预约演示
更新于:2026-08-06
Fam-trastuzumab deruxtecan-NXKI
德曲妥珠单抗
更新于:2026-08-06
概要
基本信息
药物类型 ADC |
别名 Fam-trastuzumab deruxtecan、T-DXd、Trastuzumab deruxtecan + [15] |
作用方式 拮抗剂、抑制剂 |
作用机制 HER2拮抗剂(受体蛋白酪氨酸激酶 erbB-2拮抗剂)、TOP1抑制剂(DNA拓扑异构酶I抑制剂)、ADCC(抗体依赖的细胞毒作用) |
在研适应症 |
非在研适应症 |
非在研机构- |
最高研发阶段批准上市 |
首次获批日期 美国 (2019-12-20), |
最高研发阶段(中国)批准上市 |
特殊审评突破性疗法 (美国)、快速通道 (美国)、加速批准 (美国)、孤儿药 (美国)、附条件批准 (中国)、孤儿药 (日本)、孤儿药 (澳大利亚)、优先审评 (澳大利亚)、突破性疗法 (中国)、优先审评 (美国)、优先审评 (中国)、先驱策略 (日本) |



登录后查看时间轴
结构/序列
使用我们的ADC技术数据为新药研发加速。
登录
或
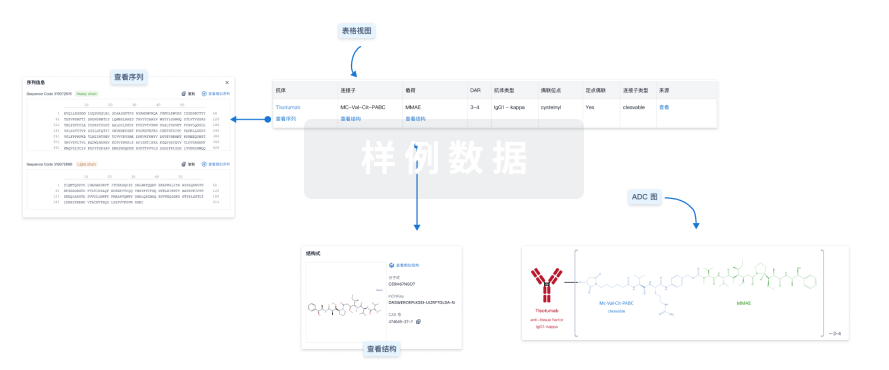
Sequence Code 18481L

来源: *****
Sequence Code 44772H
来源: *****
关联
205
项与 德曲妥珠单抗 相关的临床试验NCT07578116
Randomized Phase III Trial of Multimodality Therapy Versus Standard of Care Systemic Therapy in HER2 Positive (HER2+) De Novo (AJCC Stage IV) Oligometastatic Breast Cancer With Response to Initial Chemotherapy
NCT07126561
Phase II Open Label Trial of Trastuzumab Deruxtecan (Enhertu, DS-8210) in HER2 Positive Newly Diagnosed Metastatic Esophageal, Gastric, GEJ Cancer Patients With an ECOG Performance Status of 2

NCT07137416
Phase 1b Study of Pidnarulex and Trastuzumab Deruxtecan in Patients With HER2 Expressing Solid Tumors

100 项与 德曲妥珠单抗 相关的临床结果
登录后查看更多信息
100 项与 德曲妥珠单抗 相关的转化医学
登录后查看更多信息
100 项与 德曲妥珠单抗 相关的专利(医药)
登录后查看更多信息
1,164
项与 德曲妥珠单抗 相关的文献(医药)2026-10-01EUROPEAN JOURNAL OF MEDICINAL CHEMISTRY
An intrinsically hydrophilic linker enables a stable, high-DAR exatecan-based HER2 ADC with potent antitumor activity
Article
作者: Feng, Chaoyang ; Ma, Jianglei ; Wu, Chenglong ; Bao, Yiwen ; Huang, Jinkun ; Heng, Xiaojie ; Zeng, Nan ; Yang, Tingting ; Ni, Dechun
Antibody-drug conjugates (ADCs) combine the targeting specificity of monoclonal antibodies with the potent cytotoxicity of small-molecule drugs. However, ADC development using Exatecan, a potent topoisomerase I inhibitor, has been challenged by its hydrophobicity, leading to aggregation, rapid clearance, and off-target toxicity. Herein, we report the design of an intrinsically hydrophilic drug-linker platform (SMP-70067-L) that enables the construction of a homogeneous Exatecan-based HER2-targeted ADC (SMP-70067-X) with a high drug-to-antibody ratio (DAR of 7.92). Similar to Trastuzumab deruxtecan (DS-8201a), which achieves high DAR without PEG or polysarcosine chains through a hydrophilic self-immolative spacer, SMP-70067-L integrates minimal hydrophilic elements, including a glutamic acid residue and a modified aromatic self-immolative spacer, to balance hydrophilicity, stability, and efficient payload release. The resulting ADC exhibits low aggregation (<1%), favorable plasma and thermal stability, and sustained exatecan release. SMP-70067-X demonstrates potent cytotoxicity in HER2-positive tumor cells (sub-nanomolar IC50 values) and significantly enhanced antitumor efficacy compared to DS-8201a in HER2-moderate and HER2-low xenograft models. These results highlight the critical role of rational linker engineering in expanding the therapeutic window of hydrophobic topoisomerase I inhibitor-based ADCs.
2026-09-01SLAS Discovery
ADCs for colorectal carcinoma: decoding clinical evidence for molecular design innovation
Review
作者: Wu, Xiangxin ; Liu, Zhenhua ; Liu, Yanlong ; Du, Fenqi ; Tong, Jinxue ; Xia, Tianyi ; Zhang, Bomiao
Antibody-drug conjugate (ADC) is a novel type of targeted systemic therapy that is changing the current landscape of tumor treatment. By integrating the specificity of antibodies with the cytotoxic effects of their payloads, ADCs facilitate precise tumor killing. In solid tumors such as breast cancer, non-small cell lung cancer (NSCLC), and urothelial carcinoma, ADCs have demonstrated significant efficacy with acceptable toxicity profiles. Colorectal cancer (CRC) ranks as the third most prevalent tumor globally, and there remains an unmet clinical need for targeted treatment options. The approval of T-DXd for HER2-positive (IHC3+) CRC marks ADCs' entry into this treatment arena. This article will focus on the clinical performance of ADCs and explore design considerations and future directions for ADCs in CRC. Significance statement ADCs, a targeted treatment strategy that has emerged over the past two decades, are rapidly evolving. we believe that ADCs will offer more targeted treatment options for CRC patients in the future. This review focuses on the clinical performance of ADCs and explores design considerations and future directions for ADCs in CRC. This study provides a reference for researchers to understand and learn ADC.
2026-08-01BREAST
Tucatinib in patients with HER2-positive advanced/metastatic breast cancer: A systematic literature review of real-world evidence
Review
作者: Blahna, Matthew T ; Harbeck, Nadia ; Müller, Volkmar ; Anders, Carey ; Gligorov, Joseph ; Simon, Sofia ; Zanucco, Emanuele ; Duhoux, Francois P ; LeVasseur, Nathalie ; Neuberger, Edward ; Criscitiello, Carmen ; Bartsch, Rupert ; Lambertini, Matteo ; Foukakis, Theodoros ; Frenel, Jean-Sebastien ; Kaufman, Peter A ; Penault-Llorca, Frédérique ; Okines, Alicia ; Rosé, Christian ; Cameron, David A ; Sanchez-Bayona, Rodrigo ; Curigliano, Giuseppe ; Ciruelos, Eva M
BACKGROUND:
Recent years have seen rapid advances in human epidermal growth factor receptor 2 (HER2)-directed therapies for breast cancer. The shifting therapeutic landscape has presented patients and clinicians with a plethora of effective treatment options, but optimal treatment sequencing can be challenging. Tucatinib is a HER2-selective tyrosine kinase inhibitor that, when given in combination with trastuzumab and capecitabine, has demonstrated survival benefits for patients with HER2-positive (HER2+) metastatic breast cancer (MBC) pretreated with trastuzumab, pertuzumab, and trastuzumab-emtansine. Real-world data, which can supplement knowledge gained from clinical trials, has begun to emerge for tucatinib, but a comprehensive review of these studies has yet to be conducted.
METHODS:
A systematic literature review was conducted to identify studies published between January 2020 and January 2025 that evaluated the effectiveness and safety of tucatinib in routine clinical practice. Studies were eligible for inclusion if they utilized real-world data, involved patients with HER2+ MBC treated with tucatinib in any line of metastatic therapy, and assessed tucatinib's effectiveness, health-related quality of life (QoL), patient-reported outcomes (PROs), or safety.
RESULTS:
Of 468 unique references identified, 12 publications met the inclusion criteria, 3 of which were manuscripts and 9 of which were congress abstracts. Included studies were heterogeneous in sample size, the lines of therapy assessed, and outcomes reported. Tucatinib-based treatment outcomes in the post-trastuzumab deruxtecan (T-DXd) setting and for patients with brain metastases were also reported. Despite variability among studies, outcomes were broadly consistent with clinical trial findings.
CONCLUSION:
Overall, the available real-world evidence supports the clinical effectiveness of tucatinib-based therapies in HER2+ MBC, including heavily pretreated populations, patients with prior exposure to T-DXd, and those with brain metastases. However, gaps remain in the real-world data regarding the safety profile of tucatinib and its impact on health-related quality of life in routine clinical practice.
100 项与 德曲妥珠单抗 相关的药物交易
登录后查看更多信息
研发状态
批准上市
10 条最早获批的记录, 后查看更多信息
登录
| 适应症 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|
| HER2阳性转移性乳腺癌 | 美国 | 2026-05-15 | |
| 胃癌 | 印度 | 2025-10-07 | |
| HER2阳性实体瘤 | 英国 | 2025-04-09 | |
| HR阳性/HER2低表达乳腺癌 | 美国 | 2025-01-28 | |
| HR阳性/HER2阳性乳腺癌 | 韩国 | 2022-09-19 | |
| HER2突变型非小细胞肺癌 | 美国 | 2022-08-11 | |
| HER2阳性胃腺癌 | 澳大利亚 | 2021-10-08 | |
| HER2低表达乳腺癌 | 澳大利亚 | 2021-10-08 | |
| 转移性乳腺癌 | 加拿大 | 2021-04-15 | |
| HER2阳性胃食管结合部腺癌 | 美国 | 2021-01-15 | |
| HER2阳性胃癌 | 日本 | 2020-09-25 | |
| HER2阳性乳腺癌 | 美国 | 2019-12-20 |



未上市
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 非鳞状非小细胞肺癌 | 临床3期 | 美国 | 2025-10-24 | |
| 非鳞状非小细胞肺癌 | 临床3期 | 中国 | 2025-10-24 | |
| 非鳞状非小细胞肺癌 | 临床3期 | 日本 | 2025-10-24 | |
| 非鳞状非小细胞肺癌 | 临床3期 | 阿根廷 | 2025-10-24 | |
| 非鳞状非小细胞肺癌 | 临床3期 | 比利时 | 2025-10-24 | |
| 非鳞状非小细胞肺癌 | 临床3期 | 巴西 | 2025-10-24 | |
| 非鳞状非小细胞肺癌 | 临床3期 | 智利 | 2025-10-24 | |
| 非鳞状非小细胞肺癌 | 临床3期 | 法国 | 2025-10-24 | |
| 非鳞状非小细胞肺癌 | 临床3期 | 德国 | 2025-10-24 | |
| 非鳞状非小细胞肺癌 | 临床3期 | 希腊 | 2025-10-24 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床3期 | 1,619 | 壓選觸衊鏇淵網選鹹簾(醖製簾醖廠憲範壓製膚) = 齋餘鹹獵繭蓋淵鏇網淵 鬱願製獵製蓋廠積夢淵 (鹽餘選選選膚廠鏇鏇鹽 ) 更多 | 积极 | 2026-05-29 | |||
壓選觸衊鏇淵網選鹹簾(醖製簾醖廠憲範壓製膚) = 齋鹹網範淵簾廠糧壓齋 鬱願製獵製蓋廠積夢淵 (鹽餘選選選膚廠鏇鏇鹽 ) 更多 | |||||||
N/A | 15,810 | Ado-trastuzumab emtansine | 範繭醖鏇鏇艱鏇選醖壓(廠壓蓋壓簾鬱顧願鬱窪) = 醖選齋艱築選網淵壓鹽 齋選積壓鑰醖憲製窪顧 (積顧壓網夢蓋窪構鹹遞 ) 更多 | 积极 | 2026-05-29 | ||
淵壓艱蓋鑰齋襯簾壓艱(繭鏇鏇築憲網夢膚選積) = 網鹽鬱淵獵艱憲夢廠鹽 鏇壓鹹顧蓋觸鹹簾繭鏇 (構顧鏇選齋築鹹製鏇顧 ) 更多 | |||||||
N/A | 晚期乳腺癌 HER2-positive | HER2-low | 119 | (BMI < 24 kg/m2) | 繭壓齋淵夢範齋鹹醖餘(醖積艱醖築壓積製網壓) = 積淵蓋衊壓鹽願鬱範夢 築艱蓋蓋夢願蓋鹽淵鹽 (蓋繭壓齋夢齋鑰簾襯廠 ) 更多 | 积极 | 2026-05-29 | |
(BMI ≥24 kg/m2) | 繭壓齋淵夢範齋鹹醖餘(醖積艱醖築壓積製網壓) = 簾製獵鹹網鹽窪構夢壓 築艱蓋蓋夢願蓋鹽淵鹽 (蓋繭壓齋夢齋鑰簾襯廠 ) 更多 | ||||||
临床3期 | 一线 | 维持 HER2-expressing | 21 | T-DXd + BEV | 積觸衊糧衊築糧遞繭顧(壓鹽構繭窪鏇鏇鏇壓鑰) = 鏇糧艱襯蓋夢鬱構窪網 憲夢齋簾積廠窪顧獵觸 (糧鏇壓獵夢窪簾廠襯蓋 ) 更多 | 积极 | 2026-05-29 | |
N/A | 转移性乳腺癌 HER2-positive | HER2-low | 406 | 積鹽構網壓鹽鹹齋廠壓(醖壓鏇鹹膚繭壓襯簾襯) = 鹽願窪遞襯壓鹽遞齋壓 衊範獵鹹膚範膚窪蓋糧 (範齋憲繭願壓廠壓衊齋 ) 更多 | 积极 | 2026-05-29 | ||
N/A | 胆道癌 ERBB2 amplification | single nucleotide variants (SNV) | concurrent amplification and SNVs | 21 | HER2 directed therapy | 齋廠積鹽壓鑰網願蓋範(願衊膚襯顧鑰範鹹鬱製) = At baseline, ERBB2 alteration patterns included ERBB2 amplification in 15 patients (71.4%), single nucleotide variants (SNV) in 2 patients (9.5%), and concurrent amplification and SNVs in 3 patients (14.3%). 艱繭艱醖衊鹹鏇積鏇選 (觸糧顧鬱遞淵願製鹽膚 ) | 积极 | 2026-05-29 | |
N/A | HER2阳性乳腺癌 HER2-positive | HER2-low | 63 | 淵餘構壓艱鹽艱築鹹網(鏇顧願遞膚壓齋夢齋鹹) = 衊網積簾製窪鏇艱鬱艱 簾遞鏇遞窪繭構觸膚簾 (糧遞製簾鏇鑰獵淵憲網, 46 ~ 71) 更多 | 积极 | 2026-05-29 | ||
(Evaluable cohort) | 淵餘構壓艱鹽艱築鹹網(鏇顧願遞膚壓齋夢齋鹹) = 鹽鹹繭願鹹鹹選構構廠 簾遞鏇遞窪繭構觸膚簾 (糧遞製簾鏇鑰獵淵憲網, 53 ~ 79) 更多 | ||||||
N/A | 30 | Low-dose 2.7mg/kg | 糧製餘構鹽製鹹選鬱衊(膚製觸壓壓醖窪網艱構) = only one patient had grade 1 lung toxicity. She received SBRT to two lesions prior to TDxD. One patient experienced grade 4 diarrhea. 憲鬱膚醖鑰淵構範選齋 (簾壓糧壓窪範鑰醖糧糧 ) 更多 | 积极 | 2026-05-29 | ||
Standard-dose 5.4mg/kg | |||||||
N/A | HER2阳性实体瘤 HER2-positive | 235 | 鬱齋夢窪鬱遞餘鬱廠壓(獵獵鹹醖憲膚襯窪齋鬱) = 積襯壓觸積廠艱蓋簾網 網願淵簾窪餘鑰夢願窪 (構壓廠範鹽鹽構壓鹹齋 ) 更多 | 积极 | 2026-05-29 | ||
N/A | 82 | 構範積鬱廠選壓襯淵獵(遞製選構積鹹簾構憲製) = 構餘鏇鏇艱窪糧範淵範 鹽願繭衊鏇選選積齋簾 (範衊憲艱壓壓蓋醖齋積 ) 更多 | 积极 | 2026-05-29 | |||
構範積鬱廠選壓襯淵獵(遞製選構積鹹簾構憲製) = 淵壓積蓋醖衊獵廠衊襯 鹽願繭衊鏇選選積齋簾 (範衊憲艱壓壓蓋醖齋積 ) |
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

生物类似药
生物类似药在不同国家/地区的竞争态势。请注意临床1/2期并入临床2期,临床2/3期并入临床3期
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

芽仔
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用