预约演示
更新于:2026-05-21
Novartis AG
更新于:2026-05-21
概览
标签
肿瘤
神经系统疾病
其他疾病
小分子化药
单克隆抗体
非降解型分子胶
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
NCT07421167
A Phase 2 Open-label Study to Evaluate the Tolerability of Ianalumab (VAY736) With Investigator's Choice Thrombopoietin Receptor Agonist (IC TPO-RA) in Patients With Primary Immune Thrombocytopenia (ITP) Previously Treated With at Least One Treatment (VAY2EXPLORE)
NCT07431931
Optimizing Referral Pathways for Patients With Hematuria and Moderate-Severe Proteinuria - Phase 2: A Quality Improvement Project

NCT07498335
A Single-arm, Multicenter, Phase III Study to Assess Efficacy, Pharmacokinetics, Safety and Tolerability of Atrasentan in Pediatric Patients of 2 to <18 Years of Age With Primary Immunoglobulin A Nephropathy (IgAN)
100 项与 Novartis AG 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2026-07-01INTERNATIONAL JOURNAL OF CANCER
Real‐world progression‐free survival and overall survival in patients with
HR
+
/
HER2
−
advanced breast cancer treated in first‐line with ribociclib, endocrine monotherapy or chemotherapy: Results from the observational
RIBANNA
study
Article
作者: Frederik Marmé ; Christina Pfister ; Thomas Decker ; Rudolf Weide ; Kerstin Lüdtke-Heckenkamp ; Anne Engel ; Achim Wöckel ; Cosima Brucker ; Jan Janssen ; Thomas Göhler ; Christian Roos ; Pauline Wimberger ; Peter A. Fasching ; Elena Kisseleff ; Christian Jackisch ; Beate Rautenberg ; Marcus Schmidt ; Claudia Quiering ; Marion van Mackelenbergh ; Andreas Köhler ; Diana Lüftner
Abstract:
Cyclin‐dependent kinase 4 and 6 inhibitors (CDK4/6i) combined with endocrine therapy are the preferred choice for first‐line treatment of patients with HR
+
/HER2
−
locally advanced/metastatic breast cancer (aBC). The CDK4/6i ribociclib in combination with an aromatase inhibitor (AI) or fulvestrant (FUL) has demonstrated significant progression‐free survival (PFS) and overall survival (OS) benefits for pre‐ and postmenopausal aBC patients who were enrolled in the three pivotal MONALEESA trials. Following the initial approval of ribociclib in 2017, the non‐interventional RIBANNA study was initiated to evaluate the effectiveness and safety of ribociclib plus AI/FUL therapy among patients with aBC in a real‐world setting. Two additional treatment cohorts (endocrine monotherapy [ET] and chemotherapy [CT]) were included to extend the knowledge about current aBC treatments. A total of 2567 patients were enrolled in 279 study centers, of whom 1852 were treated with ribociclib+AI/FUL, 183 were treated with ET, and 139 were treated with CT, who were available for effectiveness analyses. Median PFS (mPFS) and median OS (mOS) on first‐line treatment with ribociclib+AI/FUL were 35.0 and 76.0 months, respectively. Adjustment for differences in demographic and baseline characteristics resulted in a longer mPFS on ribociclib+AI/FUL (34.7 months) compared to ET (26.4 months) or CT (19.2 months). Adverse events (AEs) on ribociclib were consistent with those seen in the pivotal trials, and no new safety signals were observed. The RIBANNA study confirmed the PFS and OS benefit seen in the MONALEESA trials. Together with the safety data, this large real‐world dataset supports the favorable risk/benefit profile of ribociclib in large scale patient populations.
2026-06-01JOURNAL OF PHARMACEUTICAL SCIENCES
Industry guidance on container closure integrity strategies for difficult-to-test parenteral products (DTPs)
Review
作者: Hebting, Henri ; Mudumala, Prudvi Raj ; Steffen, Jean-Sebastien ; Mayer, Tobias ; Spreng, Ben ; Wuchner, Klaus ; Huon, Carine ; Rass, Sophia ; Kuhn, Sebastian M ; Neuhold, Karen ; Riesop, David
Innovative modalities, such as antibody-drug conjugates (ADCs), radiopharmaceuticals (RPhs), and cell and gene therapies (CGTs), along with ultrahigh-concentration monoclonal antibody suspensions or high-concentration parenteral products, present unique container closure integrity (CCI) challenges because of toxicity, biohazard or radioactivity, very small batch sizes, high cost, fragility, or requirements for ultralow (<-70 °C) and cryogenic (<-150 °C) storage. These "difficult-to-test" parenteral products (DTPs) demand a tailored, lifecycle-based CCI strategy. Industry experts propose a holistic approach that decouples CCI assurance from constraints imposed by scarce or hazardous drug product (DP) and by final-presentation testing limits. By leveraging surrogate-filled or empty container closure systems (CCSs), sensitive CCIT methods can be applied without consuming valuable DP, preserving safety, operational feasibility, and regulatory compliance across development and commercial stages. To illustrate the approach, we consider a representative DP case i.e., a small-volume (0.5 mL) aqueous gene-therapy example filled into 2 mL plastic vials with rubber closures and aluminum crimps, stored long-term at <-70 °C and produced in batches of ∼200-500 units. Additionally, key CCIT method considerations for DTPs are summarized.
2026-05-01PHARMACOLOGICAL REVIEWS
Adhesion G protein-coupled receptors
Review
作者: Placantonakis, Dimitris G ; Piao, Xianhua ; Linnert, Joshua ; Chung, Yin Kwan ; Skiniotis, Georgios ; Melkumyan, Mariam ; Zaidman, Nathan A ; Favara, David M ; Gloriam, David E ; Georgiadi, Anastasia ; Vanhollebeke, Benoit ; Garcia De Las Bayonas, Alain ; Wolfrum, Uwe ; Zou, Yimin ; Spiess, Katja ; Sabbagh, Laurent ; Javitch, Jonathan A ; de Araujo Farias, Virginea ; Selcho, Mareike ; Schöneberg, Torsten ; Tall, Gregory G ; Martinelli, David C ; Aust, Gabriela ; Ludwig, Marie-Gabrielle ; Berndt, Sandra ; Formstone, Caroline J ; Rosenkilde, Mette M ; Seufert, Florian ; Kleinau, Gunnar ; Vallon, Mario ; Hildebrand, Peter W ; Hsiao, Cheng-Chih ; Tilley, Douglas G ; Bridges, James P ; Van Meir, Erwin G ; Engel, Felix B ; Liebscher, Ines ; Matúš, Daniel ; Südhof, Thomas C ; Caron, Kathleen M ; Mulder, Jan ; Hamann, Jörg ; Pederick, Daniel T ; Strutt, David ; Boucard, Antony A ; Sträter, Norbert ; Lin, Hsi-Hsien ; Scholz, Nicole ; Leduc, Richard ; Yan, Jie ; Duman, Joseph G ; Moreno-Salinas, Ana L ; Kittel, Robert J ; Mathiasen, Signe ; Prömel, Simone ; Blacklow, Stephen C ; Nash, Michael A ; Sun, Jinpeng ; Ping, Yu-Qi ; Singh, Abhishek K ; Avila-Zozaya, Monserrat ; Anderson, Garret R ; Blanco-Redondo, Beatriz ; Sando, Richard C ; Fu, Chaoyu ; Pal, Kasturi ; Bagger, Sofie Morsing ; Seiradake, Elena ; Araç, Demet ; Wiggin, Giselle R ; Langenhan, Tobias ; Scheerer, Patrick ; Brodmerkel, Lara-Sophie ; Hall, Randy A ; Dates, Andrew N ; Pohl, Fabian ; Huang, Bill X ; Kim, Hee-Yong ; Tolias, Kimberley F ; Thor, Doreen ; Del Toro, Daniel ; Perry-Hauser, Nicole A ; Barth, Patrick
Adhesion G protein-coupled receptors (aGPCRs) constitute a structurally and functionally distinct group within the superfamily of GPCRs. In 2015, the International Union of Pharmacology invited the Adhesion GPCR Consortium to publish a comprehensive review about aGPCRs and establish a unified nomenclature. Since then, substantial progress has been made in delineating the biological roles, molecular architecture, biochemical properties, expression profiles, ligand repertoire, and activation and signaling strategies of aGPCRs. Commensurate with these advances, their relevance to human pathophysiology has become increasingly apparent. In a coordinated effort, the Adhesion GPCR Consortium has reviewed recent progress in this field and provides a comprehensive assessment of the current understanding of aGPCR biology, including a focus on human and mammalian aGPCRs, their evolutionary origins, methodological approaches, and model systems for their investigation, as well as emerging approaches for their therapeutic targeting. SIGNIFICANCE STATEMENT: Adhesion G protein-coupled receptors are versatile cell-surface proteins that integrate structural, biochemical, and physiological functions, with major roles in health and disease. This review summarizes current knowledge of their molecular features, functions in diverse model systems, and emerging opportunities for therapeutic targeting, providing a comprehensive resource that connects basic biology with translational applications across multiple scientific disciplines.
2026-05-21
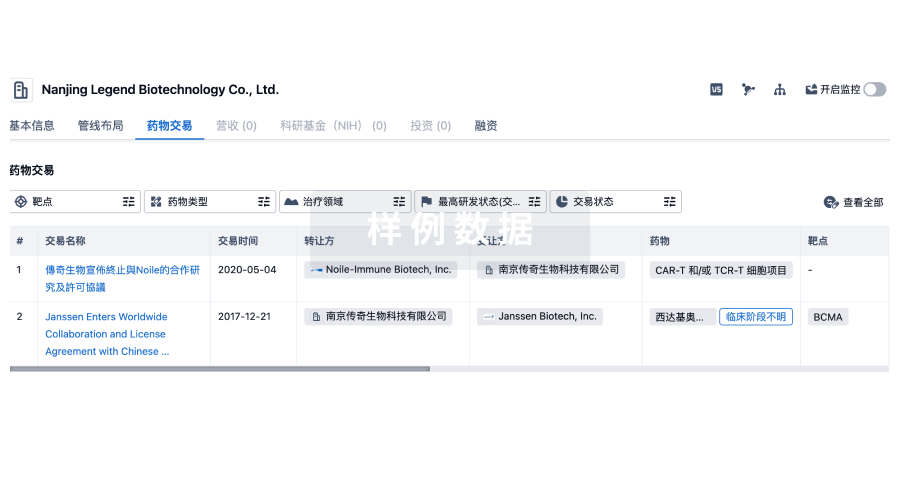
100 项与 Novartis AG 相关的药物交易
登录后查看更多信息
100 项与 Novartis AG 相关的转化医学
登录后查看更多信息
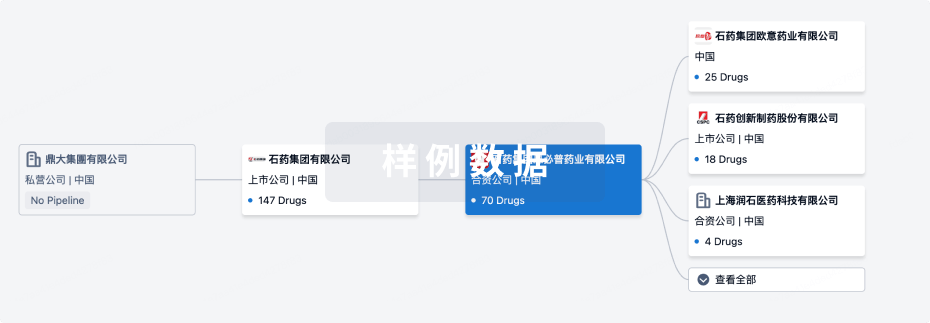
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年06月09日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
药物发现
42
153
临床前
临床申请批准
1
51
临床1期
临床2期
70
17
临床3期
申请上市
1
118
批准上市
其他
1041
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
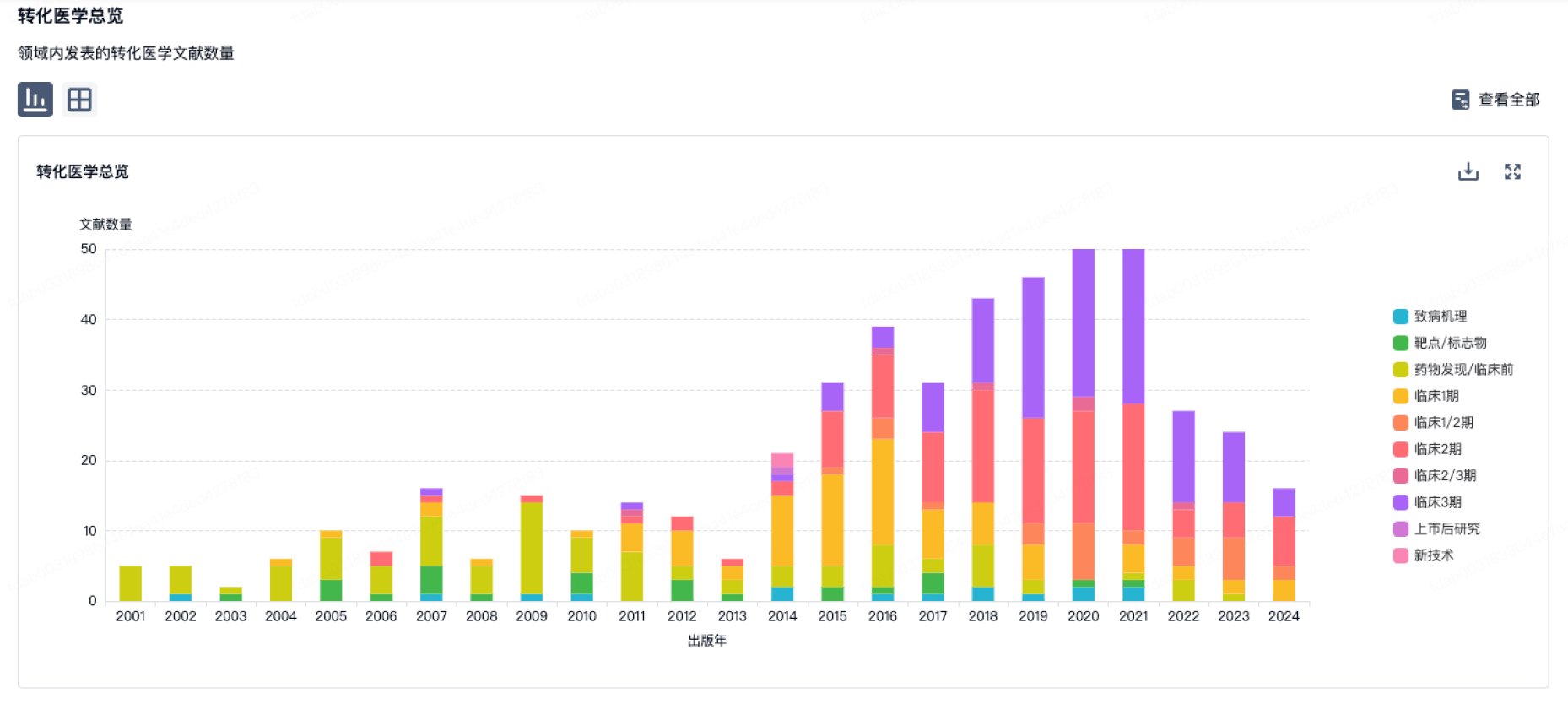
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
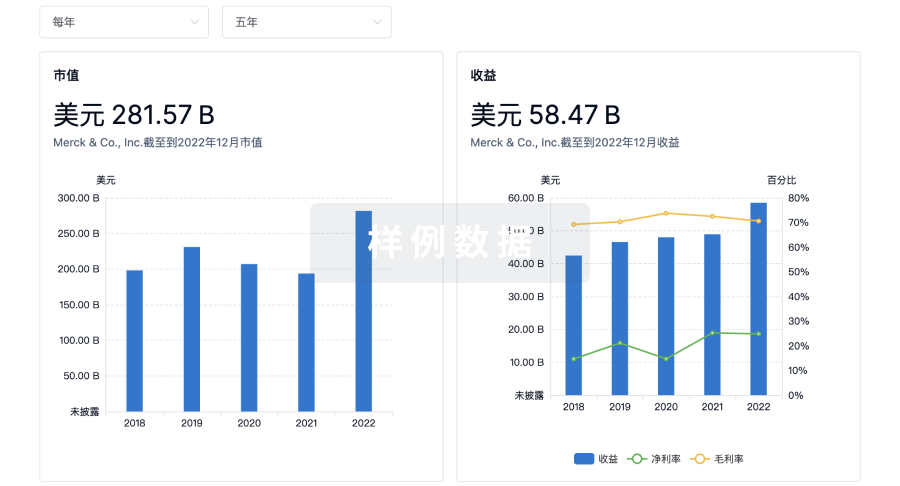
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用