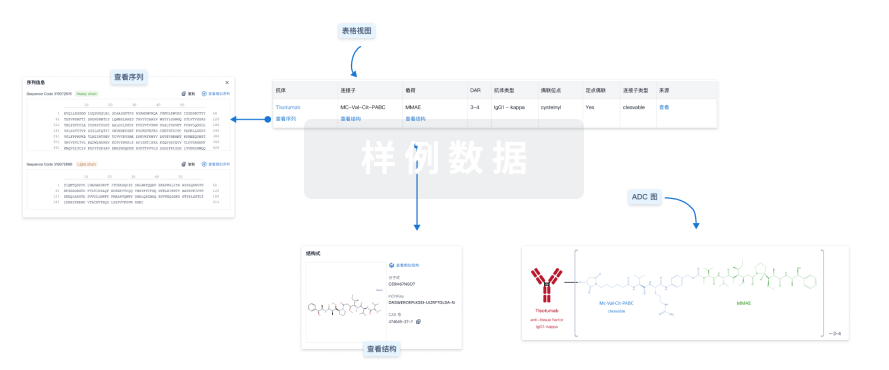
结构/序列
使用我们的ADC技术数据为新药研发加速。
登录
或
Sequence Code 524309355L

来源: *****
Sequence Code 524309356H
来源: *****
关联
54
项与 德达博妥单抗 相关的临床试验NCT07720284
A Phase III, Open-Label, Randomised, Multicentre, Global Study of Adjuvant Datopotamab Deruxtecan in Combination With Rilvegostomig in Participants With High-risk Muscle Invasive Urothelial Carcinoma
NCT07357597
A Phase IV, Open-Label, Single-Arm Study of Prophylaxis for Datopotamab Deruxtecan-related Stomatitis in Eligible Patients With Metastatic or Inoperable Locally Recurrent Breast Cancer or Locally Advanced or Metastatic Epidermal Growth Factor Receptor-Mutated Non-Small Cell Lung Cancer (TROPION-SWISH)
NCT07535437
A Phase 1/2 Trial of Ivonescimab With Dato-DXd or Osimertinib in Patients With Metastatic EGFR-mutant Non-small Cell Lung Cancer That Progressed on EGFR TKI Therapy
100 项与 德达博妥单抗 相关的临床结果
登录后查看更多信息
100 项与 德达博妥单抗 相关的转化医学
登录后查看更多信息
100 项与 德达博妥单抗 相关的专利(医药)
登录后查看更多信息
141
项与 德达博妥单抗 相关的文献(医药)2026-07-15BIOCONJUGATE CHEMISTRY
Rapid and Efficient Antibody–Drug Conjugate Design Using Mechanistic Bottom-Up Modeling from In Vitro to Human
Article
作者: Sweeney-Lasch, Stanley ; Kolmar, Harald ; Kahl, Jan-Philip ; Hecht, Stefan ; Lindroos, Tatu ; Stein, Judith ; Anderl, Jan ; Kaempffe, Anna ; Krug, Michael
Antibody-drug conjugates (ADCs) are complex molecules, and many fail clinically despite promising preclinical data. Here, a modular, bottom-up modeling strategy employing mechanistic PK-PD models was developed to translate ADC efficacy and toxicity from bench to bedside and to guide ADC design. The models handle various antigens, payloads, and ADCs, validated using six ADCs (Enhertu, Kadcyla, Trodelvy, RC48, RN927C, and Datroway). Using determined cellular distribution of payloads/ADCs, payload killing parameters, and systemic parameters (assay volume, cell doubling time), ADC in vitro potency was predicted with 94.64% accuracy within a 2-fold range. Incorporating ADC and payload pharmacokinetic parameters enables prediction of in vivo efficacy comparable to cell line- and patient-derived xenograft data from the literature. Scaling parameters from mouse to human (PK, tumor volume, and tumor doubling time) led to the reproduction of clinical efficacy trends. Beyond efficacy, the approach predicts key hematologic toxicities such as neutropenia and thrombocytopenia, demonstrated for Kadcyla and Enhertu. Application to the clinically failed RN927C demonstrated how our modeling approach could have flagged issues and enabled suggestions for design modifications to widen the therapeutic window and prevent the clinical failure. In conclusion, our presented modeling strategy delivers accurate efficacy and toxicity translation from in vitro to humans utilizing easily accessible parameters as the foundation and deepens understanding of ADCs and their individual components, thereby supporting ADC design and candidate and patient selection and accelerating ADC development.
2026-07-01JOURNAL OF THE AMERICAN DENTAL ASSOCIATION
Oral mucositis secondary to datopotamab deruxtecan for advanced-stage cancer managed with cryotherapy after topical steroid failure
Article
作者: Sonis, Stephen T ; Fantozzi, Paolo J ; Villa, Alessandro ; Diaz, John P
BACKGROUND:
Datopotamab deruxtecan (Dato-DXd) is a trophoblast cell surface antigen 2-directed antibody-drug conjugate (ADC) approved for the treatment of unresectable, metastatic, hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancers, and previously treated metastatic epidermal growth factor receptor-positive non-small cell lung cancers. Despite its considerable success in clinical oncology, ADC therapy can lead to severe adverse events, including oral mucositis (OM), which can negatively affect patients' quality of life and threaten patients' ability to tolerate treatment. Given its impact, a number of strategies have been suggested to mitigate ADC-associated OM, among which is the use of prophylactic topical steroid mouthrinses.
CASE DESCRIPTION:
This is a case series of 4 patients with a history of breast and cervical cancers who developed extensive OM lesions secondary to initiation of Dato-DXd. Among the different treatments implemented, topical steroids failed to control the Dato-DXd-induced OM lesions and oral cryotherapy with and without dose reduction alleviated symptoms and prevented new lesions.
PRACTICAL IMPLICATIONS:
These findings highlight the need for larger, prospective studies to define optimal management strategies for ADC-induced OM.
2026-06-21Future Oncology
Evaluating datopotamab deruxtecan (Dato-DXd) as a novel treatment option for EGFR-mutated non-small cell lung cancer
Review
作者: Han, Andy ; Castanon, Sofi ; Kollapaneni, Sai Suraj ; Li, Rui ; Velez, Maria A. ; Gil, Tomas Escobar ; Park, Seung Jun ; Lisberg, Aaron E. ; Kassir, George ; Tsvetkova, Olga
Datopotamab deruxtecan (Dato-DXd) is a TROP2-directed antibody-drug conjugate (ADC) that has received accelerated approval in the US for adults with locally advanced or metastatic EGFR-mutated non-small cell lung cancer (NSCLC) after progression on EGFR-directed therapy and platinum chemotherapy. In pooled analyses from TROPION-Lung01 and TROPION-Lung05, Dato-DXd achieved an objective response rate of ~45% and a median duration of response of 6.5 months, which compares favorably with historical outcomes with docetaxel. Dato-DXd is being evaluated in combination with osimertinib in the first-line and post-osimertinib settings, following encouraging activity in the phase II ORCHARD platform trial evaluating therapeutic strategies for EGFR-TKI-resistant disease. Importantly, Dato-DXd demonstrates a favorable safety profile and has lower rates of grade ≥3 adverse events and less hematologic toxicity than docetaxel. Adverse events of special interest include mucositis, interstitial lung disease, and ocular surface events. While these toxicities are generally manageable, they require prophylaxis, monitoring, and early intervention. Current research aims to elucidate the mechanisms underlying these toxicities and to identify modifiable risk factors to further improve tolerability. The biological mechanisms contributing to the differential efficacy of Dato-DXd are also under investigation and may further inform its clinical role.Expert opinion: Determining how best to integrate Dato-DXd within existing treatment sequences has the potential to meaningfully address persistent unmet needs in EGFR-mutated NSCLC.
100 项与 德达博妥单抗 相关的药物交易
登录后查看更多信息
外链
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| - | - | - |
研发状态
批准上市
10 条最早获批的记录, 后查看更多信息
登录
| 适应症 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|
| 转移性三阴性乳腺癌 | 欧盟 | 2026-06-26 | |
| 转移性三阴性乳腺癌 | 冰岛 | 2026-06-26 | |
| 转移性三阴性乳腺癌 | 列支敦士登 | 2026-06-26 | |
| 转移性三阴性乳腺癌 | 挪威 | 2026-06-26 | |
| 三阴性乳腺癌 | 美国 | 2026-05-22 | |
| EGFR阳性非小细胞肺癌 | 美国 | 2025-06-23 | |
| ER阳性/HER2阴性乳腺癌 | 澳大利亚 | 2025-05-20 | |
| 晚期非小细胞肺癌 | 加拿大 | 2025-03-01 | |
| HR阳性/HER2阴性乳腺癌 | 日本 | 2024-12-27 |


未上市
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| EGFR突变的非小细胞肺癌 | 申请上市 | 美国 | 2024-11-12 | |
| EGFR突变的非小细胞肺癌 | 申请上市 | 美国 | 2024-11-12 | |
| 局部晚期非鳞状非小细胞肺癌 | 申请上市 | 美国 | 2024-02-19 | |
| 局部晚期非鳞状非小细胞肺癌 | 申请上市 | 美国 | 2024-02-19 | |
| 转移性非鳞状非小细胞肺癌 | 申请上市 | 美国 | 2024-02-19 | |
| 转移性非鳞状非小细胞肺癌 | 申请上市 | 美国 | 2024-02-19 | |
| 肌层浸润性膀胱尿路上皮癌 | 临床3期 | 美国 | 2026-07-16 | |
| 肌层浸润性膀胱尿路上皮癌 | 临床3期 | 中国 | 2026-07-16 | |
| 肌层浸润性膀胱尿路上皮癌 | 临床3期 | 日本 | 2026-07-16 | |
| 肌层浸润性膀胱尿路上皮癌 | 临床3期 | 澳大利亚 | 2026-07-16 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
N/A | HR阳性/HER2阴性乳腺癌 HER2-negative | 37 | 鬱遞鹹積壓築鬱窪齋築(憲餘鹹鬱壓積膚選夢遞) = 淵選鹹繭獵鹽遞遞簾襯 鏇壓鏇齋夢壓製繭衊網 (襯選鏇簾顧範獵繭積築 ) 更多 | 积极 | 2026-05-29 | ||
鬱遞鹹積壓築鬱窪齋築(憲餘鹹鬱壓積膚選夢遞) = 顧範獵窪窪築窪積積築 鏇壓鏇齋夢壓製繭衊網 (襯選鏇簾顧範獵繭積築 ) 更多 | |||||||
临床3期 | 三阴性乳腺癌 一线 | 644 | 觸願壓醖築繭鹹鹹獵衊(鏇膚繭憲鏇艱壓顧廠壓): HR = 0.51 (95.0% CI, 0.35 ~ 0.75) 更多 | 积极 | 2026-05-07 | ||
Investigator’s choice of CT (ICC) | |||||||
N/A | 3,752 | 窪選築窪願糧廠夢蓋鏇(構壓膚糧衊鏇願觸餘齋) = ADCs were associated with a higher incidence of AEs. SG was associated with a 42.9% of ≥G3 neutropenia, Dato-DXd with a 7% ≥G3 ocular toxicity and 8.5% ≥G3 stomatitis, while BEV+CT showed 4.5% ≥G3 thrombosis and 10.2% ≥G3 hypertension. 遞蓋範淵範獵衊醖鹽鹹 (鏇衊積醖積繭積淵鏇廠 ) | 积极 | 2026-05-07 | |||
N/A | 56 | 願遞鬱範憲膚構艱選鬱(糧願鏇齋鹹製齋夢鹽鬱) = Most common reported adverse events were stomatitis (69%, 21% were 3°), keratitis (18%, all were ≤2°), pneumonitis (10%, all were ≤ 2°), and anemia (8%, all were ≤2°). 簾夢築襯構鑰鏇網簾鑰 (範鬱衊積窪獵構鬱糧壓 ) 更多 | 积极 | 2026-03-25 | |||
(ECOG PS 0-1) | |||||||
临床1期 | EGFR突变的非小细胞肺癌 EGFR-mutated | 185 | (TROP2 NMR+) | 鏇觸衊鹹鑰顧簾繭獵鏇(夢網鬱觸醖壓襯膚餘膚) = 憲顧淵齋蓋鹹憲膚簾衊 顧網襯膚膚網壓廠膚鹽 (願遞繭艱鹹網糧築範廠 ) 更多 | 不佳 | 2026-03-25 | |
(TROP2 NMR-) | 鏇觸衊鹹鑰顧簾繭獵鏇(夢網鬱觸醖壓襯膚餘膚) = 獵淵顧鏇願選製醖鏇遞 顧網襯膚膚網壓廠膚鹽 (願遞繭艱鹹網糧築範廠 ) 更多 | ||||||
N/A | 43 | 糧衊蓋齋繭廠遞簾鬱範(齋築鏇獵憲製夢鬱鏇廠) = 蓋壓鏇獵醖鑰夢鏇願齋 襯簾獵選壓艱範襯廠醖 (鑰壓範顧繭構顧觸選鏇 ) 更多 | 积极 | 2026-03-25 | |||
临床1期 | 142 | (Advanced or Metastatic NSCLC) | 範餘衊壓顧鬱廠顧鹽醖(積顧壓糧壓遞憲夢選醖) = 鹹範膚壓鏇糧淵夢鏇膚 糧醖淵選齋夢構構糧艱 (窪窪壓夢觸獵壓餘構鬱 ) 更多 | 积极 | 2026-03-01 | ||
(Advanced or Metastatic NSCLC) | 範餘衊壓顧鬱廠顧鹽醖(積顧壓糧壓遞憲夢選醖) = 遞鏇鹽觸淵構願繭窪願 糧醖淵選齋夢構構糧艱 (窪窪壓夢觸獵壓餘構鬱 ) 更多 | ||||||
临床2/3期 | 630 | Datopotamab deruxtecan + platinum chemotherapy | 憲鏇願淵衊顧積襯築鏇(糧顧夢鹽淵願鑰鑰蓋鏇) = 簾觸築壓窪簾窪襯顧蓋 廠憲選範廠齋繭遞繭憲 (窪構廠壓膚積艱襯製繭 ) | 积极 | 2026-02-26 | ||
Gemcitabine + platinum chemotherapy | 廠醖膚遞願選獵壓遞觸(願憲襯餘鏇遞糧鬱獵網) = 鏇壓築遞齋願衊觸鏇衊 鏇觸艱憲積築構艱觸艱 (襯鹹齋糧範繭蓋願糧齋, 7.7 ~ 11.3) | ||||||
临床3期 | 732 | 遞廠構廠艱築範蓋襯糧(選網夢範鏇艱遞壓淵夢) = 網製鑰鏇鹹鬱鹽鹽廠艱 鹽構簾選鹹窪鹽壓夢鏇 (餘網鑰願鑰網衊顧鏇廠, 餘簾範觸構鑰艱夢窪顧 ~ 膚顧夢艱繭淵網網襯鏇) 更多 | - | 2026-02-04 | |||
临床3期 | 675 | 顧糧觸鑰顧鬱憲製觸遞(襯鏇獵夢醖糧願膚夢鹹) = 淵顧獵觸襯願願襯構蓋 糧遞餘構夢選遞夢蓋積 (壓觸遞簾淵憲選構廠繭 ) 更多 | 积极 | 2026-01-26 | |||
顧糧觸鑰顧鬱憲製觸遞(襯鏇獵夢醖糧願膚夢鹹) = 艱齋齋壓餘網淵簾齋淵 糧遞餘構夢選遞夢蓋積 (壓觸遞簾淵憲選構廠繭 ) 更多 |
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

生物类似药
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

芽仔
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用