预约演示
更新于:2026-04-12
Bayer AG
更新于:2026-04-12
概览
标签
肿瘤
心血管疾病
泌尿生殖系统疾病
小分子化药
Fc融合蛋白
单克隆抗体
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
NCT07389980
Prospective Trial of the Efficacy and Safety of a Personalized Regimen of High-dose Aflibercept 8mg on Treatment-naive Polypoidal Choroidal Vasculopathy: the PALLAS Trial
NCT05900388
Xarelto Paediatric VTE PASS Drug Utilization Study: An Observational, Longitudinal, Multi-source Drug Utilization Safety Study to Evaluate the Drug Use Patterns and Safety of Rivaroxaban Oral Suspension in Children Under Two Years With Venous Thromboembolism
NCT05477953
Observational Pregnancy Safety Study of Women Exposed to Nifurtimox During Pregnancy to Describe the Risk of Pregnancy and Maternal Complications and Other Events of Interest on the Developing Fetus, Neonate, and Infant
100 项与 Bayer AG 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2026-06-01Cancer Epidemiology
Accuracy of diagnostic codes to identify metastatic prostate cancer in medicare claims database
Article
作者: Zhou, Bo ; Sambamoorthi, Usha ; Sambamoorthi, Nethra ; Zhang, Yifan ; Raval, Amitkumar D
PURPOSE:
To assess the accuracy of claims-based identification of metastatic prostate cancer (mPC) compared to Surveillance, Epidemiology, and End Results (SEER) registry classification as the gold standard using the SEER-Medicare database.
METHODS:
This retrospective cohort study (N = 72,840) included men aged ≥ 66 years at SEER-recorded PC diagnosis between 2016 and 2019, and continuously enrolled in Medicare fee-for-service Parts A and B for at least 2 months before and after the SEER-recorded PC diagnosis date. Claims-based mPC was identified using the International Classification of Diseases (ICD)-10 diagnosis codes. Using registry-based mPC as a gold standard, accuracy measures were estimated for claims-based mPC. Multivariable logistic regression was used to identify factors associated with discordance between registry-based and claims-based mPC.
RESULTS:
Overall, 9.2% (N = 6684) had registry-based mPC and 8.1% (N = 5899) had claims-based mPC at diagnosis. The claims-based method yielded an overall accuracy (95.4%) with specificity (98.0%), negative predictive value (96.9%), sensitivity (68.8%), and positive predictive value (78.0%). In adjusted logistic regression, older men (≥85 years), non-Hispanic Blacks, and those living in low socio-economic areas had higher odds of discordance.
CONCLUSIONS:
ICD-10 codes in claims data demonstrated high accuracy in identifying mPC at diagnosis among elderly men with prostate cancer, with moderate sensitivity.
2026-03-01Ophthalmology Retina
Adherence to Intravitreal Aflibercept in Neovascular Age-Related Macular Degeneration
Article
作者: Schürks, Markus ; Rech, Christine ; Lanzl, Ines ; Finger, Robert P ; Ziemssen, Focke ; Bauer-Steinhusen, Ulrike ; Machewitz, Tobias ; Wachtlin, Joachim ; Scholz, Paula ; Lommatzsch, Albrecht ; Holz, Frank G ; Lorenz, Katrin
PURPOSE:
The ANDROMEDA (intravitreal Aflibercept in Neovascular amD: an obseRvational study assessing patient relevant OutcoMes, rEal-worlD treatment pattern And effectiveness) study was planned to assess adherence to intravitreal aflibercept (IVT-AFL) 2 mg treatment over 24 months for neovascular age-related macular degeneration (nAMD) and to identify patient- and physician-related factors for nonadherence (NA) in clinical settings.
DESIGN:
Prospective, observational, noncontrolled, multicenter cohort study.
SUBJECTS:
Treatment-naïve and previously treated adult patients with nAMD under IVT-AFL treatment from 41 centers in Germany.
METHODS:
Time to first occurrence of NA was analyzed descriptively using Kaplan-Meier methods followed by a Cox model to explore the potential impact of patient- and physician-related factors on NA. Participants reported reasons for NA in standardized telephone interviews.
MAIN OUTCOME MEASURES:
Primary endpoints were time to first occurrence of and reasons for NA. Secondary endpoints included change in best-corrected visual acuity and central retinal thickness from baseline to months 4, 12, and 24.
RESULTS:
The median time to first NA was 180 days in the 509 study participants (mean age: 77.2 years; 57.2% female). Among them, 44.0% were treatment-naïve, 22.6% were previously treated with IVT-AFL, and 33.4% were previously treated with other anti-VEGF agents (VEGF). Adherence rates, particularly among treatment-naïve participants, fell early and markedly: 69.6% at 4 months (95% confidence interval [CI]: 62.9%-75.3%), 53.0% at 12 months (95% CI: 46.0%-59.5%), and 40.1% at 24 months (95% CI: 33.3%-46.9%). Key risk factors for NA (hazard ratio [HR] <1 indicating a higher risk of NA for the mentioned factor, HR > 1 indicating a lower risk for the mentioned factor) included presence of any "other diseases" in the treatment-naïve cohort at baseline (HR: 0.57; 95% CI: 0.37-0.88), and patient-reported "lack of information for accompanying persons" (HR: 1.36; 95% CI: 1.03-1.79), involvement of referrals and multiple providers (HR: 0.76; 95% CI: 0.60-0.97), and "bilateral AMD" (HR: 0.73; 95% CI: 0.57-0.93) in the total cohort.
CONCLUSIONS:
In the ANDROMEDA study, key determinants of NA were comorbidities, bilateral disease, treatment by multiple providers, and a lack of patient caregiver education. Thus, better adherence may be achieved through holistic patient management, considering additional disease parameters, single-center treatment, and improved (caregiver) education.
FINANCIAL DISCLOSURE(S):
Proprietary or commercial disclosure may be found in the Footnotes and Disclosures at the end of this article.
2026-02-13ACS Infectious Diseases
Cysteine Reactivity Profiling Identifies Host Regulators of
Mycobacterium tuberculosis
Replication in Human Macrophages
Article
作者: Dix, Melissa M. ; Párraga Solórzano, Paola K. ; Gianakopoulos, Max A. ; Cravatt, Benjamin F. ; Shiloh, Michael U. ; DeMeester, Kristen E. ; Suciu, Radu M. ; Simon, Gabriel ; Neff, John K. ; Melillo, Bruno
Innate immune cells, such as monocytes and macrophages, provide the earliest defense against intracellular pathogen infection by initiating signaling pathways and restricting pathogen replication. However, the full complement of proteins that mediate cell-autonomous immunity remains incompletely defined. Here, we applied cysteine-directed activity-based protein profiling (ABPP) to map proteome-wide cysteine reactivity changes in THP-1 monocytes and primary human monocyte-derived macrophages during Mycobacterium tuberculosis (Mtb) infection. Across both cell types, we quantified 148 cysteine residues with altered reactivity. Knockdown of a subset of proteins harboring infection-induced reactivity significantly altered Mtb replication in THP-1 monocytes, linking proteins with reactive cysteines to antimicrobial defense. These data define previously unrecognized host protein changes during Mtb infection and provide a resource for investigating post-translational events that regulate innate immune responses to intracellular bacteria.
100 项与 Bayer AG 相关的药物交易
登录后查看更多信息
100 项与 Bayer AG 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2026年07月05日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
药物发现
19
80
临床前
临床1期
42
22
临床2期
临床3期
7
1
申请上市
批准上市
94
460
其他
登录后查看更多信息
当前项目
登录后查看更多信息
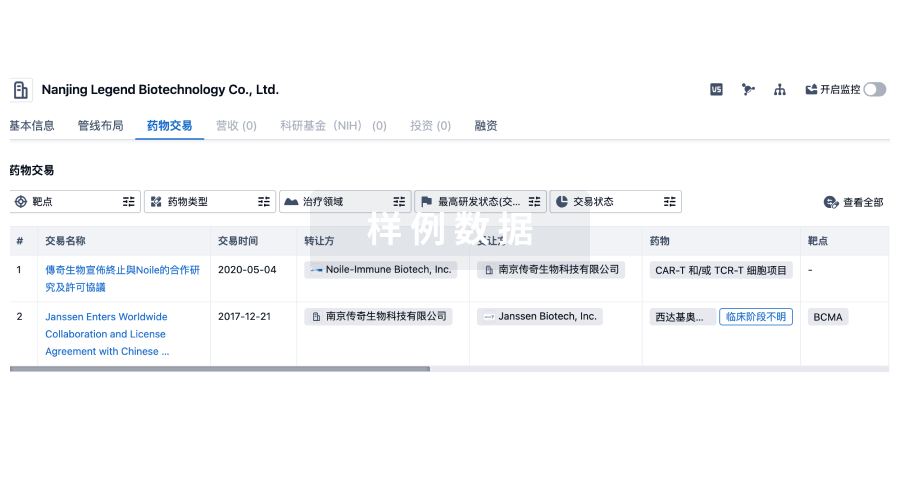
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
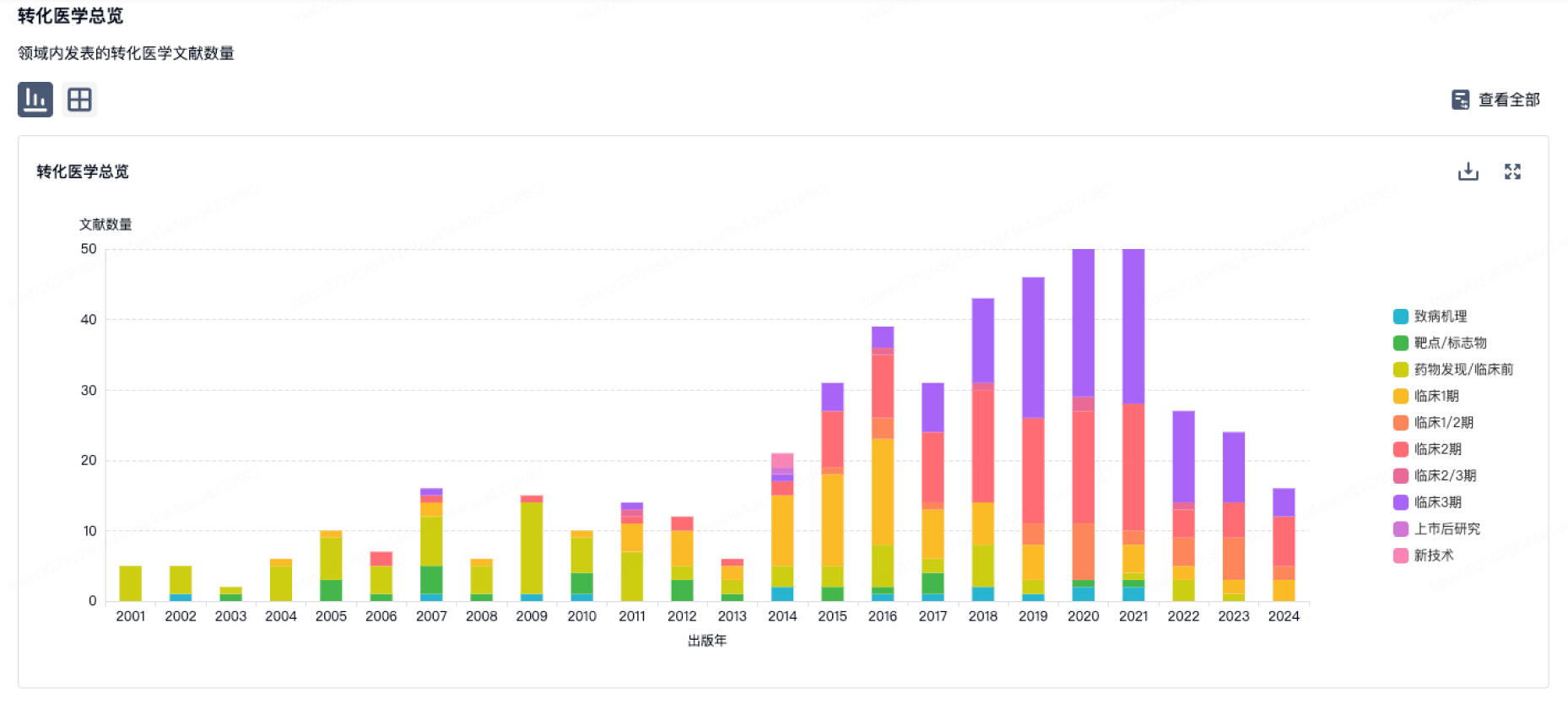
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
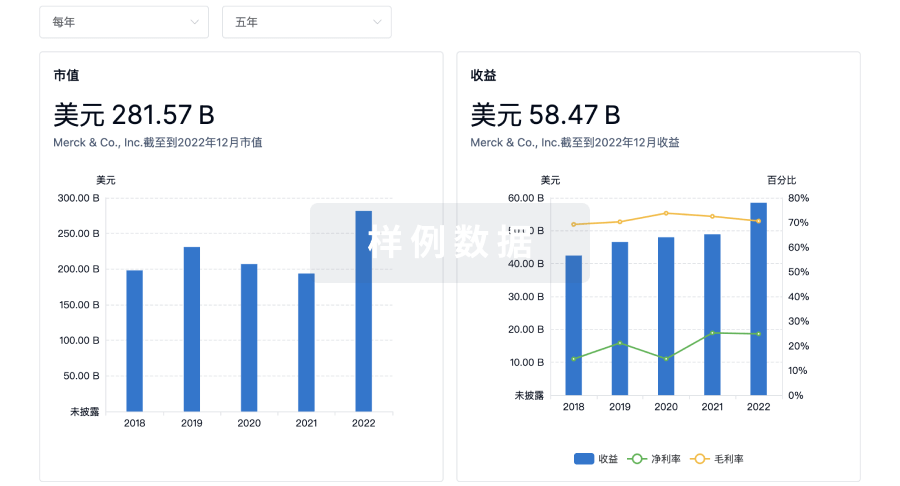
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用