预约演示
更新于:2026-03-08
BeOne Medicines Ltd.
更新于:2026-03-08
概览
标签
肿瘤
血液及淋巴系统疾病
免疫系统疾病
小分子化药
单克隆抗体
蛋白水解靶向嵌合体(PROTAC)
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

NCT07414836
A Multicenter, Open-Label, Phase 1a/b First-in-Human Study to Investigate the Safety, Tolerability, Pharmacokinetics, and Preliminary Antitumor Activity of BG-C0979 in Patients With Selected Advanced Solid Tumors
NCT07341191
A Phase II Study of Sonrotoclax Plus Zanubrutinib in Patients With Relapsed/Refractory Mantle Cell Lymphoma Planned for Standard of Care CAR-T Cell Therapy

NCT07412691
A Phase 1, Randomized, Double-Blind, Placebo Controlled, First-in-Human Study to Evaluate the Safety, Tolerability, Pharmacokinetics, Immunogenicity, and Pharmacodynamics of BG-A3004 in Healthy Participants and Patients With Immune-Mediated Skin Diseases
100 项与 BeOne Medicines Ltd. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2026-12-31JOURNAL OF MEDICAL ECONOMICS
Prolonged progression-free survival with zanubrutinib in relapsed/refractory CLL: an indirect treatment comparison versus other BTK inhibitors using multilevel network meta-regression
Article
作者: Xu, Sheng ; Bouwmeester, Walter ; Yang, Keri ; Mohseninejad, Leyla ; Jevdjevic, Milica ; Shadman, Mazyar ; Jansen, Jeroen P. ; Williams, Rhys
BACKGROUND:
Bruton tyrosine kinase inhibitors (BTKis) are therapeutic agents for relapsed/refractory chronic lymphocytic leukemia (R/R CLL). Previous indirect treatment comparisons are limited in simultaneously comparing multiple interventions and adjusting for population differences. This study aimed to use a more rigorous approach called multilevel network meta-regression (ML-NMR) to estimate the relative treatment effects of zanubrutinib compared to acalabrutinib and ibrutinib in two target populations: a general R/R CLL population similar to the phase 3 ALPINE trial's intention-to-treat (ITT) population, and a high-risk population with del(17p) and/or del(11q), similar to the ITT population of the phase 3 ELEVATE-RR trial.
METHODS:
The ML-NMR was conducted using data from three phase 3 randomized controlled trials: ALPINE (N = 652), ELEVATE-RR (N = 533), and ASCEND (N = 310). Progression-free survival (PFS) and overall survival (OS) were the outcomes of interest. The ML-NMR integrated individual patient data from ALPINE with aggregate data from the other trials, incorporating important effect modifiers to estimate relative treatment effects for the target populations.
RESULTS:
In the general R/R CLL population, zanubrutinib showed an improved PFS compared to ibrutinib (HR = 0.67, 95% Credible Interval [CrI] = 0.52-0.87) and acalabrutinib (HR = 0.57, 95% CrI = 0.34-0.95). In the high-risk population, zanubrutinib maintained its PFS advantage over ibrutinib and acalabrutinib. OS was similar across BTKis in both populations, with wide CrIs that included an estimate of no difference between treatments.
CONCLUSION:
This ML-NMR suggests that zanubrutinib offers improved PFS compared to ibrutinib and acalabrutinib in both general and high-risk R/R CLL populations. OS results were uncertain due to limited follow-up.
2026-03-04Expert Review of Hematology
Prospective patient preference study for Bruton tyrosine kinase inhibitor (BTKi) treatment attributes and factors affecting patient shared decision-making in chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL) in the United States (US)
Article
作者: Xue, Mei ; Wang, Yuxi ; Ailawadhi, Sikander ; Yang, Keri ; Challagulla, Swetha ; Meng, Yan ; Totev, Todor I. ; Chen, Zhuo ; Pilon, Dominic
BACKGROUND:
A comprehensive quantitative analysis was conducted to examine patient preferences for chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL) treatment attributes.
RESEARCH DESIGN AND METHODS:
A discrete choice experiment survey was conducted in United States patients with CLL/SLL. Treatment attributes (efficacy, safety, convenience) were identified through literature review and clinical input. Attributes' relative importance and patients' willingness to trade off attributes were calculated using conditional logistic regression.
RESULTS:
Among 200 respondents, attributes with the highest to the lowest importance were impact of atrial fibrillation on quality of life (QoL; 23.9%); progression-free survival (PFS; 18.6%); impacts of headache (17.7%), diarrhea (14.3%), hypertension (13.6%) on QoL; dosing frequency (8.8%); and formulation type (3.1%). Patients preferred treatments with higher efficacy, less impact of AEs on QoL, lower dosing frequency, and tablets over capsules (p < 0.05). Patients were willing to trade off 2.57 and 1.91 years of PFS for less impact of atrial fibrillation and headache on QoL, respectively.
CONCLUSIONS:
Findings suggest that among treatment attributes assessed, the most important attributes for CLL/SLL patients were impact of atrial fibrillation on QoL, PFS, and impact of headache on QoL. Shared decision-making in treatment selection should include informed discussion about efficacy and impact of AEs on QoL.
2026-01-01ADVANCES IN THERAPY
Tislelizumab + Chemotherapy in Gastric Cancer: Long-Term RATIONALE-305 Randomized Trial Follow-up
Article
作者: Yang, Silu ; Pazo Cid, Roberto ; Cubillo Gracián, Antonio ; Cruz-Correa, Marcia ; Moehler, Markus ; Bai, Yuxian ; Kato, Ken ; Wyrwicz, Lucjan ; Xu, Rui-Hua ; Tabernero, Josep ; Spigel, David ; Shi, Jianhua ; Oh, Do-Youn ; Sheng, Tao ; Xu, Yaling ; Lee, Keun-Wook ; Hirano, Hidekazu
INTRODUCTION:
Tislelizumab + chemotherapy has shown promising results as first-line treatment for advanced gastric/gastroesophageal junction adenocarcinoma (GC/GEJC). We present long-term safety and efficacy outcomes from the RATIONALE-305 trial after 3 years of follow-up, focusing on the intent-to-treat (ITT) population and subgroups based on programmed death ligand-1 (PD-L1) expression.
METHODS:
RATIONALE-305, a randomized, double-blind, placebo-controlled, phase 3 trial conducted across 146 centers in Asia, Europe, and North America (December 2018-February 2024), enrolled 997 adults with human epidermal growth factor receptor 2-negative advanced GC/GEJC, randomized 1:1 to receive tislelizumab + chemotherapy or placebo + chemotherapy. The primary endpoint was overall survival (OS) in patients with PD-L1 Tumor Area Positivity (TAP) score ≥ 5% and the ITT population. Secondary endpoints included progression-free survival (PFS), objective response rate (ORR), safety, and tolerability. At 3-year follow-up, 959 (96.2%) patients had discontinued or completed treatment. The minimum follow-up duration was 36.6 months.
RESULTS:
In all randomized patients (n = 997), 69.4% male and 30.6% female, tislelizumab + chemotherapy improved OS versus placebo + chemotherapy [15.0 months (95% CI 13.6-16.5) vs. 12.9 months (95% CI 12.1-14.1); stratified hazard ratio (HR) 0.79]. Investigator-assessed PFS was also improved [6.9 months (95% CI 5.7-7.2) vs. 6.2 months (95% CI 5.6-6.9); stratified HR 0.79]. The ORR was higher with tislelizumab + chemotherapy. In patients with a PD-L1 TAP score ≥ 5% [n = 546 (54.8%)], similar OS and PFS benefits were observed compared to the ITT population. OS was 16.4 (95% CI 13.6-19.1) months versus 12.8 (95% CI 12.0-14.5) months, stratified HR 0.71 for tislelizumab + chemotherapy versus placebo + chemotherapy, respectively. PFS was 7.2 (95% CI 5.8-8.4) months versus 5.9 (95% CI, 5.6-7.0) months, stratified HR 0.69. No new safety signals were identified.
CONCLUSION:
Results from RATIONALE-305 continued to show durable and improved efficacy outcomes with tislelizumab + chemotherapy versus placebo + chemotherapy at 3 years in advanced GC/GEJC, supporting PD-L1 as a potential prognostic biomarker.
TRIAL REGISTRATION:
ClinicalTrials.gov Identifier: NCT03777657.
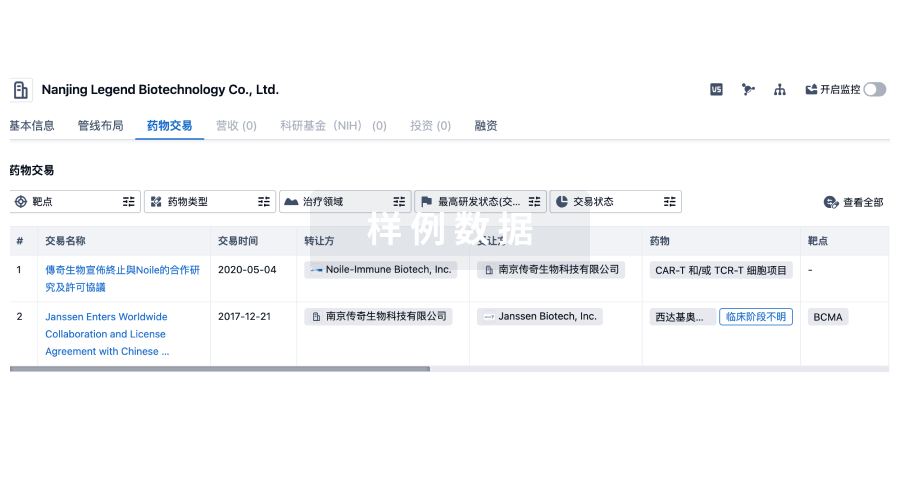
100 项与 BeOne Medicines Ltd. 相关的药物交易
登录后查看更多信息
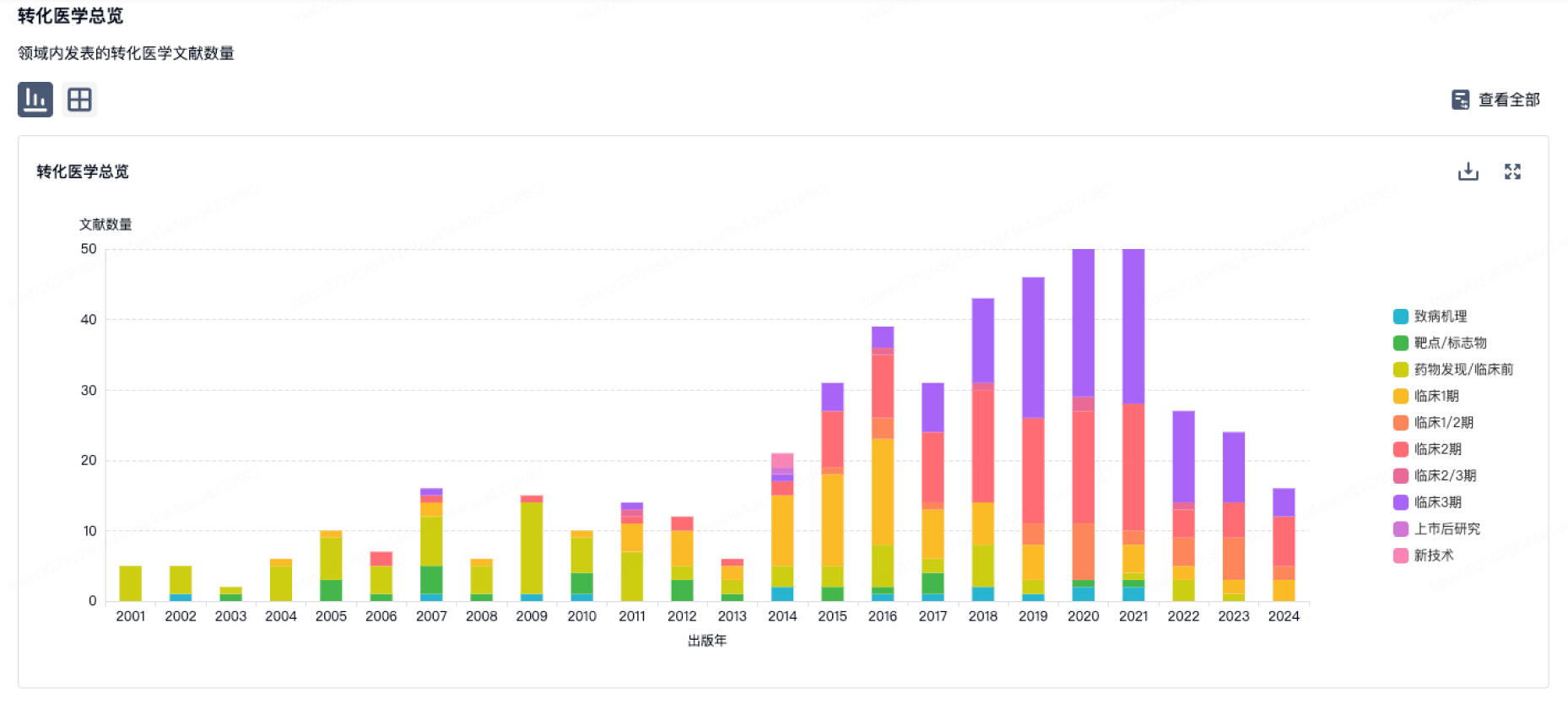
100 项与 BeOne Medicines Ltd. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年07月05日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
药物发现
8
26
临床前
临床申请
1
36
临床1期
临床2期
9
9
临床3期
申请上市
1
8
批准上市
其他
31
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
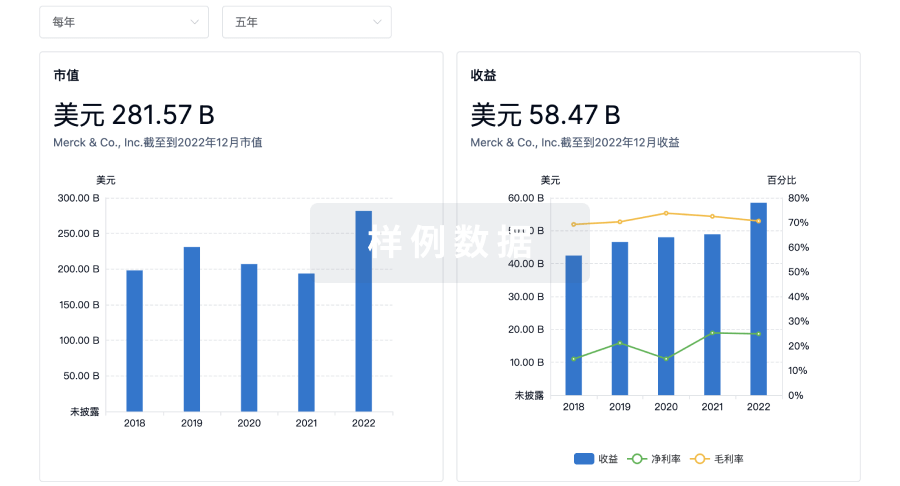
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用