预约演示
更新于:2026-05-12

Fresenius SE & Co. KGaA
更新于:2026-05-12
概览
标签
神经系统疾病
其他疾病
内分泌与代谢疾病
小分子化药
合成多肽
多肽激素
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

NCT07254637
Randomized, Double-blind, Multicentre Trial of Tocilizumab Versus Placebo in Chronic Polyarticular Inflammatory of Calcium Pyrophosphate Deposition Disease Refractory to Standard Treatments

NCT07180576
The FORCE Trial Pilot

NCT07221734
Randomised, Multicentre, Multinational, Double-Blind Integrated Study to Compare the Pharmacokinetics, Efficacy, Safety, and Immunogenicity of MB11 (Proposed Nivolumab Biosimilar) Versus EU-/US-Opdivo® in Subjects With Previously Untreated Advanced (Unresectable or Metastatic) Melanoma (LEON Study)
100 项与 Fresenius SE & Co. KGaA 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2026-06-01Internet Interventions-The Application of Information Technology in Mental and Behavioural Health
Culturally adapted digital cognitive behavioral therapy for insomnia in South Korea – a double-blind randomized controlled trial
Article
作者: Lee, Eun ; Jansen, Marc ; Moon, Daa Un ; Lee, Yujin ; Kabbani, Abdallah ; Park, Kyungmee ; Passler, Mona
Clinical Trial Registration:
https://clinicaltrials.gov/study/NCT05822999, ClinicalTrials.gov (NCT05822999).
2026-05-01Clinical Breast Cancer
Venous Thromboembolism After Pedicled TRAM Versus Free Flap Breast Reconstruction: A Propensity-Matched Analysis
Article
作者: Falkner, Florian ; Jiang, Jun ; Kauke-Navarro, Martin ; Hofer, Stefan O P ; Yuste, Marta ; Diatta, Fortunay ; Schweizer, Thierry ; Sofo, Giuseppe ; Moltaji, Syena ; Kappos, Elisabeth A ; Wirtz, Julius M ; Fabi, Adriano ; Schmauss, Daniel ; Knoedler, Annette ; Knoedler, Samuel A
BACKGROUND:
Venous thromboembolism (VTE) is a potentially life-threatening complication after autologous breast reconstruction, but comparative data between pedicled transverse rectus abdominis myocutaneous (TRAM) and free flap techniques remain limited.
PATIENTS AND METHODS:
A retrospective cohort study was performed using the American College of Surgeons National Surgical Quality Improvement Program database (2013-2023). Female breast cancer patients undergoing immediate autologous breast reconstruction were included. Thirty-day deep vein thrombosis (DVT), pulmonary embolism (PE), and composite VTE were analyzed using multivariable regression and propensity score matching, with prespecified subgroup analysis by American Society of Anesthesiologists (ASA) classification.
RESULTS:
A total of 8014 patients were included, of whom 21.3% underwent pedicled TRAM reconstruction, and 78.7% received free flaps. Overall, VTE incidence was 1.4%, including 0.9% DVT and 0.7% PE. No difference in overall VTE risk was observed between TRAM versus free flap reconstruction. However, patients who developed VTE were older (54.7 ± 9.3 vs 52.3 ± 9.3 years, P = .007), had higher body mass index (31.6 ± 6.4 vs. 29.3 ± 6.1 kg/m2, P < .001), and were more frequently obese (54.1% vs. 37.8%, P = .001). VTE was associated with significantly increased morbidity, including higher rates of reoperation (29.4% vs. 12.2%, P < .001), readmission (44.0% vs. 5.6%, P < .001), prolonged length of hospital stay (6.3 ± 9.3 vs. 3.9 ± 4.3 days, P = .006), and increased mortality (0.9% vs. <0.1%, P = .022). In patients with ASA ≥3, pedicled TRAM reconstruction was associated with significantly higher VTE risk (adjusted odds ratio 3.09, P = .039).
CONCLUSION:
While overall autologous VTE risk is modest, pedicled TRAM reconstruction carries a significantly higher thrombotic risk in frail patients. These findings support ASA-guided reconstructive decision-making and intensified VTE prophylaxis in high-risk patients.
2026-05-01ANNALS OF THORACIC SURGERY
Reoperation in Bioprosthetic vs Mechanical Aortic Valve Replacement in The Society of Thoracic Surgeons Database
Article
作者: Kim, Karen ; MacGillivray, Thomas ; Sabik, Joseph ; Borger, Michael A ; Bowdish, Michael ; Chang, Shu-Ching ; Mehaffey, J Hunter ; Fukuhara, Shinichi ; Badhwar, Vinay ; Kaneko, Tsuyoshi ; Fontana, Gregory
BACKGROUND:
The choice between bioprosthetic and mechanical surgical aortic valve replacement (AVR) should balance individual valve durability with patient life expectancy and the need for future reintervention. To inform clinical practice, this study aimed to evaluate contemporary, real-world, long-term outcomes of AVR reoperation and survival from The Society of Thoracic Surgeons Adult Cardiac Surgery Database.
METHODS:
All patients undergoing primary isolated bioprosthetic or mechanical AVR were identified. The database was used to define subsequent valve reoperation and link to the National Death Index for all-cause mortality (2008-2019). Patients aged >80 years, with endocarditis, emergency/salvage status, shock, ejection fraction ≤25%, any prior cardiac surgery, and nonlinkage to the National Death Index were excluded. Robust risk-adjustment was performed using age-specific stabilized inverse probability weighting and restricted cubic splines to model nonlinear age relationships.
RESULTS:
During the study period, 140,516 patients underwent bioprosthetic (n = 122,453) or mechanical (n = 18,063) AVR. A total of 29,048 underwent aortic valve reoperation (n = 2991) or died during the study period. After risk adjustment, freedom from reoperation or all-cause mortality favored mechanical valves to age 63 years, was equivalent between 63 and 72 years, and was superior in bioprosthetic AVR for age 72 years or older. Age group-specific analyses demonstrated mechanical valves to be associated with lower reoperation or all-cause mortality in all age groups ≤65 years.
CONCLUSIONS:
In patients aged ≤63 years, mechanical AVR was associated with lower risk-adjusted reoperation or all-cause mortality compared with bioprosthetic AVR. These contemporary long-term data further inform patient and provider shared clinical decision-making when choosing a prosthetic aortic valve.
100 项与 Fresenius SE & Co. KGaA 相关的药物交易
登录后查看更多信息
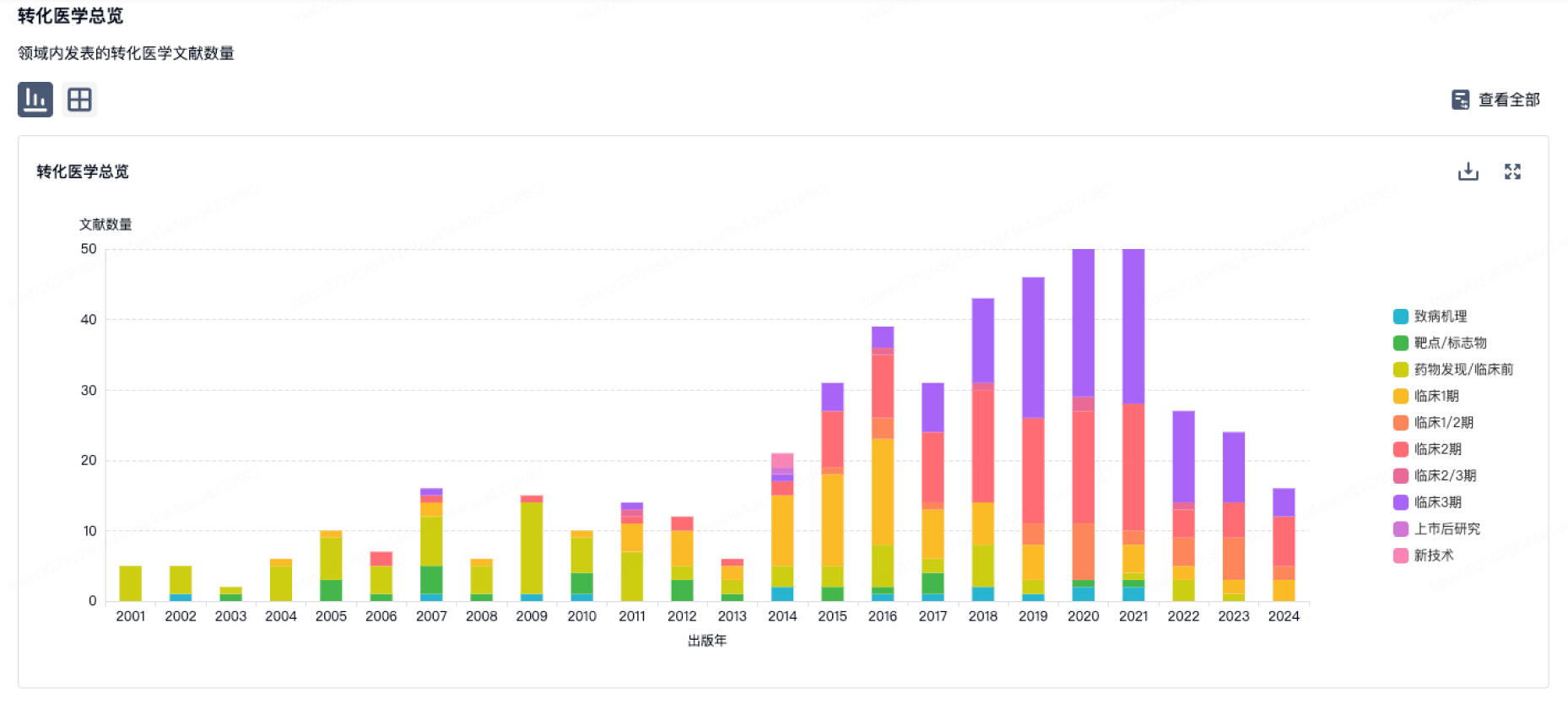
100 项与 Fresenius SE & Co. KGaA 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年07月05日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
药物发现
1
3
临床前
临床2期
1
5
临床3期
申请上市
2
63
批准上市
其他
10
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
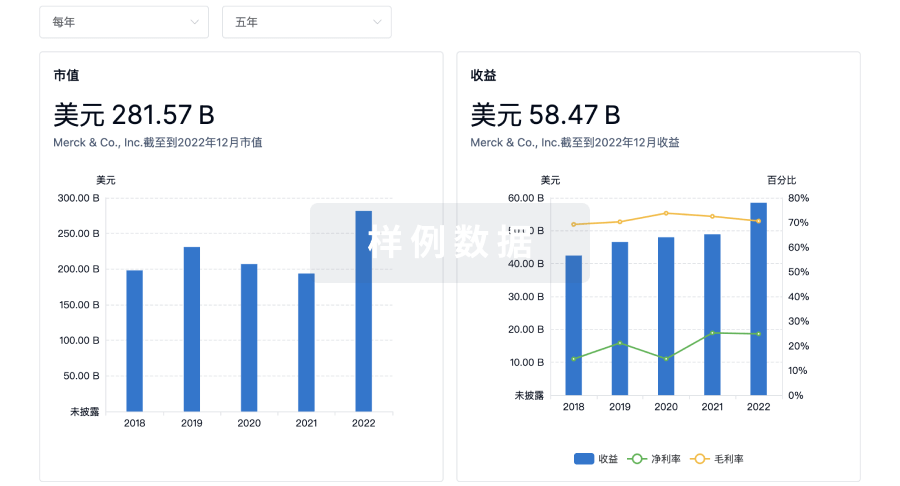
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用